This is the third Labor Day of this blog. I usually take the opportunity to mark the lack of progress in the physician work environment and this year is not much different. All of the usual corporate and government buzzwords being promoted to suggest why physicians need to be managed by somebody who knows nothing about medicine. All of the hype about computerization and how the grossly overpriced electronic health record will save us all, even as the printout from that record looks less and less coherent. I just read a copy of The Institute from the IEEE on Big Data. From that report:
"It's is estimated that the health care industry could save billions by using big-data health analytics to mine the treasure trove of information in electronic health records, insurance claims, prescription orders, clinical studies, government reports, and laboratory results.
Analytics could be used to systematically review clinical data so that treatment decisions could be based on the best available data instead of on physicians' judgment alone...."
The state of current electronic health records as the worst value in the information technology sector is is probably not too surprising given the above observations or the following:
"Instead of seeing only 20 patients a day, doctors are able to see 75 to 100 people and get ahead of the wave..."
I don't know what kind of doctor sees 75-100 patients a day or what the quality of these visits is, but I have never met a physician who wanted to see that many people in a day and wonder if it would not trip a billing fraud flag somewhere in the CMS data base. I have talked with many physicians who were overwhelmed by coming into the office and having 200 tests to review and sign an additional 30-50 orders in addition to seeing 20 patients that day. We are decades away from any machine intelligence being incorporated into the medical record. The current EHR has destroyed the narrative, especially in psychiatry and converted the basis of care to a checklist. Instead of higher order machine assisted decision making the electronic health record has not resulted in the expected savings or utilization of technology. Paying tens of millions of dollars in licensing fees per year and larger IT departments with thousands of PCs running 24/7 to access the sever farm has not produced a nickel of savings and has added large recurring costs.
So I have not noticed any striking improvements in the practice environment. At the same time, it is at such a low level that it is difficult for me to say that it has deteriorated any further. The American Psychiatric Association (APA) the largest professional organization for psychiatrists still supports collaborative care - a managed care model of psychiatric care that in some cases eliminates any direct access to psychiatrists. The American Medical Association also seems managed care friendly largely due to their support of the PPACA. Both organizations support the onerous recertification process mandated by the American Board of Medical Specialties.
The only bright spot I can think of this year was being seated at the same table with 3 younger colleagues at at a Minnesota Psychiatric Society CME event. They had all been practicing for 10 years or less. They were all in private practice to one degree or another. They were all women and although I haven't seen it studied I think that women may have a greater skill level (at least relative to men of my generation) in setting up and managing a private practice. I was quite interested in their experiences and they listed all of the positives. The overwhelming positive that I took away from that meeting was that their practice environment was very positive because they ran it and had eliminated all of the toxic administrators along the way who were supposed to manage them. They did not have to tolerate the notion that just because they were an employee that they suddenly needed supervision from somebody who was not qualified to supervise them. Near the end of our conversation they tried to talk me into going into private practice myself. I have always been an employee, but my current vocational trajectory has been predicated on fleeing toxic administrators. I gave the usual excuses about being one bad cold away from retirement and an old dog not being able to learn new tricks.
If I was starting out today - I would only be working for myself and I would try to design the practice to reflect my interests in neuropsychiatry and severe mental illnesses. Any resident reading this should consider this career path. The decision may be as easy as contemplating seeing 75-100 patients a day and meeting with an administrator who suggests that you could see more.
Happy Labor Day to any physician reading this whether you are in private practice or on the assembly line in a clinic or hospital somewhere. And good luck to physicians everywhere in avoiding unnecessary administration.
George Dawson, MD, DFAPA
Kathy Pretz. Better Health Care Through Data. The Institute September 2014. p 6 - 7.
Showing posts with label conflict of interest. Show all posts
Showing posts with label conflict of interest. Show all posts
Monday, September 1, 2014
Monday, April 7, 2014
Prior Authorizations - An Incredible Waste of Time
Anyone who has read this blog in the past is aware of my opinion of middlemen in health care and how they waste everyone's time and run up costs. Pharmacy Benefit Managers (PBM) remain there right up at the top. The PBM is the company that your doctor calls to get authorization so that an insurance plan will pay for all or part of a specific prescription drug. It has never been more clear to me that their sole function is to be an obstacle to the physician, the pharmacist and the patient. The goal of that obstruction is to increase the likelihood that anyone of those parties will give up at some point and either not fill the prescriptions or accept a different product that is less expensive, less effective, or one that has more side effects. I am sure that the pharmaceutical companies have gamed the system to make it harder for PBMs to deny claims on a scientific basis. They can do this by maximizing the number of FDA approved indications up front. In many cases that results in a product with multiple diverse indications so that the newer medication can be prescribed based on secondary indications. The physician, pharmacist and patient are left to deal with all of the unnecessary bureaucracy in between.
I posted my interaction with a PBM sometime ago and named them in that post. I learned about the power of corporate America as a result of that post. The VP of the company involved called me the next morning and wanted information about the patient involved. One thing led to another but the bottom line was that I pulled that post as a result of that sequence of events. Since my position has not significantly changed since then, the companies involved here will remain nameless. Keep in mind that identical transactions occur tens of thousands of times per day in the United States as PBMs and pharmaceutical companies battle for the healthcare dollar at your expense.
