Four years ago, I commented on a prediction that the era of
“blockbuster drugs” in psychiatry would soon be over. That designation is used
for medications that generate $1 billion in sales per year. Even at the time of
my original comment, most of the drugs prescribed by psychiatrists were
generic drugs that were often very inexpensive. The example that I frequently
refer to is the antidepressant citalopram that was available for four dollars
per month.
Last week PharmaCompass,
a drug industry analytic and service company came out with a list of the top
100 drugs by sales in that industry. They listed the top 30 drugs by sales and their
website lists the top 500 drugs with additional metrics such as whether or not
sales are increasing or decreasing and by the percentage. There were no
psychiatric drugs in the top 30. Lyrica or pregabalin, a drug used primarily
for neuropathic pain and fibromyalgia came in at number 16 and generated $4.6
billion in sales. Some consider it to have a tertiary indication for anxiety
but I would not consider it to be a drug primarily for psychiatric
applications.
Sales
Position
|
Company / Companies
|
Product Name
|
Active Ingredient
|
Main Therapeutic Indication
|
2018 Revenue in US$ billion
|
1
|
AbbVie Inc., Eisai
|
Humira®
|
Adalimumab
|
Autoimmune Disorder
|
20.47
|
2
|
Bristol Myers Squibb, Pfizer
|
Eliquis
|
Apixaban
|
Cardiovascular Diseases
|
9.87
|
3
|
Celgene
|
Revlimid
|
Lenalidomide
|
Oncology
|
9.69
|
4
|
Bristol Myers Squibb, Ono Pharmaceuticals
|
Opdivo
|
Nivolumab
|
Oncology
|
7.57
|
5
|
Amgen, Pfizer, Takeda
|
Enbrel
|
Etanercept
|
Immunology
|
7.45
|
6
|
Merck & Co.
|
Keytruda
|
Pembrolizumab
|
Oncology
|
7.17
|
7
|
Roche
|
Herceptin
|
Trastuzumab
|
Oncology
|
7.05
|
8
|
Roche
|
Avastin
|
Bevacizumab
|
Oncology
|
6.92
|
9
|
Roche
|
Mabthera/ Rituxan
|
Rituximab
|
Oncology, Immunology
|
6.82
|
10
|
Bayer, Johnson & Johnson
|
Xarelto
|
Rivaroxaban
|
Cardiovascular Diseases
|
6.58
|
11
|
Bayer, Regeneron
|
Eylea
|
Aflibercept
|
Ophthalmology
|
6.55
|
12
|
Johnson & Johnson, Merck & Co., Mitsubishi Tanabe
|
Remicade
|
Infliximab
|
Autoimmune Disorders
|
6.44
|
13
|
AbbVie, Johnson & Johnson
|
Imbruvica
|
Ibrutinib
|
Oncology
|
6.21
|
14
|
Pfizer
|
Prevnar 13/ Prevenar 13
|
Pneumococcal 7-Valent Conjugate
|
Vaccine
|
5.80
|
15
|
Johnson & Johnson, Mitsubishi Tanabe
|
Stelara
|
Ustekinumab
|
Immunology, Dermatology
|
5.25
|
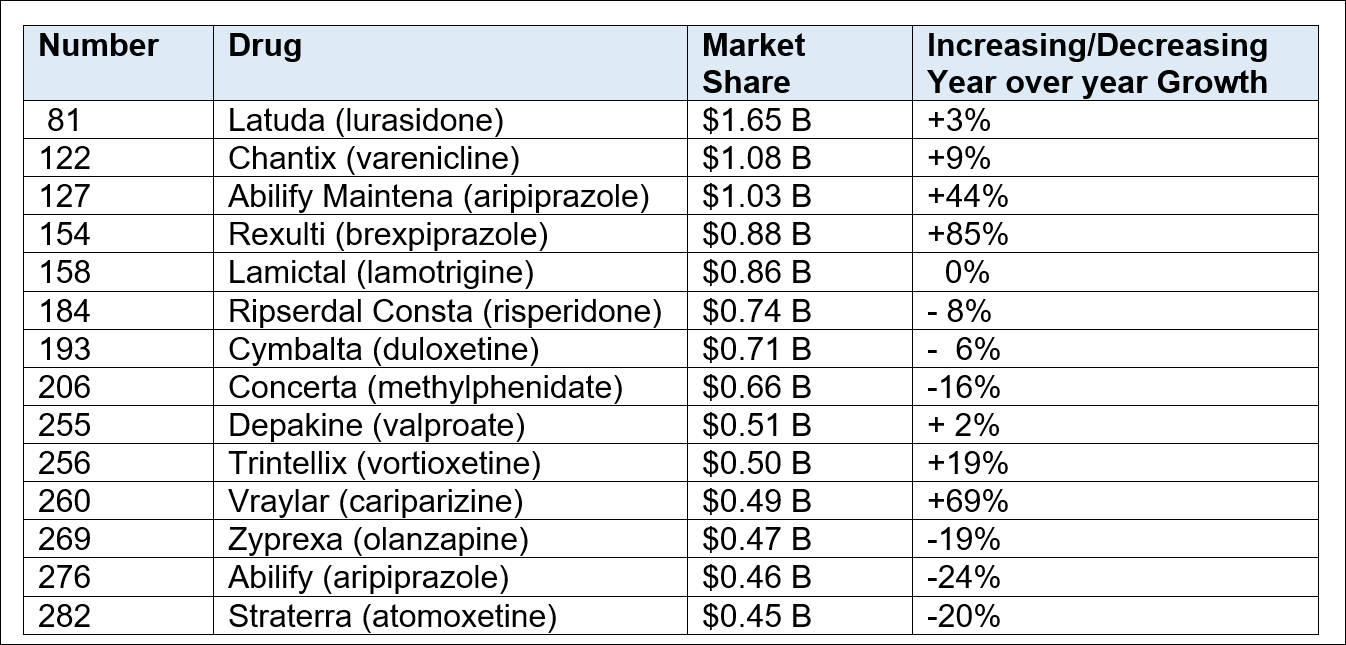
Medications for neurological and mental disorders had a total market share of $55.8 billion or 10.2% of the entire market. There were only three medications that would qualify as blockbuster drugs and being used by significant numbers of psychiatrists and they included Latuda (lurasidone), Chantix (varenicline), and Abilify Maintena (aripiprazole). The blockbuster drugs listed are all concentrated in a few specialties. Several are from the same class. For example both Eliquis and Xarelto are novel oral anticoagulants (NOACs). The total market share of the top 15 drugs greatly surpasses any amounts every attained by psychiatric medications. That makes sense because many are treating conditions that have a high prevalence and these medications generally represent an advance in pharmacotherapy.
I posted this mostly to note the trends over time.
Journalists and other commentators tend to get carried away with market snapshots. I
have not really noticed any negative commentary about the fact that the current
blockbuster drugs that have nothing to do with psychiatric disorders are
generating much more pharmaceutical company income. I also have not heard any
commentary on how there is a natural fluctuation in this market based on drug
