“There is a widespread, rosy misconception that viruses evolve over time to become more benign. This is not the case: there is no predestined evolutionary outcome for a virus to become more benign, especially ones, such as SARS-CoV-2, in which most transmission happens before the virus causes severe disease…”
Professor of Evolution and Genomics
University of Oxford
I typically don’t like to post on a non-psychiatric topic
immediately after posting one. But the
current level of misinformation on the pandemic necessitates this. That is
obviously not because I am a big influencer with widespread readership – but I
like responding to the sea of right wing misinformation on Twitter. And today
it was all about how the response to the pandemic was an overreaction with far
reaching effects. Nothing about how the virus has killed 1.1 million Americans,
the impact of that mortality on families and businesses, the impact on the
healthcare system and its workers, and the enduring disability of millions with
long COVID. The evidence is clear that
the pandemic was mishandled early on as the Trump administration denied the
degree of the problem and then falsely reassured the public that everything was
under control. The only way the right wing can rewrite that history is to push
a false narrative that there was a conspiracy theory to prevent any
investigation of the lab leak theory, that face masks and public health
measures don’t work, that school children are irrevocably damaged from online
learning, and that all of these unnecessary measures were really an unnecessary
infringement on freedom. Unfortunately, pandemic viruses don’t work that way.
They do not really care about your political affiliation or what you read on
Twitter.
One of the popular myths during the early to mid-pandemic
was the idea of herd immunity and how by ignoring all of the public
health suggestions up to and including the immunizations (or “jabs” as they are
referred to by the right wing) the entire population would build up immunity
and the pandemic would fade away. The way that argument was typically presented
minimized any death or disability along the way. Herd immunity would happen and it would happen
quickly to resolve the problem. It also
implicitly assumed that writing off the elderly and the 10% of the population
that is immunocompromised was morally acceptable. Not much discussion of how herd immunity
would happen without immunizations – since many of the proponents were
ideologically sympathetic to the idea that public health measures and
immunization were unnecessary.
An associated concept of endemic disease cropped up
at one point. The popular usage was to
say: “This is no longer a pandemic, there are no more large outbreaks,
therefore we can declare it is an endemic like the common cold viruses.” Since this was also an ideological rather
than scientific argument – it was also a rationale for stopping all of the
suggested public health measures and getting things back to normal as soon as
possible,
That brings me to a brief essay on endemics written by
evolutionary virologist Aris Koutzourakis in Nature
(1). The title speaks for itself. His definition of endemic is straightforward
- endemic infections mean that the
infection rate is static – not rising or falling. The best intuitive example is common cold viruses – there are predictable seasonal fluctuations but the
number of viruses and the composition of the pool of common respiratory viruses
stays about the same and no one outcompetes the others. Nobody is too worried
about common cold viruses because they are not too deadly and don’t commonly
overwhelm the healthcare system.
Influenza viruses are somewhat different. Whether and epidemic or pandemic occurs
depends on an elaborate system of guessing the correct components for the
influenza vaccine and measures taken to prevent zoonotic transmission of potentially
more lethal influenzas viruses – like avian influenza. That backdrop of common
cold versus influenza viruses seems like a way to understand endemicity. It leaves out one important point and that is
endemic pathogens can also be lethal and create disability.
Dr. Koutzourakis lists several examples of endemic, but
lethal pathogens including malaria, polio, and tuberculosis. They are all significant causes of mortality
and morbidity. He successfully predicted
that unless the pandemic was stopped quickly subsequent evolving variants could
be more transmissible and difficult to treat.
That occurred with the subsequent 4 SARS-CoV-2 variants. Viral evolution has also
been observed with other pandemic viruses and the occurrence of more dangerous
variants. He analyzes the current behavioral situation correctly in the United States. Even if people are not using the word endemic –
they are generally stating that the pandemic is over and that it is time for a
return to normal. Normal typically means no public health measures like masking, social distancing, or even
deciding to stay home if you are ill.
The only place that those measures are acceptable is in a medical or
dental facility and even then they are no longer universal. To compound the problem,
the anti-public health ideologues are either bragging that they were correct
all along or actively spreading misinformation about masks, vaccines, or the
origin of the virus.
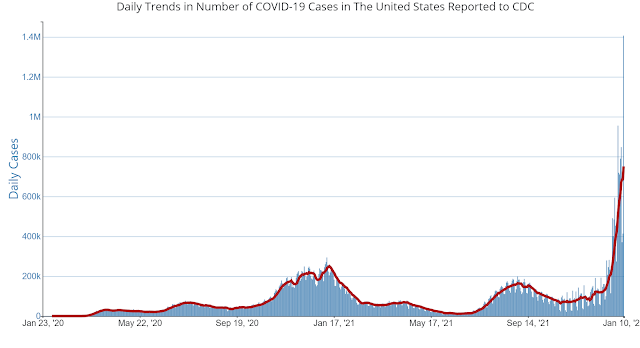
The graphic at the top of this page (click to enlarge) is taken from the CDC
web site today. Even though the area in
the red rectangle looks fairly static going back to May of 2022 – the actual
number of cases per week ranges from 170 to 900K.
That corresponds with weekly deaths 1,795 to 3,697. Dr. Katzourakis
suggests that there is the potential to see additional spikes of infection and
suggests that the direction this pandemic will take at this point depends a lot
on continued public health measures, immunizations, antiviral medication, and
individual behavior. One of the critical
aspects of science as I explained in my previous post is that scientists look
at data supporting or refuting hypotheses in terms of probabilities and also speculate
with probability statements. Viral epidemiologists and evolutionary virologists
know how viruses work and evolve. Their predictions are much more likely to be
accurate than someone with no expertise and no data. The next time you hear politicians or news
personalities talking like this pandemic is over take it as an unfounded
opinion. Do the same thing when your neighbor tells you that you don’t need to
get any more vaccinations or wear a mask in crowded places.
Don’t let ideology blind you to science.
George Dawson, MD, DFAPA
References:
1: Katzourakis A.
COVID-19: endemic doesn't mean harmless. Nature. 2022 Jan;601(7894):485. doi:
10.1038/d41586-022-00155-x. PMID: 35075305.
2: Centers for
Disease Control and Prevention. COVID Data Tracker. Atlanta, GA: US Department
of Health and Human Services, CDC; 2023, March 12. https://covid.cdc.gov/covid-data-tracker accessed on 03/12/2023
3: Callaway E.
Beyond Omicron: what's next for COVID's viral evolution. Nature. 2021
Dec;600(7888):204-207. doi: 10.1038/d41586-021-03619-8. PMID: 34876665.