I am still working on the theory about how the VP of a PBM hears about a post on an obscure Internet blog and calls me the next day. The only three theories I have at this point are:
1. NSA grade Internet surveillance system by the managed care cartel.
2. A reader wants to see me silenced because they disagree with my viewpoint or just dislike psychiatrists. They forwarded the link to the company named in my original post.
3. My reputation as a tireless crusader against managed care and all of its associated systems. Well not so much a crusader, but there have been some memorable moments. Like a conference where I was speaking out against managed care - rather vehemently only to have the VP of one of these organizations remark: "Dr. Dawson - don't you work for a managed care organization?"
If I did - they never censored me.
Back to the case at hand. I was called originally by a pharmacist and had no information about the situation. I had to call her back and ask for a fax. I got the fax and it contained the prescription and a number for the PBM. I called and got their endless and indecipherable telephone queue. After typing in the correct identification number 3 times and saying it once (I thought I would forgo the voice recognition system that is set up to not work) I was put on hold and connected with a human. He asked me to "verify" in a line by line manner all of the data already on the faxed form. After wasting those minutes he talked about pulling up the prior authorization points as though he was going to call in another person for that detailed process. After a long pause (I am sure that many of my colleagues lose it at this point) he asked me the indication for the drug. This drug has only one indication and I told him. He said: "It's approved."
That sequence of events, taking a total of about 20 minutes would be enough to piss off any intelligent person, but then he said: "The office can call the pharmacy and tell them the prescription is authorized" I was momentarily confused and said "What office?" He said: "Your office."
That's right. Here we have a sequence of events that starts at the pharmacy with the PBM telling the pharmacist that prior authorization is needed. The pharmacist has to talk to me twice on the phone and send me a fax. And I have to complete this waste of time by calling and acting like an agent of the PBM. Just to be sure that I wasn't being totally lied to I asked the pharmacist if it was true that the physician's office had to call and complete this sequence from hell. Her response was "It's about 80:20 from the doctors' offices."
Call me a dinosaur. Call me a hot head. But this exercise in helping corporate America make more money, while taking valuable time away from me, my employer, my patients, and my family is an abomination and a manipulation. It can exist only in a country where corporate welfare is the rule of the day and conflict of interest is at all levels of government. From the perspective of corporate America prior authorization is a good way to get physicians and pharmacists to work for them for free. From the physician's perspective - it is a complete waste of time.
George Dawson, MD, DFAPA
Supplementary 1: Although the sequence of events listed above may sound incredible it is not. I have dealt with PBM telephone queues where there was no way out. You could not enter the numbers by keypad or say them through voice recognition. There was no way to speak to a human. I had to call the pharmacist back and explain that the prior authorization through the PBM was basically a sham and if the patient wanted the medication they would need to pay for it out of pocket.
It would be a lot more honest if the PBM would just tell people: "We make money by denying your prescriptions and in an ideal world we would prefer to not have to pay for anything."
But I guess that would be bad for public relations.
I posted my interaction with a PBM sometime ago and named them in that post. I learned about the power of corporate America as a result of that post. The VP of the company involved called me the next morning and wanted information about the patient involved. One thing led to another but the bottom line was that I pulled that post as a result of that sequence of events. Since my position has not significantly changed since then, the companies involved here will remain nameless. Keep in mind that identical transactions occur tens of thousands of times per day in the United States as PBMs and pharmaceutical companies battle for the healthcare dollar at your expense.
I am still working on the theory about how the VP of a PBM hears about a post on an obscure Internet blog and calls me the next day. The only three theories I have at this point are:
1. NSA grade Internet surveillance system by the managed care cartel.
2. A reader wants to see me silenced because they disagree with my viewpoint or just dislike psychiatrists. They forwarded the link to the company named in my original post.
3. My reputation as a tireless crusader against managed care and all of its associated systems. Well not so much a crusader, but there have been some memorable moments. Like a conference where I was speaking out against managed care - rather vehemently only to have the VP of one of these organizations remark: "Dr. Dawson - don't you work for a managed care organization?"
If I did - they never censored me.
Back to the case at hand. I was called originally by a pharmacist and had no information about the situation. I had to call her back and ask for a fax. I got the fax and it contained the prescription and a number for the PBM. I called and got their endless and indecipherable telephone queue. After typing in the correct identification number 3 times and saying it once (I thought I would forgo the voice recognition system that is set up to not work) I was put on hold and connected with a human. He asked me to "verify" in a line by line manner all of the data already on the faxed form. After wasting those minutes he talked about pulling up the prior authorization points as though he was going to call in another person for that detailed process. After a long pause (I am sure that many of my colleagues lose it at this point) he asked me the indication for the drug. This drug has only one indication and I told him. He said: "It's approved."
That sequence of events, taking a total of about 20 minutes would be enough to piss off any intelligent person, but then he said: "The office can call the pharmacy and tell them the prescription is authorized" I was momentarily confused and said "What office?" He said: "Your office."
That's right. Here we have a sequence of events that starts at the pharmacy with the PBM telling the pharmacist that prior authorization is needed. The pharmacist has to talk to me twice on the phone and send me a fax. And I have to complete this waste of time by calling and acting like an agent of the PBM. Just to be sure that I wasn't being totally lied to I asked the pharmacist if it was true that the physician's office had to call and complete this sequence from hell. Her response was "It's about 80:20 from the doctors' offices."
