"Over the past year, SAMHSA leadership with staff to establish a set of internal business strategies that will ensure the effective and efficient management of the Strategic Initiatives. The resulting Internal Operating Strategies serve as the mechanism through which SAMHSA will optimize deployment of staff and other resources to support the Strategic Initiatives. These Internal Operating Strategies (IOS)—Business Operations, Data, Communications, Health Financing, Policy, Resource Investment and Staff Development—articulate SAMHSA’s effort to achieve excellence in operations and leverage internal strengths by increasing productivity, efficiency, accountability, communications, and synergy."
Being employed at one time in a large managed care organization, I am used to seeing business speak like this. I learned to cringe when I read it because any Strategic Initiative based on business speak rather than science or clinical expertise typically ends up being a nightmare. That's just my experience, but any American who survived the last financial debacle has to be sensitized to words like "productivity, efficiency, accountability, communications, and synergy." I have a previous post on the Orwellian nature of the word accountability in case you missed it. But you can substitute any of a number of words in this paragraph - like excellence. We used to have a term in medicine called quality that actually meant something. Excellence as used in the business community is a whole new ballgame. The number of centers of excellence and top hospitals and clinics based on business measures can be astounding. You can probably drive out in your community and see one of these banners wrapped around some facility right now.
SAMHSA is supposed to be the federal government's lead agency for the treatment of mental illness and substance use disorders. There has been some debate, but I think the political strategy of SAMHSA is very clear and that is to continue the rationing and managed care tactics that have been in place for the past 30 years and make them official government policy. Lately they have been using tactics that I have seen from these companies over the past 10 years. Here is what I am seeing so far.
Consumer slogans and concepts are identified that are easy (and free) to support. Micky Nardo, MD posted their pamphlet on their working definition of Recovery . This is their "primary goal" for the next year and it was supposedly built on among other things: "consultation with many stakeholders" . The pamphlet goes on to the definition of recovery with no apparent rules for their all inclusive definition. For example, does everyone in recovery need to have all of the elements of the definition? Are there exceptions? If someone is lacking an element would we say their are not in recovery? Is this just a subjective and totally personal assessment? Or is this a goal? If so, why is the lead agency for mental health and substance use promoting it and making it a primary goal? Note the goal here is "behavioral health". Behavioral health is the managed care version of mental health. SAMHSA is therefore supporting the managed care view of the world. That world view has rationed and otherwise decimated resources available for the treatment of mental illnesses. Just a few observations on the 10 page pamphlet.
Social media is used for marketing purposes. Well it is the 21st century and this is how everybody including government agencies gets noticed these days. I got this cheery notification from SAMHSA in an e-mail this morning:

Nothing like using a standard Internet marketing strategy to discuss a process that has no proven efficacy in treating mental illness. This is the kind of marketing approach to medicine and mental illnesses that I have seen and expect to see from managed care companies. It usually happens right before they decide they will financially penalize you for NOT practicing Wellness activities. In a plan where I was enrolled each employee had to pick a Wellness activity and a counselor would call at intervals and decide if you were in fact compliant with your activity. Noncompliance meant higher premiums. In the business world wellness can cost you.
Since SAMHSA is really not a managed care company, why are they using their marketing and political strategies? The most likely explanation is the unparalleled success of managed care against physicians and other traditional health care organizations. SAMHSA seems to have surprisingly little expertise in treating significant mental illnesses. That puts them on par with most managed care companies in the US who if they are honest will flat out tell you that their job is to extract as much money as possible from subscribers who believe that they signed up for some kind of mental health or substance use benefit and send it somewhere else. That theme is repeated time and time again in corporate America and nobody would fault an American corporation with than attitude. With a government agency, especially the lead agency there should be a much higher standard than a corporate one. What is the evidence for my statement?
