
CBS news came out with an analysis this morning that most
Republican mid-term election candidates are election deniers. That is 308 out of 597 total. They agree with former President
Trump that he actually won the 2020 election, despite the fact that there is absolutely
no evidence to support that claim. The evidence is lacking even when analyzed by Republicans and judges and attorneys who are Republican appointees. When
that claim is reported in the news these days it is characterized as a lie. Even
apart from the news media, the January
6th Committee has presented direct evidence that this claim was
inaccurate and had no supporting evidence and that it also formed the basis for the coordinated attack on the Capitol and an attempt by former President Trump and his
associates to overthrow the newly elected government of the United States.
What should be most concerning for any citizen of the
United States is that attempted insurrection. There is a good chance that if
the current crop of Republican candidates – most of whom are overt election
deniers become the majority in the House that former President Trump and his
associates will not be held accountable for this action. That is unprecedented
in any democracy and it flaunts the rule of law and political convention of the
United States. If the insurrection had succeeded – the United States as we know
it would cease to exist. Democracy instead would be replaced by a Republican party
of moral and gun extremists.
Instead of focusing on preserving the Republic – voters seem focused on the economy and inflation – as though any group of politicians has a more favorable history in that area. Over the course of my lifetime, we have had worse inflation, much worse unemployment, 10 recessions, 2 economic crises that nearly collapsed the world economy, and 30 yr fixed mortgage rates at least twice as high as they are now. The people who saved the economy were professional economists from the Federal Reserve who are appointed and not elected officials. Elected officials consistently have the opportunity to pass legislation to reduce financial market risk due to speculation, but they seem to lose interest every time one of these crises has passed. In this case both inflation and the possible recession can be explained by historical events (pandemic, Russian invasion of Ukraine) affecting the supply side and driving up prices. Rising interest rates to decrease demand and reduce inflation have made increased the cost of borrowing and that comes following a long period of artificially low interest rates that included low interest rates for savings accounts. In some cases, money market and bond funds were paying negative interest.
I present the following graph as economic evidence. It is not exhaustive but it illustrates my point. I thought about adding a timeline of Federal Reserve Chairs but ran out of time. The national debt increases substantially under all presidents. The recessions are the shaded areas. Major crises in the economy occurred with the Savings and Loan Crisis (1982-1989), Long Term Capital Management liquidation (1998) and the Subprime Mortgage Crisis of 2007-2010. The graph extends to August of 2022 with unemployment at 3.5% and Sticky Price Consumer Price Index of 6.39%. Republican politicians are saying this is the highest inflation rate in 40 years. What they are not saying is that it is also the highest rate of corporate profits in 70 years and the Federal Reserve has made interest rate increases that are already taking effect in the housing market. (click to enlarge)

I say that the voters seem focused on the economy because it is hard to get valid news about voter preferences from major networks focused on either balancing one party against the other (when no such symmetry exists) or acting essentially like the public relations department of the Republican party. Viewers used to be able to turn on the news and watch reliable journalists deliver the facts, but now they have a choice to listen to a broadcaster who parrots their political ideology. The facts take a distant second place. There is no clearer example than election denial and all of its ugly correlates like voter suppression and political violence.
There is only one party that has multiple members endorsing both of those
options. To listen to some of those
candidates today – they make it seem like the opposition party has similar
problems. There were no Democrats advocating for the violent overthrow of the
US government. There were no Democrats
addressing violent groups and suggesting that they “stand by”. There were no Democrats writing and passing permitless carry gun laws at a time when gun homicides and suicides are high and
school shootings continue unabated. There
were no Democrats passing laws that allow heavily armed men wearing body armor and
carrying assault weapons to gather in proximity to a
legislative body and intimidate them. There is no symmetry between parties on
the issue of political violence, gun violence, and the orderly transitions between elections.
I could continue but realize that this scarcely read blog
and the lateness of this post will probably not change much. I will end by
posting what I consider the top issues to be in order of importance. I have
posted before that I am a long time small “i” independent but in the current
Constitutional Crisis I don’t have much of a choice and I have already voted.
The vote I cast last week required 2 forms of ID, my address had to be
confirmed in an electronic database and I had to sign a registry and one of the
two envelopes containing my paper ballot.
That sealed paperwork was directly observed and signed off by an election
worker. This is what I voted on:
1: Preservation of
American Democracy. No insurrection against the government can stand and none
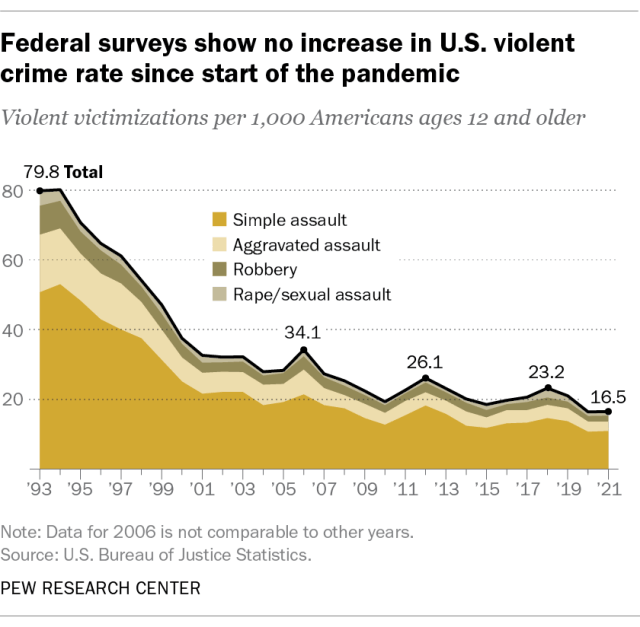
of the conspirators should go unpunished. Any party claiming to be the Law and Order party should understand this. That party is trying to make crime an issue and it is hard to say if the media or the GOP is the reason for this focus - but the reality is that there has not been an increase in violent crime and there has been a 30 year trend in a positive direction.