Call me a dinosaur. Call me a hot head. But this exercise in helping corporate America make more money, while taking valuable time away from me, my employer, my patients, and my family is an abomination and a manipulation. It can exist only in a country where corporate welfare is the rule of the day and conflict of interest is at all levels of government. From the perspective of corporate America prior authorization is a good way to get physicians and pharmacists to work for them for free. From the physician's perspective - it is a complete waste of time.
George Dawson, MD, DFAPA
Supplementary 1: Although the sequence of events listed above may sound incredible it is not. I have dealt with PBM telephone queues where there was no way out. You could not enter the numbers by keypad or say them through voice recognition. There was no way to speak to a human. I had to call the pharmacist back and explain that the prior authorization through the PBM was basically a sham and if the patient wanted the medication they would need to pay for it out of pocket.
It would be a lot more honest if the PBM would just tell people: "We make money by denying your prescriptions and in an ideal world we would prefer to not have to pay for anything."
But I guess that would be bad for public relations.
Monday, January 27, 2014
WIll Integrity Save Psychiatry?
The answer is - it depends on how it is applied.
In the last two days, I have seen the integrity argument pulled out. Allen Frances is still using his bully pulpit on the Huffington Post, where it seems that anything critical of psychiatry is readily posted. In this case, he used the text of a blogger and the timeline created by this blogger to illustrate how there was no disclosure of a conflict of interest by a group of researchers, one of whom was the chair of the DSM-5 Task Force. The APA investigated this and acknowledged the non-disclosure of the conflict of interest. Apparently the acknowledgement in the form of an apology from the research group and the investigation by the APA is not enough for these critics. The blogger Dr. Nardo suggests that an "outside panel" be appointed to review his findings and the original materials again. I cannot think of how an "outside panel" could be convened. I have never really seen an objective analysis by an outside panel and wonder who might be selected. And yes I am suggesting that any outside panel would naturally have a significant conflict of interest. There appear to be many critics of psychiatry and only weak defenders.
He refers to a post by an anonymous web professional Neuroskeptic who summarized the state of things in his post as there being "no smoking gun." He also concludes that the idea of a psychiatric critics benefiting from book sales with the same theme suggests "by which logic, every author in history has had a financial conflict of interest in their own ideas." As a student of conflict of interest that IS a logical conclusion, especially when I see links to two of Dr. Frances' books listed right below the Huffington Post article. It is also an obvious fact that people routinely deny that applies to all human endeavors. If I am heavily invested in any subject my "ideas" can be counted upon to be fairly subjective and consistent with my self interest whether that is academic or financial. That is why I have read thousands of articles in Science, Nature, and medical journals in the past three decades and very few have panned out. At a larger level it is why Ioannides could declare that most published research is false. It is why you can count on seeing significant side effects from practically every medication approved by the FDA as safe and effective. So yes, I am afraid that same standard applies to the critics as well as the people doing the heavy lifting and trying to prove something in the first place. I would even take it a step further and suggest that the same transparency rules should be applied. How much money can you make as a critic of psychiatry or the DSM? My guess is plenty.
Both Dr. Frances and Dr. Nardo seem to be suggesting that all of the conflict of interest issues of academic psychiatrists and the way the APA handles them is sending psychiatry to hell in a handbasket. This is a historically incorrect view of the dismantling of psychiatry in the United States. Every day people in this country are getting inadequate psychiatric care. It has nothing to do with the ethical behavior of academic psychiatrists. It has a lot to do with the fact that the APA is not a very politically savvy organization and there are massive conflicts of interest interfering with the delivery of psychiatric care. Here are a few scenarios:
1. A depressed or psychotic but nonfunctional person is discharged from the emergency department because of a lack of "acute dangerousness" criteria. The family is outraged but they are told: "Look there is nothing we can do because he/she is not imminently dangerous to themselves. Upon further investigation the state has a "gravely disabled" criterion in the commitment statutes but it is practically never used. They find that local hospitals and courts never use that criteria because the patients admitted are too difficult to treat and place.
2. A person with acute alcohol and benzodiazepine withdrawal is sent home from the ER with a bottle of lorazepam and advised how to detoxify themselves. They go home and take the entire bottle to get high.
3. A person with alcoholism and depression is admitted for suicidal behavior. She was intoxicated, depressed and staring at a handgun. The next day the attending physician is contacted by a psychiatrist/utilization reviewer from the insurance company who has concluded the patient is no longer suicidal and they can be discharged. He will no longer authorize payment for inpatient treatment.
4. A pharmacy benefit manager refused to refill a 2 week prescription by a patient's psychiatrist. They have the pharmacist faxes a form to the psychiatrists office saying that they will only accept a 3 month prescription. The psychiatrist takes time to explain first to the pharmacists and then 2 different people at the PBM (total time 30 minutes) the rationale for not giving a large supply of medication to a chronically suicidal patient. The PBM refuses to change their position.
5. A managed care company refuses to cover psychotherapy provided by a psychiatrist. The psychiatrist explains that he is an expert in this type of therapy and the patient has been referred to him by the patient's primary psychiatrist. The managed care company authorizes 3 "crisis sessions".
6. A person completes a PHQ-9 scale in their primary care clinic and they score an 18. They see their primary care physician and say they would like to see a therapist. They are told to take an antidepressant and to come back in two weeks to fill out another PHQ-9. Total time of the visit is 5 minutes.
7. A person is seen in their primary care clinic and in 20 minutes is told by their nonpsychiatric physician that they have bipolar disorder. They are prescribed quetiapine, citalopram, and divalproex. Within several days they are too sedated to function at work.
