
An article entitled Euthanasia and Assisted Suicide of Patients With Psychiatric Disorders in the Netherlands 2011-2014 caught my eye in this month's JAMA Psychiatry (1). It wasn't that long ago that I recall being in the midst of a rather intense argument in a staff meeting about euthanasia in the broadest of terms. Like many heated political arguments (I consider a lot of what goes on under the heading of ethics to be little more than politics) this one degenerated to personal terms. The pro-euthanasia proponent ended the argument with: "Well if I am dying of terminal cancer and I want to end it, there is no one who is going to tell me that I can't do it. Not you or anyone else." In the dead silence that followed nobody brought up the obvious point that is the state of affairs currently. Euthanasia proponents have always made that argument when in fact what they really want is to recruit physicians to provide them with euthanasia. That is hardly the same thing as actively stopping them. I would make the secondary argument that nobody really needs to be actively recruited these days. I can't remember the last legal battle about whether a physician providing hospice care ordered too many opioids and benzodiazepines for a suffering terminally ill patient. If I had to guess, the last time I saw that question raised in a court in the Midwest was about 20 years ago.
The concept of euthanasia in patients with psychiatric disorders is an even more complicated process. Psychiatric disorders per se are not terminal illnesses, there is no protracted phase of increasing suffering and futile live saving measures with a fairly predictable death. Death primarily due to psychiatric disorders occurs as a result of suicide, risk taking, comorbid medical illnesses, and severe disruptions in self care and homeostasis due to acute disorders like catatonia. These are all relatively acute processes. That does not mean that there are no people with chronic mood disorders, personality disorders, and psychoses. Is the suffering in these situations acute and severe enough that euthanasia should be considered and if so, do any standards apply?
The authors of the Dutch study set out to study the characteristics of psychiatric patients receiving euthanasia or assisted suicide (EAS) in Belgium and the Netherlands. The case studies of 66 cases were reviewed in the database of the Dutch regional euthanasia review committees. There were 46 women and 20 men. A little over half (52%) had made previous suicide attempts. 80% had been hospitalized in psychiatric units. Most of the patients were aged 50-70 but 1/3 were older than 70. Most (36) had depression and 8 of those patients had psychotic features. The patients were described as chronically symptomatic and 26 patients had electroconvulsive therapy (ECT). Two had deep brain stimulation - one for obsessive compulsive disorder and one for depression. There was significant medical comorbidity. The authors comment that there was very little social history to the point that they could not reconstruct the persons current living situation from what was abstracted. Some of the reports contained fairly subjective data - as an example: "The patient was an utterly lonely man whose life had been a failure." There was extensive treatment but also treatment refusal in 56%.
Twenty-one patients had been refused EAS at some point and in 3 of these cases the original physician changed their mind and performed EAS. In the other 18 patients, the physician performing the EAS was new to the patient. In 14 of those cases that physician was affiliated with a mobile euthanasia practice called the End-of-Life Clinic. In 27 cases a psychiatrist did EAS and the rest were general practitioners. Physicians disagreed in about 24% of the cases and EAS proceeded despite the disagreement. In 8 cases the psychiatric consultant did not think that due care criteria specifying "no reasonable alternative" had been met. The Euthanasia Review Committee (ERC) found that due care criteria were met in all psychiatric cases referred except for one. In another case the ERC was described as being critical but in the end agreed with the euthanasia decision. It was a case of a man who broke his leg in a suicide attempt and then refused all treatment and requested EAS.
The authors come to several conclusions. The first involves the issue that in this study the ratio of women to men was 2.3 to 1 and that is the opposite of what is expected with suicide. They suggest that the availability of EAS may make the desire to die "more effective" for women. Although the overall psychiatric sample was younger than the non-psychiatric EAS cases, they argue that the fact that a significant portion have significant comorbidities and this may indicate that Dutch physicians tend to self regulate EAS to a specific patient profile. They point out that more judgment is required in psychiatric cases than in the cases involving terminal physical illness - 83% of which involved a malignancy. They note that decision-making capacity can be affected by neuropsychiatric illness and that medical futility is difficult to determine especially when care is refused. There were no official EAS psychiatric consultants involved in 41% of the cases. In 11% of cases there was no psychiatric involvement at all. Their overarching observation was that EAS for psychiatric illnesses involved making decisions about complex disorders and considerable judgment needed to be exercised. They suggested that the decision about EAS required "considerable physician judgment" and that regional committees overseeing euthanasia deferred to the opinion of the treating physician when consultants disagreed.
I have never seen it discussed but conflict of interest issues are prominent in any decisions about the autonomy of people who are designated psychiatric patients. At the first level, there is the wording of the policy or statute. There are criteria that are thought to be very objective that are used to decide if a person should be subject to civil commitment, guardianship, conservatorship, or any of the laws involving competency to proceed to trial, cooperate with one's defense attorney, or a mental illness or defect defense. In all cases, the wording of each state's statute would seem to determine an obvious standard. Those standards are routinely compromised in practice by any number of political considerations. In the case of not guilty by reason of mental illness, the compromise occurs any time there are high profile cases that involve heinous crimes. No matter how severe the mental illness, there will be a raft of experts on either side and the verdict will almost always be guilty. At the other end of the spectrum is civil commitment. Observing any commitment court over time will generally show the oscillation between libertarian approaches to more strict standards where need for psychiatric treatment is the more apparent standard. The libertarian approach often uses a standard of "imminent dangerousness" as an excuse to dismiss the patient irrespective of what the statute may say. It also seems to coincide with the available resources of the responsible county. That is why in Minnesota the land of 10,000 lakes and 87 counties we say: "On any given day there are 87 interpretations of the civil commitment law." Despite that range of interpretations, it would be highly unlikely that a patient who broke his leg in a suicide attempt (a case presented in this paper) would not be a candidate for court ordered treatment rather than euthanasia. On the other hand, I do not know anything about civil commitment and forced treatment in the Netherlands.
