I was surprised to get a recent warning letter from the FDA on an inhaled preparation of loxapine called Adasuve. Loxapine is an antipsychotic drug of medium potency. Back in the late 1980s we had a drug trial of loxapine versus haloperidol on one of the inpatient units I was running at the time. It was a fairly effective drug for acute symptoms of psychosis and was less potent than haloperidol so it has fewer neurological side effects. It never seemed like a very popular medication with psychiatrists. There was some recurrent interest around the issue of first and second generation antipsychotics with some authors suggesting that it had a receptor profile that was more similar to second generation or atypical antipsychotics. During the initial period when it was approved and marketed under the brand name Loxitane it was available in both oral and injectable forms.
I could only locate one study at PubMed on the Adasuve in the current medical literature searching on the brand name. There were 20 studies at clinicaltrials.gov web site but unfortunately no results were posted. Some of them appear to be very interesting including one that looks at the QTc interval effects of inhaled loxapine. A review of the Adasuve web site shows that bronchospasm is a black box warning and that there is a Risk Evaluation and Mitigation Strategy (REMS) to assess prior to prescribing and monitoring the patient after each administered dose. It looks like it can only be given in a registered health care facility by personnel who can assess and manage any pulmonary complications. Although the pulmonary conditions that contraindicate use seem fairly straightforward (asthma, COPD, any pulmonary diagnosis associated with bronchospasm) the actual diagnoses are probably more complex due to a number of factors including smoking status, body weight, and the complexity of the underlying pulmonary syndromes. Staff administering this medication should assess the patient for pulmonary problems at every episode and not depend on historical diagnoses.
From a philosophical standpoint, there needs to be an active debate about new patents or patent extensions on medications that are currently generic drugs like loxapine. During the time it was primarily used it certainly did not demonstrate any superior efficacy or side effect profile relative to other typical or atypical antipsychotics. Loxapine is metabolized to amoxapine, an FDA approved antidepressant that has been used on a limited basis in psychiatric practice and is generally not considered a first or second line antidepressant. The metabolic relationship led some authors to speculate that the combination may be effective in psychotic depression but that application was never realized. So in this case we have a drug with limited applications that has been repackaged in a riskier dosage form. That seems like several steps in the wrong direction. The details about the pharmacokinetics are available in the package insert. Looking at this data, the main advantage appears to be the short time is takes to reach maximum plasma concentration (1-2 minutes). A useful study here would have looked at a subgroup of patients taking parenteral loxapine and similar pharmacokinetic measures. In the study I alluded to from the 1980s loxapine was compared directly to haloperidol for acute agitation in schizophrenia or bipolar disorder.
With this medication released into practice, if I was still working on an acute inpatient unit I would be very skeptical of using this medication for acute agitation. Use is limited to a single dose in a 24 hour period. The people who need this medication are generally medically complex, may still have street drugs in their system, are generally cigarette smokers and their pulmonary and in many cases their cardiac status may be unknown. If the initial dose is not effective, the question becomes - now what? Patient preference may be an issue since some patients request a fast acting medication but they do not want parenteral injections. Patients with an addiction history may have used drugs by insufflation, inhalation, and intravenous injection and that may be a factor in their decision making. All other factors considered there have been studies of patient preference for specific medications to treat acute agitation and of the antipsychotic class of medications only olanzapine is highly rated. Besides the degree of acceptance, post marketing surveillance will be important in terms of medication side effects. The current approval was based on pooled data from three studies looking at a total of 259 patients getting the active medication and 263 patient receiving placebo. That is not many doses of this medication.
Zohydro probably requires less discussion. Zohydro is advertised as the only acetaminophen free, extended release form of hydrocodone available in the United States. It is available in dosage forms ranging from 10 mg to 50 mg intended as a twice-a-day dose schedule. Zohydro comes with the following black box warning:
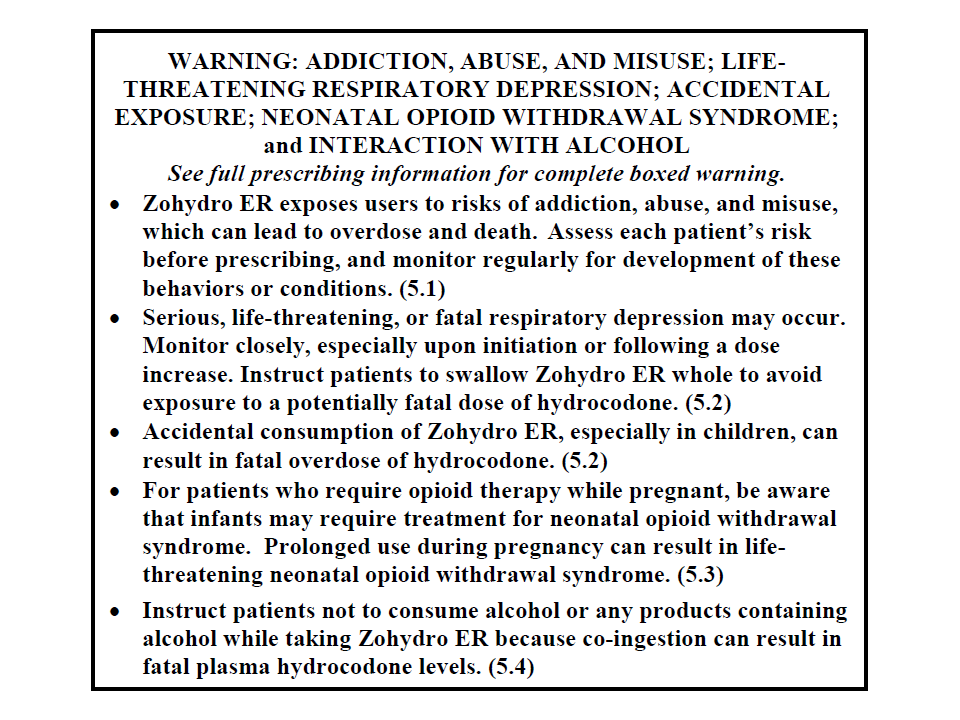
The interesting part of this approval process was that the scientific advisory panel, for the FDA voted overwhelmingly against approving this medication, but it was approved anyway. We are currently in the midst of an opioid epidemic based on a number of metrics including emergency department visits for complications, deaths from accidental overdose, per capita consumption of opioids relative to the rest of the world, and the increasing number of people addicted to opioids. We are also entering a period of increased policing of physicians by numerous agencies for opioid prescribing practices. There is fairly good evidence that the "opioid epidemic" started with a pain treatment initiative suggesting that physicians were not treating pain aggressively enough. The pendulum has swung to the point where there will be clear blame for at least some physicians who are using opioids to treat chronic pain.