The are just a few examples of thousands of people everyday who are receiving grossly inadequate care based on a specific ethical principle of physician behavior. That is the physician makes an assessment and prescribes care in what he or she believes is the best interest of the patient. That is the contract. There is no insurance company or government bureaucrat involved. There is no restricted access to mental health care or pretending that primary care physicians are psychiatrists. There is no remote "assessment" by a physician employed by a managed care company that prioritizes the financial well being of that insurance company or pharmacy benefit manager over the patient. In fact, I do not understand how that is ethical behavior at all.
That is the basis of the decline of psychiatry in this country. It has taken a proportionately larger hit than any other specialty. It is documented in detail on this blog and in E. Fuller Torrey's recent book. The adventures or misadventures of academic psychiatrists are relevant only insofar as the APA seems to use the President of the APA as a position that academics cycle in and out of. The idea that "psychiatrists in the trenches" are poorly represented by such a system is accurate with two possible exceptions that I can think of. Psychiatrists in the trenches are also poorly represented by criticism of academic psychiatrists and their conflict of interest agreements and personal employment contracts. It does nothing to address the central problems of the specialty, provides no tools that front line psychiatrist can use against all of the real conflicts of interest they face on a day by day basis, and is generally demoralizing. Before any critics suggest that I am supporting a "whitewash" - put yourself in the position of a psychiatrist who has just put in a 12 hour day taking care of 20 inpatients and putting up with passive aggressive and aggressive MCO and PBM reviewers who have been wasting your time and interfering with your care. You go home to read the paper and suddenly there is a major story of how unethical psychiatrists are - based on the appearance of conflict of interest. You try to remember that last time you saw a CME event that was sponsored by a pharmaceutical company. Then you check your files to make sure you have enough CME credits for relicensure. As an added piece of information that same psychiatrist doesn't really care about Section 3 in the DSM-5 or the issue of dimensional versus categorical diagnoses. They have not blinked an eye with the release of DSM-5 and won't in the future.
That is how the psychiatrist in the trenches experiences this academic exercise in conflict of interest. I say if you want to pull out an ethical argument and use that to help front line psychiatrists, it needs to be focused on the obvious targets in managed care and the government bureaucracies that support them.
You know - the real forces dismantling psychiatry (very effectively I might add) over the past three decades.
George Dawson, MD, DFAPA
In the last two days, I have seen the integrity argument pulled out. Allen Frances is still using his bully pulpit on the Huffington Post, where it seems that anything critical of psychiatry is readily posted. In this case, he used the text of a blogger and the timeline created by this blogger to illustrate how there was no disclosure of a conflict of interest by a group of researchers, one of whom was the chair of the DSM-5 Task Force. The APA investigated this and acknowledged the non-disclosure of the conflict of interest. Apparently the acknowledgement in the form of an apology from the research group and the investigation by the APA is not enough for these critics. The blogger Dr. Nardo suggests that an "outside panel" be appointed to review his findings and the original materials again. I cannot think of how an "outside panel" could be convened. I have never really seen an objective analysis by an outside panel and wonder who might be selected. And yes I am suggesting that any outside panel would naturally have a significant conflict of interest. There appear to be many critics of psychiatry and only weak defenders.
He refers to a post by an anonymous web professional Neuroskeptic who summarized the state of things in his post as there being "no smoking gun." He also concludes that the idea of a psychiatric critics benefiting from book sales with the same theme suggests "by which logic, every author in history has had a financial conflict of interest in their own ideas." As a student of conflict of interest that IS a logical conclusion, especially when I see links to two of Dr. Frances' books listed right below the Huffington Post article. It is also an obvious fact that people routinely deny that applies to all human endeavors. If I am heavily invested in any subject my "ideas" can be counted upon to be fairly subjective and consistent with my self interest whether that is academic or financial. That is why I have read thousands of articles in Science, Nature, and medical journals in the past three decades and very few have panned out. At a larger level it is why Ioannides could declare that most published research is false. It is why you can count on seeing significant side effects from practically every medication approved by the FDA as safe and effective. So yes, I am afraid that same standard applies to the critics as well as the people doing the heavy lifting and trying to prove something in the first place. I would even take it a step further and suggest that the same transparency rules should be applied. How much money can you make as a critic of psychiatry or the DSM? My guess is plenty.
Both Dr. Frances and Dr. Nardo seem to be suggesting that all of the conflict of interest issues of academic psychiatrists and the way the APA handles them is sending psychiatry to hell in a handbasket. This is a historically incorrect view of the dismantling of psychiatry in the United States. Every day people in this country are getting inadequate psychiatric care. It has nothing to do with the ethical behavior of academic psychiatrists. It has a lot to do with the fact that the APA is not a very politically savvy organization and there are massive conflicts of interest interfering with the delivery of psychiatric care. Here are a few scenarios:
1. A depressed or psychotic but nonfunctional person is discharged from the emergency department because of a lack of "acute dangerousness" criteria. The family is outraged but they are told: "Look there is nothing we can do because he/she is not imminently dangerous to themselves. Upon further investigation the state has a "gravely disabled" criterion in the commitment statutes but it is practically never used. They find that local hospitals and courts never use that criteria because the patients admitted are too difficult to treat and place.
2. A person with acute alcohol and benzodiazepine withdrawal is sent home from the ER with a bottle of lorazepam and advised how to detoxify themselves. They go home and take the entire bottle to get high.