discovery and the current rules on patent exclusivity. Many of the previous
psychiatric “blockbusters” are obviously rapidly losing market share now that
there are generic versions. I would argue that the current data also may
indicate that restrictions on current medications may be limiting their market
share.
The issue of direct to consumer advertising has typically not been discussed in these opinion pieces. I have seen Rexulti frequently in television ads. The application is generally antidepressant augmentation - accompanied by a very fast and diluted compilation of symptoms of both tardive dyskinesia and neuroleptic malignant syndrome. How much do those ads contribute to the market growth of Rexulti? My speculation is quite a lot. It would not take much for a person taking an antidepressant and not experiencing adequate relief to call their primary care physician for the addition of Rexulti. I have seen similar ads for Vraylar.
The issue of direct to consumer advertising has typically not been discussed in these opinion pieces. I have seen Rexulti frequently in television ads. The application is generally antidepressant augmentation - accompanied by a very fast and diluted compilation of symptoms of both tardive dyskinesia and neuroleptic malignant syndrome. How much do those ads contribute to the market growth of Rexulti? My speculation is quite a lot. It would not take much for a person taking an antidepressant and not experiencing adequate relief to call their primary care physician for the addition of Rexulti. I have seen similar ads for Vraylar.
Looking only at market share and pharmaceutical revenue only
provides a look at one cost of this market. There is a huge pharmaceutical
benefit manager component that generates revenue primarily by requiring their
authorization for specific medications and also packaging deals for
managed-care organizations. There is definite cost what they do but they
currently are allowed to force physicians to work for them for free.
I hope that this information allows people take a more
skeptical look at political and journalistic pieces that use pharmaceutical
sales numbers and specialty sales for one rhetorical purpose for another. I am
specifically referring to the recent good old days of the psychiatric drug “blockbusters”
where much of what was written was an indictment against psychiatry and those
psychiatrists who either worked directly for pharmaceutical companies or
received some minor perk. There was the conspiracy theory that pharmaceutical companies had influenced the DSM-5. That is both unrealistic and it greatly exaggerates the importance of that book. The data illustrates that no amount of physician
manipulation can maintain a pharmaceutical product as a “blockbuster”
independent of market forces.
Those market forces also have a significant political and regulatory component where the real conflict of interest lies. Allow me to translate that to Congress and the FDA.
Those market forces also have a significant political and regulatory component where the real conflict of interest lies. Allow me to translate that to Congress and the FDA.
George Dawson, MD, DFAPA
Graphics Credit
The top table from PharmaCompass was posted with their permission.
Disclaimer:
I had to identify and hand count the psychiatric drugs on the PharmaCompass web site from their graphic interface. It is possible that I missed some or the count is off (they were not numbered). Let me know if you detect any errors.
Disclaimer:
I had to identify and hand count the psychiatric drugs on the PharmaCompass web site from their graphic interface. It is possible that I missed some or the count is off (they were not numbered). Let me know if you detect any errors.


