There was some of the usual controversy in the media today. Is Attention Deficit~Hyperactivity Disorder over diagnosed or underdiagnosed? The usual controversy contained the usual stories of how easy it is to get a diagnosis of ADHD in some places. In some places it seems like just a matter of expense - a thousand dollar test battery. In other places there are people disabled by the condition who cannot get adequate treatment. In the meantime there are international experts cranking out reams of papers on the importance of diagnosing and treating this condition in childhood. Occasionally an article shows up in the papiers about the cardiovascular safety of these medications. And in the New England Journal of Medicine there was a paper about a higher incidence of psychosis due to these medications. Where does the reality lie?
I was fortunate enough to have worked at a substance use treatment center for about 12 years just prior to retiring. Only adults were treated at that facility. A significant number of them were diagnosed and treated as children. There were also a significant number of patients newly diagnosed as adults - some as old adults in their 60s and 70s. Whether or not ADHD can occur as a new diagnosis during adulthood is controversial and establishing a history consistent with childhood ADHD is problematic due to recall errors and biases. Secondary causes of ADHD in adults such as substance use problems and brain injuries increases in prevalence. Although I am speculating, secondary causes seem a more likely cause of attentional symptoms in adults and therefore acquired ADHD without childhood ADHD if it does exist is an entirely different problem.
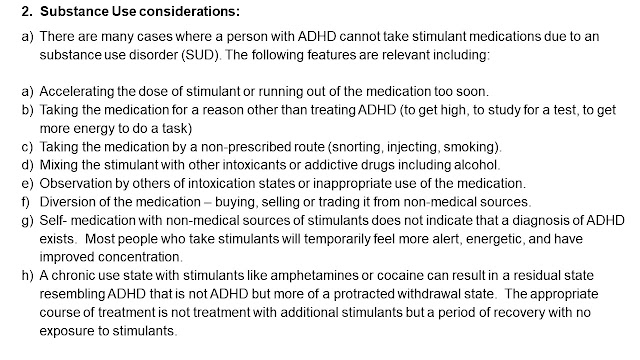
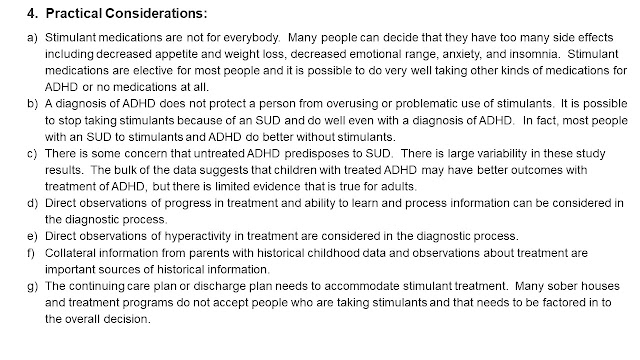
Prescribing stimulants to patients who may have stimulant use disorders is problematic for a number of reasons. Initially we had an administrative safeguard on the practice. Stimulant prescriptions could only be approved with a second opinion by another psychiatrist after reviewing the record. Eventually we had a core of psychiatrists who practiced the same way and the second opinion was no longer necessary. Over the course of 12 years I developed these discussion points. I think they are a good example of the minimum ground you need to cover in an evaluation for ADHD. I typically had a 60-90 minute time frame to work with and could see people on a weekly basis for 30 minute follow ups. These evaluations were often controversial and resulted in collateral contacts, typically with a family member who was advocating for the stimulant prescription.


I added the following slide based on polypharmacy considerations in the paper cited in reference 1. This is a common clinical problem that needs to be approached rationally and that includes limit setting on the concept that every side effect or symptom needs to be addressed by a medication rather than a medication discontinuation, reduction, or substitution. I always include a discussion of rare but serious side effects, synergistic side effects, drug interactions, interactions with comorbid medical problems and associated medications, and very serious interactions that could lead to hospitalization or death, like serotonin syndrome.
I am going to end on a note about countertransference based on a disagreement I had at a conference about my methods. The speaker advocated for prescribing stimulants as a general operating practice for anyone with ADHD. When I confronted him about the problem of substance use he claimed his motivation was that he considered it his priority to "help" people and he thought that stimulants were the most helpful medication.
Whether or not a medication is helpful for any psychiatric disorder depends on a very careful assessment and clinical expertise that considers several dimensions including the potential risks and benefits for the patient and the incorporation of the patient preferences and values into the clinical decision making process. In my evaluations, I try to sum all of that up in an informed consent discussion. In the area of ADHD evaluation and treatment, that covers a lot of ground and there is no simple uniform recommendation.
George Dawson, MD, DFAPA
Photo Credit: Many thanks to my colleague Eduardo A. Colon, MD for allowing me to use his photos.






I'm old enough to remember than even the hippies, who were generally in favor of mind-altering drugs, used to say "speed kills." I also recall docs pushing the ADHD diagnosis back when video arcades were big. They said the fact that kids with the diagnosis were observed concentrating on an arcade game for hours despite buzzers and bells going off all the time and tons of kids milling about did not prove that the kids could concentrate because "that isn't concentration." Well, I wondered, what is it then? Studies have shown that the younger kids in a class in schools with no semesters were much more likely to be given the diagnosis than the older ones. And then there's the issue of ruling out other causes of poor concentration. Another study in Palo Alto CA found that a large percentage of kids were sleep deprived.
ReplyDeleteAs a Canned Heat fan - I recall the "speed kills" message in their song "Amphetamine Annie" released in 1968. They also listed some additional symptoms of amphetamine use disorder along the way before her ultimate death. That would have occurred during the first amphetamine epidemic at the link above. Prior to the DSM "minimum brain dysfunction" was one of the diagnoses. My high school experience at the time was that learning problems of any kind were not handed well in school.
DeleteSleep disturbance is definitely in the differential diagnosis for ADHD. In outpatient practice it was common for me to trace many psychiatric complaints back to life long sleep problems that started in childhood - often as night terrors.
I remember the "minimum brain dysfunction" diagnosis as well.
ReplyDeleteAnother reason for the sleep deprivation in kids is that a lot of parents these days let their kids stay awake half the night playing video games.