3. A person with alcoholism and depression is admitted for suicidal behavior. She was intoxicated, depressed and staring at a handgun. The next day the attending physician is contacted by a psychiatrist/utilization reviewer from the insurance company who has concluded the patient is no longer suicidal and they can be discharged. He will no longer authorize payment for inpatient treatment.
4. A pharmacy benefit manager refused to refill a 2 week prescription by a patient's psychiatrist. They have the pharmacist faxes a form to the psychiatrists office saying that they will only accept a 3 month prescription. The psychiatrist takes time to explain first to the pharmacists and then 2 different people at the PBM (total time 30 minutes) the rationale for not giving a large supply of medication to a chronically suicidal patient. The PBM refuses to change their position.
5. A managed care company refuses to cover psychotherapy provided by a psychiatrist. The psychiatrist explains that he is an expert in this type of therapy and the patient has been referred to him by the patient's primary psychiatrist. The managed care company authorizes 3 "crisis sessions".
6. A person completes a PHQ-9 scale in their primary care clinic and they score an 18. They see their primary care physician and say they would like to see a therapist. They are told to take an antidepressant and to come back in two weeks to fill out another PHQ-9. Total time of the visit is 5 minutes.
7. A person is seen in their primary care clinic and in 20 minutes is told by their nonpsychiatric physician that they have bipolar disorder. They are prescribed quetiapine, citalopram, and divalproex. Within several days they are too sedated to function at work.
The are just a few examples of thousands of people everyday who are receiving grossly inadequate care based on a specific ethical principle of physician behavior. That is the physician makes an assessment and prescribes care in what he or she believes is the best interest of the patient. That is the contract. There is no insurance company or government bureaucrat involved. There is no restricted access to mental health care or pretending that primary care physicians are psychiatrists. There is no remote "assessment" by a physician employed by a managed care company that prioritizes the financial well being of that insurance company or pharmacy benefit manager over the patient. In fact, I do not understand how that is ethical behavior at all.
That is the basis of the decline of psychiatry in this country. It has taken a proportionately larger hit than any other specialty. It is documented in detail on this blog and in E. Fuller Torrey's recent book. The adventures or misadventures of academic psychiatrists are relevant only insofar as the APA seems to use the President of the APA as a position that academics cycle in and out of. The idea that "psychiatrists in the trenches" are poorly represented by such a system is accurate with two possible exceptions that I can think of. Psychiatrists in the trenches are also poorly represented by criticism of academic psychiatrists and their conflict of interest agreements and personal employment contracts. It does nothing to address the central problems of the specialty, provides no tools that front line psychiatrist can use against all of the real conflicts of interest they face on a day by day basis, and is generally demoralizing. Before any critics suggest that I am supporting a "whitewash" - put yourself in the position of a psychiatrist who has just put in a 12 hour day taking care of 20 inpatients and putting up with passive aggressive and aggressive MCO and PBM reviewers who have been wasting your time and interfering with your care. You go home to read the paper and suddenly there is a major story of how unethical psychiatrists are - based on the appearance of conflict of interest. You try to remember that last time you saw a CME event that was sponsored by a pharmaceutical company. Then you check your files to make sure you have enough CME credits for relicensure. As an added piece of information that same psychiatrist doesn't really care about Section 3 in the DSM-5 or the issue of dimensional versus categorical diagnoses. They have not blinked an eye with the release of DSM-5 and won't in the future.
That is how the psychiatrist in the trenches experiences this academic exercise in conflict of interest. I say if you want to pull out an ethical argument and use that to help front line psychiatrists, it needs to be focused on the obvious targets in managed care and the government bureaucracies that support them.
You know - the real forces dismantling psychiatry (very effectively I might add) over the past three decades.
George Dawson, MD, DFAPA
Wednesday, January 1, 2014
The Real Conflicts of Interest in Medicine and Psychiatry Today
I noticed some confusion around the GSK article that was recently posted. I decided to start the New Year examining conflicts of interest (COI) in medicine and psychiatry because they are widespread. These COI are much more widespread than the press or politicians have stated. That is because there are more players than physicians involved and these other players are hardly ever mentioned. You would never realize that by reading the papers largely because COI is always described as a problem with physicians. Nothing could be further from the truth.
My goal is to outline as many as possible and hopefully readers here will be able to fill in any that I might have missed. Because I am just one guy working in his spare time, it will not be an encyclopedic listing but it will be more comprehensive than you will find anywhere in the press or possibly the existing medical literature. It will also be more comprehensive than the typical political analysis that usually suggests that the only relevant conflicts of interest have to do with physicians making money or prescribing drugs in exchange for certain rewards. As you will see, these may be some of the least important conflicts of interest.