There are a couple of additional problems with the FDA approved package insert for Zohydro. The first is the Indication or reason the FDA approved this drug in the first place. The indication for Zohydro is: ".....the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment for which alternative treatment options are inadequate." That is a shockingly inadequate description of a pain syndrome. In keeping with a medication as a tool model for regulatory approval this is acceptable. But any physician prescribing this medication should have a more specific pain diagnosis that specifically addresses the chronicity of the pain and why this might be an acceptable approach.
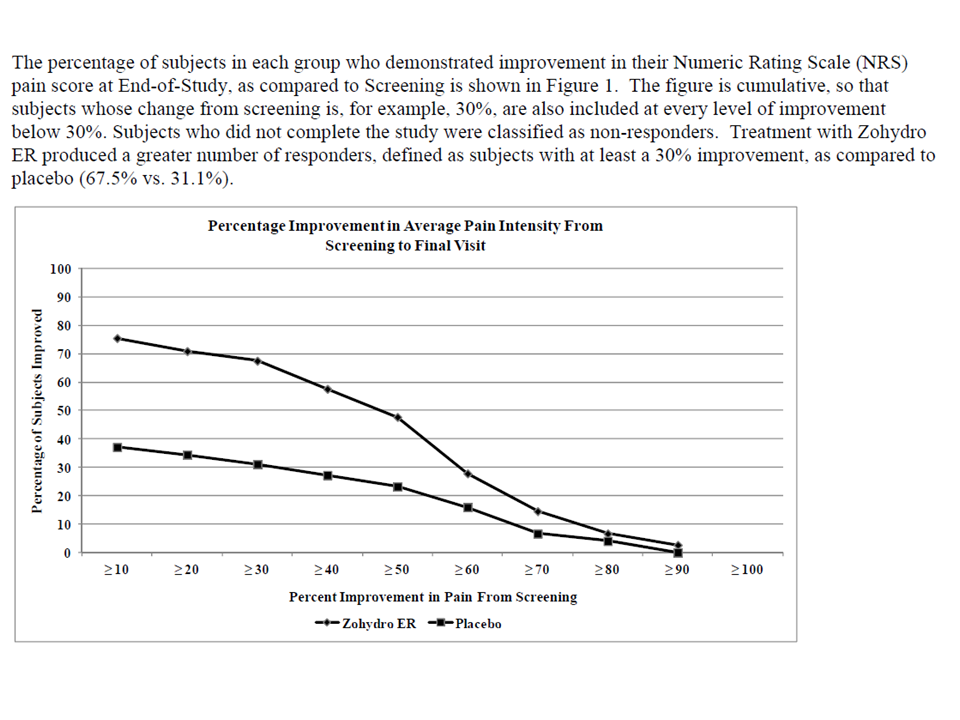
The second problem on my first read through of the package insert is the following graphic of the efficacy of this medication. It plots the results of an study of Zohydro versus placebo in 510 subjects who were already on chronic opioid therapy for chronic back pain.
From an addiction standpoint, hydrocodone and acetaminophen compounds are some of the most frequently diverted and abused compounds. It is not uncommon to get a history of people taking amounts that are the equivalent of chronic overdoses with the acetaminophen component. Many if not most of the people with this addiction are aware of the risks of the acetaminophen component but when the chronic phase of the addiction develops they will continue to use it and ignore that danger. Patient preferences can be a factor in the decision to prescribe an opioid. Hydrocodone combination medications are in high demand on the street indicating to me that is is a preferred product to many addicts. The package insert contains remarkably little useful practical information on abuse, dependence, and addiction. We are told that there is a REMS strategy and that the FDA is requiring manufacturers of newly approved long acting opioids to conduct long term follow up studies to look at the "serious risks of long term use."
I think it would be a lot easier if FDA regulators just looked at the current data on the CDC web site about the addiction risk of opioids and answer the question: "Why would Zohydro be any different?"
George Dawson, MD, DFAPA
FDA. Adasuve Full Prescribing Information. (Click on appropriate link).
European Medicines Agency. Adasuve EPAR (European Public Assessment Report).
Additional Clinical Note 1: On 1/14/2014 the FDA issued a recommendation that health professionals stop using combination products that contain more than 325 mg acetaminophen. That same page has a link to a letter that will be sent to manufacturers that these dose strengths be withdrawn over the next three years. Based on their rationale (no increased efficacy with acetaminophen and risk for hepatotoxicity), I don't know why 325 mg acetaminophen is the magic number. The addiction experience with combination products suggest that people will routinely use potentially toxic doses as part of their addiction, even when they know that there is a potential problem with the amount of acetaminophen. This new rule may increase increase the amount of opioids prescribed.