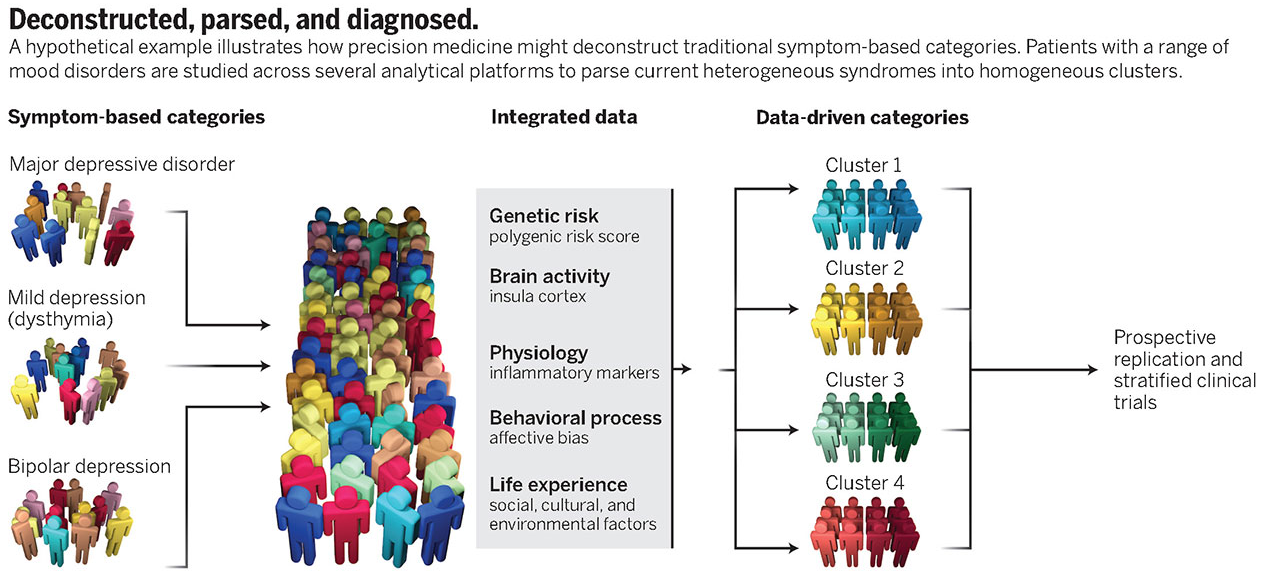
There is no reason I can think of that a euthanasia standard can be interpreted any more logically. This Dutch study points to that. It also points to another issue that is never really discussed when it comes to psychiatric diagnosis or the ethics and laws that apply to them. The conscious state of the individual is never recognized. Brain function is parsed very crudely into separate domains of symptoms, cognitions, and decisions. The examiner or legal representative usually has some protocol by which they declare the person competent or not and the legal or ethical consequences proceed from that. There may be a discussion of personality that is also based on this parsing process. Very occasionally there is a discussion of the person's baseline, but that is about it. That is a serious problem for any student of human consciousness. Let me explain why. I think that it is a universal human experience to experience a transient (days to months) change in your conscious state that might result in you not wanting to live. The insult could be a physical or mental illness. It would seem to me that at a minimum there can be multiple conscious states operating here that look like a request for assisted suicide or euthanasia. The limits would be bounded by a completely rational decision based on medical futility and suffering on one side and an irrational decision based on the altered conscious state on the other. The only way for any examiner to make that kind of determination is to know the patient very well over time to recognize at the very least that they are not themselves. Doing an examination for the express purpose of determining if a person meets criteria for euthanasia in a short period of time is by contrast a very crude process.
There is too much variability in the patient's conscious state and how that impacts treatment and ultimately recovery to consider psychiatric disorders as a basis for a decision about euthanasia and assisted suicide.
George Dawson, MD, DFAPA
References:
1: Kim SH, De Vries RG, Peteet JR. Euthanasia and Assisted Suicide of Patients With Psychiatric Disorders in the Netherlands 2011 to 2014. JAMA Psychiatry.2016;73(4):362-368. doi:10.1001/jamapsychiatry.2015.2887.
2: Appelbaum PS. Physician-Assisted Death for Patients With Mental Disorders—Reasons for Concern. JAMA Psychiatry. 2016;73(4):325-326. doi:10.1001/jamapsychiatry.2015.2890.
Supplementary 1: I intentionally wrote the above post without reading the accompanying commentary by Paul S. Appelbaum, MD. Dr. Appelbaum is an expert in forensic psychiatry and has written extensively on ethical issues in psychiatry. Dr. Appelbaum's essay provides some additional facts, but his areas of concern do not touch on my focus on the conscious state of the individual.

.png)




{kind=link}
{kind=link}