A good starting point is this diagram I made that looks at all of the important conflicts of interest that impinge on physicians. The diagram is not exhaustive. (click to enlarge)
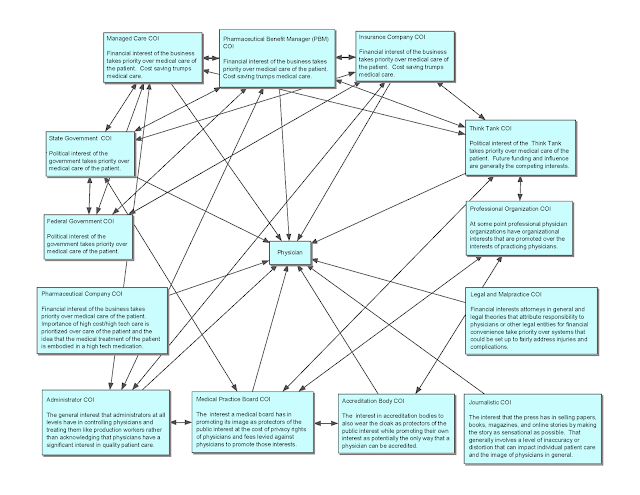
Not all of the links are drawn and there are many smaller entities involved that have not been graphed. As you can see I have 13 major areas here that directly impact on physicians. It is important to keep in mind the main goal or interest is the practice of medicine. It flows from an ethical relationship with a physician. That relationship is defined as the physician acting toward the patient in a way that is only in the best interest of the patient in exchange for a professional fee. The modern relationship makes an important distinction in that the physician needs to be practicing scientific medicine. The American Psychiatric Association (APA) has a policy statement with some useful definitions. The APA defines the primary interest as "the highest level of evidence based practice, ethically based and scientifically valid research, and quality continuing education for the benefit of patients, the profession and society." They define secondary or personal interests such as personal, financial, or professional that: "may inhibit, distract, or unduly influence their (physicians) judgment or behavior in a manner that detracts from or subordinates the primary interest of patients and may be perceived by some as undermining public trust." Six examples of situations that may require vigilance to prevent conflict of interest issues are given and 5 of 6 can be seen as derivative of physician relationships with the pharmaceutical industry.
The Institute of Medicine (IOM) definition of conflict of interest is: "a set of circumstances that creates a risk that professional judgment or actions regarding a primary interest will be unduly influenced by a secondary interest." Note that the IOM makes no distinction about conflict of interest versus the appearance of conflict of interest. It turns out that the appearance of conflict of interest is the common standard that is used to indict the medical profession. The classic example that is typically given in the media is the influence of pharmaceutical representatives on physician prescribing behavior. The recent GSK disclosure confirms that that pharmaceutical representatives were paid based on the number of product prescriptions that the physicians they visited actually wrote. The idea is that promotional items of widely variable value (pens to pizza to golf outings to trips) and free samples led to increased prescriptions. Free samples provided to clinics was probably also a major factor and became a mainstay for many patients with limited or no mental health benefits. Typical press coverage suggests that the results of this type of conflict of interest are widespread and certain, but I would suggest that the great majority of physicians including many of those who were paid consultants by the pharmaceutical industry were not laboring under any conflict of interest.
Consider for a moment the conflicts of interest (COI) listed across the top of the diagram starting on the left with Managed Care COI. I have reviewed those conflicts of interest in great detail in previous posts. As an example consider the conflicts of interest in this post on how physician employees are managed by managed care companies. In all cases, there is a direct conflict of interest between physicians interest and the interest of the company and its managers. In every situation that I am aware of the physicians lose. That is typically viewed as a plus by the business managers running the company because it allows them to do whatever they want to do in terms of closing clinics and programs, firing physicians, firing support staff, coming up with business based performance metrics that are divorced from clinical reality, and denying care when they want to. When the conflict is framed as entitled doctors being managed for the first time in order to be fiscally responsible - apart from the obvious rhetoric the real impact on patients is lost. That has included the rationing of psychiatric services, the destruction of inpatient psychiatry services, the elimination of psychotherapy services, and the wholesale shifting of care for people with the severest forms of mental illness to deficient state operated services and correctional facilities.
Managed Care COI is almost always transacted by an army of intermediaries. There are so-called physician reviewers or utilization reviewers who look at records from a distance and second guess physicians actually treating the patient. They can say that they don't think a patient needs a particular service such as hospitalization and the patient is invariably discharged. These days many hospitals owned by managed care companies employ non-physician case managers who function the same as utilization reviewers and tell physicians when to discharge patients from the hospital. This review process represents what I consider to be the largest conflict of interest affecting the decision making process in medicine and it is the least transparent. You are not likely to hear about it until you or a family member are hospitalized and you are told that it is "time to go" based on an insurance company decision. You can see from the diagram that this COI is enmeshed with federal and state governments, think tanks, and some of the other managed care rationing tactics - Pharmaceutical Benefit Manager COI and Insurance Company COI. All of these bureaucracies can produce insurmountable obstacles to physicians trying to care for patients by denying diagnostic and treatment modalities and denying appropriate settings for care.
Staying on the Managed Care COI for a moment what do some of the other relationships imply? A full description of those relationships would require several books to explain. This all started about 30 years ago as a concerted anti-physician movement. Several political forces had an interest in making the argument that the reason for the high cost of American medicine was that physicians were greedy and they did too many procedures. The federal government set up a complex subjective billing and coding system to slow down physicians. It was a mechanism that could be used to investigate and prosecute anyone who seemed to be billing too much. They initially enforced these totally subjective rules with the FBI. At some point in the late 1990s, they allowed managed care organizations to internalize this process and control over physicians using this mechanism was handed off to managed care. Today it allows a managed care companies to look at the documentation of patient care, decide that the notes don't meet criteria for a certain bill, and retrospectively demand payment for reimbursed services based on the number of other people seen for that problem. The relationship between managed care companies and governments allows them to reimburse whatever they want for a service and demand back as much as they want. No other professionals have private industry and governments stacked against them in this manner. It is a motivating force for psychiatrists to not accept government backed insurance at a higher rate than other physicians.