2: Voter Rights.
The Big Lie about the 2020 election was a variation of the big lie about
election problems in the United States.
That lie is used to restrict access to voters and make it more difficult
for citizens to cast their ballot. Lower income Americans are disproportionately
affected. A variation on that theme is intimidating voters and election officials. That is an ongoing process and it is encouraged by politicians spreading the Big Lie about both the election process and the integrity of the voting process. There is no evidence that either has been compromised.
3: Civil Rights. The unprecedented attack on Roe at the level
of the Supreme Court is really the culmination of Republican activism dating
back to the Carter administration. At the time a Republican activist convinced fundamental
Christians that they should be politically interested in the abortion issue and
it was used to attempt
to protect school segregation. They created one of the most divisive issues
in American politics to advance their interests and made it seem like it was a
religious issue. This is a doubling down of moral extremism. In other words moral superiority to cover an essentially immoral act. There are not many positions that are more cynical.
4: Gun Regulation. Gun carnage continues unabated and the
GOP and their justices in the Supreme Court have no reservations about allowing
it to continue. Republicans everywhere are rationalizing
it as a problem with mental illness, when the prevalence of mental illness is
the same across all countries and only the United States has mass shooters
shooting children on a regular basis, gun homicide as a leading cause of death
in children and young black men, and extremely high levels of gun homicides and
suicides. There are currently 25 states
that allow permitless concealed carry of firearms. All of this from a politicized reading of the archaic language of the Second Amendment. That alone would probably not be enough. It also takes the fear tactic that the "government", "liberals", etc are "coming for your guns." The reality is that there are so many weapons in the country - finding them and rounding them up would be an impossible task for anyone. And of course - nobody is interested in doing that.
5: Strengthening NATO. The Biden administration has handled the
crisis in Europe and rebuilding the NATO alliance expertly and they are not
getting nearly enough credit. A secondary goal should be containing terrorism with
our allies that comes in all forms including state terrorism that we are witnessing from Russia, North Korea, and Iran. It is likely there would be a much different outcome under a Trump administration.
5: Nuclear
non-proliferation: Every possible effort must be made to ensure that nuclear
weapons are not used again. There is too much loose talk about how limited tactical nuclear weapons would release less radiation and that a small local nuclear war would be "winnable" by somebody. Climate change should be a wake up call illustrating that even small changes in the environment can lead to catastrophic global changes. The detonation of nuclear weapons will not determine winners and losers. Mankind will lose and civilization will end.
6: Climate
Activism: As climate change gets more
and more obvious the party that denied it was happening clearly has no
solutions. The infrastructure bill
passed by the Biden administration was a major step in the right direction but
even that is not enough. More changes need to follow to reduce carbon
dioxide emissions and remove permanent environmental contaminants from the
environment.
7: Social
programs. There are Republican
legislators who want to cancel Social Security and Medicare or euphemistically
review it every 5 years and decide whether or not to cancel it. Every person who has paid into those programs needs
to be assured that they will get the agreed upon benefits. Republicans use socialist rhetoric to impress
upon their followers that the “socialists” want to take over the government and
restrict their freedom. In fact, social
democracies are some of the fairest systems in the world and the United States
has had social programs for a long time. Social programs in a democratic republic
have nothing to so with a socialist government.
8: Public health Initiatives:
COVID-19 denialism was a major factor in unnecessary mortality and morbidity
from that pandemic and there is no doubt who the most significant players in
that denialism were. As the climate deteriorates and mankind is in closer proximity
to millions of novel viruses in the wild – we need to infrastructure to assess
those threats and either contain them or treat the outbreaks. We need people
who understand science as a process and what needs to happen in this area. Instead we have Republican politicians bragging about ignoring public health measures.
9: A Coherent
Immigration Policy: Building walls and playing
games with the lives of undocumented immigrants is not a coherent policy. It
will take more comprehensive planning and aid to countries in Central and South
America. In addition the United States has a lower percentage of foreign born citizens than many European countries and Canada as well as a labor shortage so that increasing the number of legal immigrants each year can potentially decrease the number of people seeking political asylum.
10: Simplified Tax
Policy: Taxes are always a political football.
Promise of no new taxes and tax cuts are not realistic, especially
considering the current national debt. A
better plan is to make taxes more transparent and easier to complete. Business
taxes should not be eliminated and should be consistent year-to-year and not a
disincentive to doing business in the United States.
That is what I voted on. It does not come down to a single
issue for me. It does not come down to voting for myths rather than reality.
But it does come down to a single party.
George Dawson, MD, DFAPA