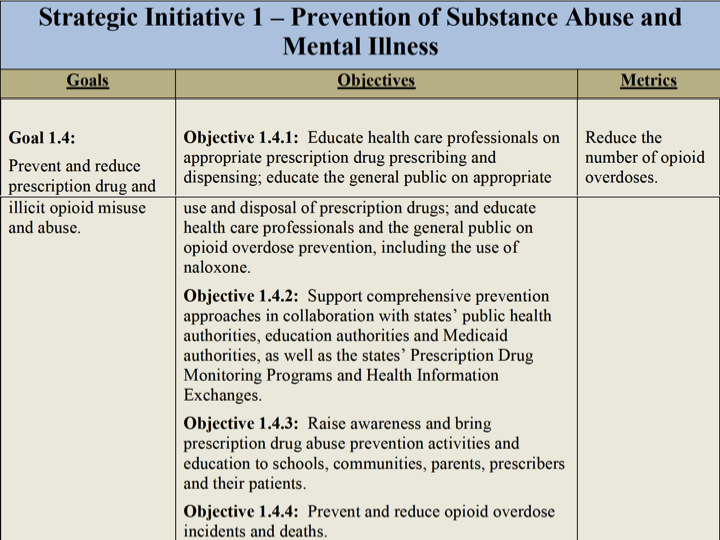
The administrators here take the incredibly naive (or cynical) view that what they say will somehow be done. It is eerily similar to the original statements without proof or scientific backing that were made at the start of the opioid epidemic. In those administrative guidelines the most compelling feature was that physicians were not doing a good job treating pain and therefore they had to be educated about it. These guidelines were written by nobody less than the Joint Commission. Now SAMHSA in their infinite wisdom is deciding that physicians need more education about this. Administrators like to play the education card. They don't seem to understand that this problem, specifically the problem of overprescribing has little to do with education and more about how physicians are being manipulated to provide services that somebody who does not have a clear picture of medical care wants. Let's remember the SAMHSA track record here. From the FDA web site, the FDA claims that in 2009 it launched an initiative with SAMHSA "to help ensure the safe use of the opioid methadone." From that press release (my emphasis added in the underlined section):
"The methadone safety campaign materials provide simple instructions on how to use the medication correctly to either manage pain or treat drug addiction," said H. Westley Clark, M.D., J.D., M.P.H., C.A.S., F.A.S.A.M., Director of SAMHSA’s Center for Substance Abuse Treatment. "Our goal for this training is to support the safe use of methadone by all patients and prescribing healthcare professionals."
The operative term is "all patients and prescribing health care professionals." In other words SAMHSA was seeing this as an educational deficit. The detailed program is still available online. If only the health care professionals could be educated enough by an administrative body that knows more than they do, the epidemic of methadone related deaths from overdose would stop. The problem occurred when the CDC looked at the epidemiology of single and multiple drug deaths involving opioids and found that the methadone related deaths occurred at much higher rates in both categories than other opioids. Their recommendation stands in contrast to the SAMHSA educational initiative. From that document - my emphasis added in the underlined section:
The CDC does not believe that the problem with the disproportionate deaths from methadone is an educational deficit. They believe it is a problem inherent in the drug, clinical setting, and experience of the physician. It should definitely not be prescribed by all physicians, even if those physicians are educated. SAMHSA apparently still believes in the educational deficit. As I have posted the associated regulatory problems includes the FDA and their continued approval of high dose opioid products against the advice of their scientific committees, and their plan to educate physicians to safely prescribe these products. I am using this example to illustrate that SAMHSA's approach, educate the masses and they will accept wellness and their health will improve by practicing wellness is a pipe dream of extraordinary dimensions. It does not work on a focal issue, why would it work on a population wide basis?
- Between 1999 and 2009, the rate of fatal overdoses involving methadone increased more than fivefold as its prescribed use for treatment of pain increased.
- Methadone is involved in approximately one in three opioid-related overdose deaths. Its pharmacology makes it more difficult to use safely for pain than other opioid pain relievers.
- Methadone is being prescribed inappropriately for acute injuries and on a long-term basis for common causes of chronic pain (e.g., back pain), for which opioid pain relievers are of unproven benefit.
- Insurance formularies should not list methadone as a preferred drug for the treatment of chronic noncancer pain. Methadone should be reserved for use in selected circumstances (e.g., for cancer pain or palliative care), by prescribers with substantial experience in its use.
Paul Summergrad's take on the politicalization of wellness/recovery versus psychiatry/medicine was a very accurate statement. Americans in general are intolerant of probability statements. Blog discussions are a particularly intolerant environment. I do not agree with his support of integrated or so-called collaborative care. It is no surprise that SAMHSA supports and has a leadership role in this managed care strategy. He stops short of pointing out that SAMHSA has nothing to offer patients with severe mental illnesses.
Besides being basically a pro-business strategy, the SAMHSA initiative also takes the grandiose approach that there are no psychiatrists out there (I will let other mental health clinicians speak for themselves) who want to see the people they treat recover and lead meaningful and satisfying lives. They make it seem like their simple business objectives will be better at this goal than personalized treatment provided by a psychiatrist. That may provide a rallying point for the detractors of psychiatry, especially when the APA chooses not to counter the insult, but it is not a concept based in reality. There is nothing more important in the practice of medicine than how a patient does under a physician's care.
I think it is time for SAMHSA to put up or shut up. Even though they have probably stacked some of the outcome statistics in their favor ahead of time and some of the outcome measures are as vague as managed care company measures of excellence (both proven business strategies), let's see what happens. And let's see if the Big Pharma critics are as skeptical of their outcome statistics as they are of a typical pharmaceutical industry funded clinical trial.
So far they have a solid check minus on the opioid initiative.
George Dawson, MD, DFAPA