Managed Care COI also means that it is practically impossible for a physician to appeal a decision by a managed care company. The appeal is to another doctor who is employed by that company. Any attempt to go outside of the company to a state insurance board is usually not productive. State insurance boards are after all generally run by political appointees who are insurance industry insiders. There are no neutral parties who are free of conflict of interest who can decide an appeal of an insurance company decision.
Practically all of the major entities represented on this chart operate in a similar manner to the managed care and insurance company conflicts of interest. They are business entities who have woven themselves deeply into the political system at all levels and they can generally do what they want to do in terms of running the US Health Care system. In most cases they treat physicians with impunity and tolerate professional groups only so far as they can co-opt some of their ideas and make it seem like they have an interest in quality care. They have also used their influence to introduce cost-effectiveness rhetoric into places where it makes no sense. That is especially true for psychiatric services where many have simply been shut down because they were not "cost-effective" enough.
Some of the other entities on the diagram are more subtle. Journalistic COI has a few sources. Certainly journalists have no interest in patient care or treatment standards. They do have an interest in selling stories and in some cases books. They have an interest in influencing people. Many of the stories I have commented on this blog over the past year were clearly rhetorical. Many were also the product of ignorance. Psychiatry is the only field in medicine, where non-experts don't hesitate to put their opinion in the New York Times and the New York Times doesn't hesitate to print it. One of the most read posts on this blog in the past year was about a Washington Post article that I critiqued for many of these reasons.
Professional Organization COI is also an interesting one. Consider the APA represents roughly 40,000 psychiatrists but only about 40% are actual members. When the American Board of Medical Specialties decided that they would introduce a new and onerous procedure to certify physicians in an ongoing manner instead of for life, the APA clearly sided with the ABMS despite widespread dissatisfaction by the membership. The conflict of interest considerations here are considerable and heavily financial. There is no scientific evidence that the proposed ABMS recertification process is a valid approach. There is certainly no evidence that a less onerous approach that would be less stressful to physicians would not achieve the goal of ongoing professional education and public safety.
The next time you read a story in the press about wealthy physicians being paid off to prescribe unnecessary medications or to perform unnecessary surgeries, pull up the COI diagram and print it out. The truth is that physicians are caught in a web of conflict of interest. Those conflicts of interest are generally set up to ration services to patients; ration or deny reimbursement to physicians; maximize the profits of middlemen (MCOs, HMOs, PBMs, Insurance companies); make politicians, think tanks, journalists and critics look good; and distribute a large chunk of the health care dollar to people who are not involved in providing the services. The impact is the greatest by far in the area of psychiatric services but at some level it affects all of medicine. The impact on physicians is also significant. All of the pressures on physicians as a result of these conflicts of interest widen dissatisfaction with the field and increase burnout. Both of those factors can potentially impact physician availability and intellectual resources necessary for optimal performance. So if your physician looks burned out - he or she may well be. It is probably directly related to doing an additional 2 or 3 hours of work every day to satisfy the requirements of all of these extraneous conflicts of interest. Of course that is all generally unreimbursed time. How would most workers react to putting in a full day and then an additional 2 - 3 hours off the clock to satisfy the requirements of some outside company? It is like working for free for another company.
That is the real cost of conflict of interest and one of the reasons that health care premiums are essentially another tax on all Americans.
Happy New Year!
George Dawson, MD, DFAPA
Institute of Medicine (US) Committee on Conflict of Interest in Medical Research, Education, and Practice; Lo B, Field MJ, editors. Conflict of Interest in Medical Research, Education, and Practice. Washington (DC): National Academies Press (US); 2009. Available from: http://www.ncbi.nlm.nih.gov/books/NBK22942/
My goal is to outline as many as possible and hopefully readers here will be able to fill in any that I might have missed. Because I am just one guy working in his spare time, it will not be an encyclopedic listing but it will be more comprehensive than you will find anywhere in the press or possibly the existing medical literature. It will also be more comprehensive than the typical political analysis that usually suggests that the only relevant conflicts of interest have to do with physicians making money or prescribing drugs in exchange for certain rewards. As you will see, these may be some of the least important conflicts of interest.
A good starting point is this diagram I made that looks at all of the important conflicts of interest that impinge on physicians. The diagram is not exhaustive. (click to enlarge)

Not all of the links are drawn and there are many smaller entities involved that have not been graphed. As you can see I have 13 major areas here that directly impact on physicians. It is important to keep in mind the main goal or interest is the practice of medicine. It flows from an ethical relationship with a physician. That relationship is defined as the physician acting toward the patient in a way that is only in the best interest of the patient in exchange for a professional fee. The modern relationship makes an important distinction in that the physician needs to be practicing scientific medicine. The American Psychiatric Association (APA) has a policy statement with some useful definitions. The APA defines the primary interest as "the highest level of evidence based practice, ethically based and scientifically valid research, and quality continuing education for the benefit of patients, the profession and society." They define secondary or personal interests such as personal, financial, or professional that: "may inhibit, distract, or unduly influence their (physicians) judgment or behavior in a manner that detracts from or subordinates the primary interest of patients and may be perceived by some as undermining public trust." Six examples of situations that may require vigilance to prevent conflict of interest issues are given and 5 of 6 can be seen as derivative of physician relationships with the pharmaceutical industry.
