The Mayo Clinic came out with their recommendations on what to do about the FDA's warning about citalopram. By their own description they are more liberal with regard to their citalopram recommendations and more conservative regarding escitalopram. I have previously reviewed the problem here and concluded that there is really a lack of data available on the likelihood of electrocardiogram abnormalities during normal clinical use and if citalopram is as cardiotoxic as the FDA is describing it - we should treat it more like a standard antiarrhythmic drug and used flecanide as an example.
For all practical purposes that would include baseline ECGs, ECGs at the max dose and taking it up one more level from either the Mayo Clinic or the FDA - a stress test looking for QTc prolongation at higher heart rates. The other elements in the Mayo recommendations based on history and physical examination and expecting some physician knowledge of drug metabolism are fairly standard. I thought it was interesting that they did not mention checking plasma levels of the drug especially in complex cases (eg. a patient with cirrhosis) who only responds to higher than recommended doses of the drug. Regarding the statements: "Selective serotonin reuptake inhibitors cannot simply be substituted for one another, not even escitalopram for citalopram." That is generally true and where are these guys in the battle against PBMs saying that these drugs are all equivalent? I have not found any patient that responded selectively to citalopram and not escitalopram. I have generally been able to convert patients to an equivalent amount of escitalopram the next day.
Both the Mayo Clinic and the FDA are silent on molecular approaches to solving this problem and screening patient for potential risk before they are started on either drug. The Mayo Clinic offers testing for cytochrome P450 genotypes. The genetic basis for hereditary prolonged QTc intervals has been a hot topic of research over the past decade. It is probably time to expand the search for additional genotypes that place people at risk during specific drug therapies. Until then we have only very approximate methods of determining the at - risk population and keeping them safe and the Mayo recommendations are more reality based than the FDA.
I think it would also be possible to estimate the risk associated with taking citalopram across the entire population. In fact, at this point the FDA seems to have the data to estimate the risk of any QTc effect at all to the risk of torsade de pointes - the most significant arrhythmia. I think it is very important for patients making the decision to have this number and if I can provide numbers on rare but serious antidepressant complications like serotonin syndrome, a federal agency with more perfect information and no patient care responsibility can do better.
George Dawson, MD, DFAPA
Sheeler RD, Ackerman MJ, Richelson E, Nelson TK, Staab JP, Tangalos EG, Dieser LM, Cunningham JL. Considerations on safety concerns about citalopram prescribing. Mayo Clin Proc. 2012 Nov;87(11):1042-5.
FDA Drug Safety Communication: Revised recommendations for Celexa (citalopram hydrobromide) related to a potential risk of abnormal heart rhythms with high doses.
Showing posts with label citalopram. Show all posts
Showing posts with label citalopram. Show all posts
Friday, November 23, 2012
Sunday, April 29, 2012
Does the FDA discriminate against antidepressants?
The FDA came out with a new warning on citalopram on 3/28/2012. The main point of the warning is that citalopram may lead to electrocardiogram changes that can be associated with an abnormal heart rhythm or arrhythmia that is potentially fatal. The specific change is prolongation of the QTc interval or the interval that correlates with the total duration of ventricular activation and recovery.
Citalopram is a widely used antidepressant medication and it widely used for three reasons. It is not likely to have a lot of interactions with other drugs. Citalopram figured prominently in the STAR*D algorithm from the largest study done on enhancing antidepressant effectiveness. A third reason is that it is a generic medication and it is very inexpensive. Psychiatrists have broad experience with the drug and the general experience is that it is well tolerated with little toxicity.
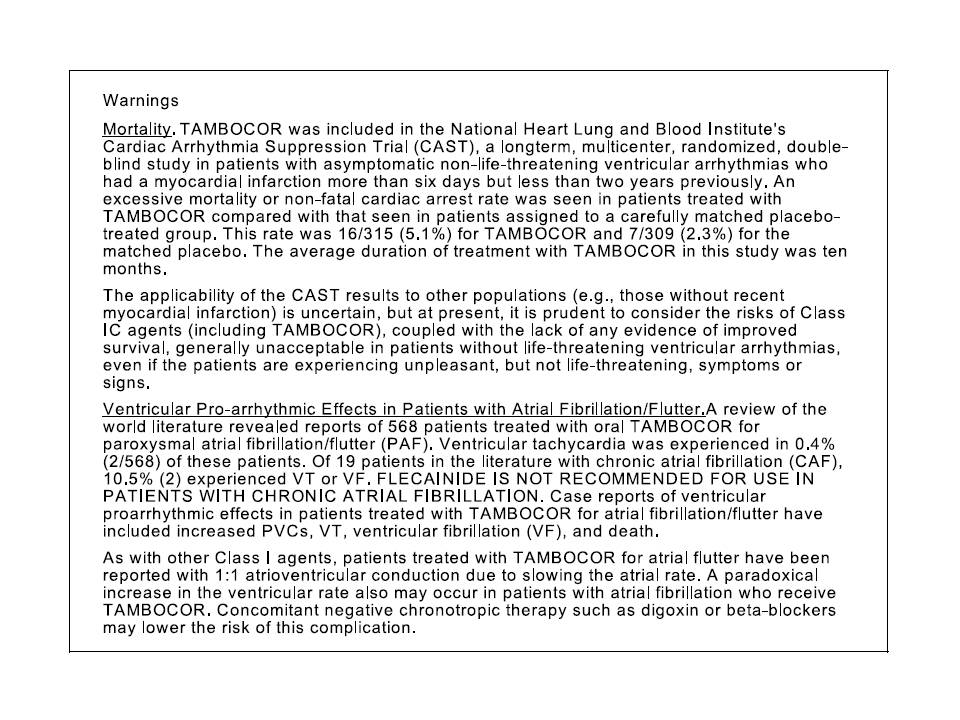
Flecainide is a Type IC antiarrhythmic agent indicated for the prevention of paroxysmal atrial fibrillation (AF), paroxysmal supraventricular tachycardia (PSVT), and the prevention of life-threatening ventricular arrhythmias like sustained ventricular tachycardia. The FDA warnings on the drug include proarrhytmic effects and excess mortality. The excess mortality was directly observed in a clinical trial done to suppress ventricular arrhythmias.
The black box warnings for each drug listed below are directly from Medline:
Looking at the safety concerns for both medications - important differences emerge. First, the FDA recommends maximum doses for the citalopram not just for the a maximum dose for adults but in specific conditions including aging. Searching the FDA web site shows exactly 25 references for safety concerns of flecainide and none of them contain that level of information. Second, the citalopram warning shows a table of QTc interval changes by dose for both citalopram and escitalopram. There is no information in FDA documents (that I could find) for flecainide even though it is widely accepted that flecainide causes dose related changes in not just the QTc interval but also the QRS and PR intervals along with a host of additional effects on cardiac pacemakers and conduction. The overall tone of the release is that citalopram is a potentially cardiotoxic drug. Third, the ECG monitoring recommendations are not internally consistent. The absolute cut off of a QTc interval of 500 ms is highly unlikely - even in cases where the patient is taking 60 mg per day or more of citalopram. It is also unlikely that the QTc intervals in the citalopram warning will lead to a QTc interval of greater than 500 ms. This will result in tens of thousands of ECGs done because that is the only way that the QTc interval can be determined.
The black box warnings and the recently issued warning all considered, serious questions are raised relative to drugs with known cardiotoxicity and the whole issue of QTc warnings in all psychiatric drugs. Certainly nobody wants a rare severe complication as a result of a prescription medication but can it really be avoided? What good would ECG screening do? There have not been any trials to address that issue of whether all patients taking citalopram need baseline ECGs. All the patients taking flecainide have probably had multiple ECGs done that indicate a possible need for treatment but there is little guidance on the ECG issue. In many patients taking flecainide, patients get serial ECGs and they do exercise stress tests to rule out proarrhythmic effects. Are the same precautions needed for patients on citalopram?
Are the thresholds for treatment different given the fact that flecainide caused increased mortality during clinical trials and citalopram did not? There would be an argument that flecainide is used to treat life-threatening arrhythmias, but the other indication is for prevention of atrial fibrillation and atrial fibrillation is not a life threatening arrhythmia. With regard to the seriousness of the diagnosis, major depression carries a lifetime mortality of 10%. Finally, where is the table on the relationship between flecainide dose and QTc prolongation like we see for both citalopram and escitalopram? Is it possible that flecainide has more of an effect throughout the dosage range than citalopram?
These are serious questions given that I have already established that there is a significant bias in the media against psychiatry, psychiatrists and psychiatric medications. The most recent FDA warning has created a lot of anxiety for psychiatrists and any patient taking citalopram. The majority of those patients are being seen by primary care physicians.
If citalopram is that cardiotoxic, let's see the evidence and let's see how it compares to a medication with known cardiotoxicity. Let's have the same level of warning for both medications and some concrete ideas about what needs to be done to manage that risk.
George Dawson, MD, DFAPA
Subscribe to:
Posts (Atom)