The Institute of Medicine (IOM) definition of conflict of interest is: "a set of circumstances that creates a risk that professional judgment or actions regarding a primary interest will be unduly influenced by a secondary interest." Note that the IOM makes no distinction about conflict of interest versus the appearance of conflict of interest. It turns out that the appearance of conflict of interest is the common standard that is used to indict the medical profession. The classic example that is typically given in the media is the influence of pharmaceutical representatives on physician prescribing behavior. The recent GSK disclosure confirms that that pharmaceutical representatives were paid based on the number of product prescriptions that the physicians they visited actually wrote. The idea is that promotional items of widely variable value (pens to pizza to golf outings to trips) and free samples led to increased prescriptions. Free samples provided to clinics was probably also a major factor and became a mainstay for many patients with limited or no mental health benefits. Typical press coverage suggests that the results of this type of conflict of interest are widespread and certain, but I would suggest that the great majority of physicians including many of those who were paid consultants by the pharmaceutical industry were not laboring under any conflict of interest.
Consider for a moment the conflicts of interest (COI) listed across the top of the diagram starting on the left with Managed Care COI. I have reviewed those conflicts of interest in great detail in previous posts. As an example consider the conflicts of interest in this post on how physician employees are managed by managed care companies. In all cases, there is a direct conflict of interest between physicians interest and the interest of the company and its managers. In every situation that I am aware of the physicians lose. That is typically viewed as a plus by the business managers running the company because it allows them to do whatever they want to do in terms of closing clinics and programs, firing physicians, firing support staff, coming up with business based performance metrics that are divorced from clinical reality, and denying care when they want to. When the conflict is framed as entitled doctors being managed for the first time in order to be fiscally responsible - apart from the obvious rhetoric the real impact on patients is lost. That has included the rationing of psychiatric services, the destruction of inpatient psychiatry services, the elimination of psychotherapy services, and the wholesale shifting of care for people with the severest forms of mental illness to deficient state operated services and correctional facilities.
Managed Care COI is almost always transacted by an army of intermediaries. There are so-called physician reviewers or utilization reviewers who look at records from a distance and second guess physicians actually treating the patient. They can say that they don't think a patient needs a particular service such as hospitalization and the patient is invariably discharged. These days many hospitals owned by managed care companies employ non-physician case managers who function the same as utilization reviewers and tell physicians when to discharge patients from the hospital. This review process represents what I consider to be the largest conflict of interest affecting the decision making process in medicine and it is the least transparent. You are not likely to hear about it until you or a family member are hospitalized and you are told that it is "time to go" based on an insurance company decision. You can see from the diagram that this COI is enmeshed with federal and state governments, think tanks, and some of the other managed care rationing tactics - Pharmaceutical Benefit Manager COI and Insurance Company COI. All of these bureaucracies can produce insurmountable obstacles to physicians trying to care for patients by denying diagnostic and treatment modalities and denying appropriate settings for care.
Staying on the Managed Care COI for a moment what do some of the other relationships imply? A full description of those relationships would require several books to explain. This all started about 30 years ago as a concerted anti-physician movement. Several political forces had an interest in making the argument that the reason for the high cost of American medicine was that physicians were greedy and they did too many procedures. The federal government set up a complex subjective billing and coding system to slow down physicians. It was a mechanism that could be used to investigate and prosecute anyone who seemed to be billing too much. They initially enforced these totally subjective rules with the FBI. At some point in the late 1990s, they allowed managed care organizations to internalize this process and control over physicians using this mechanism was handed off to managed care. Today it allows a managed care companies to look at the documentation of patient care, decide that the notes don't meet criteria for a certain bill, and retrospectively demand payment for reimbursed services based on the number of other people seen for that problem. The relationship between managed care companies and governments allows them to reimburse whatever they want for a service and demand back as much as they want. No other professionals have private industry and governments stacked against them in this manner. It is a motivating force for psychiatrists to not accept government backed insurance at a higher rate than other physicians.
Managed Care COI also means that it is practically impossible for a physician to appeal a decision by a managed care company. The appeal is to another doctor who is employed by that company. Any attempt to go outside of the company to a state insurance board is usually not productive. State insurance boards are after all generally run by political appointees who are insurance industry insiders. There are no neutral parties who are free of conflict of interest who can decide an appeal of an insurance company decision.
Practically all of the major entities represented on this chart operate in a similar manner to the managed care and insurance company conflicts of interest. They are business entities who have woven themselves deeply into the political system at all levels and they can generally do what they want to do in terms of running the US Health Care system. In most cases they treat physicians with impunity and tolerate professional groups only so far as they can co-opt some of their ideas and make it seem like they have an interest in quality care. They have also used their influence to introduce cost-effectiveness rhetoric into places where it makes no sense. That is especially true for psychiatric services where many have simply been shut down because they were not "cost-effective" enough.
Some of the other entities on the diagram are more subtle. Journalistic COI has a few sources. Certainly journalists have no interest in patient care or treatment standards. They do have an interest in selling stories and in some cases books. They have an interest in influencing people. Many of the stories I have commented on this blog over the past year were clearly rhetorical. Many were also the product of ignorance. Psychiatry is the only field in medicine, where non-experts don't hesitate to put their opinion in the New York Times and the New York Times doesn't hesitate to print it. One of the most read posts on this blog in the past year was about a Washington Post article that I critiqued for many of these reasons.
Professional Organization COI is also an interesting one. Consider the APA represents roughly 40,000 psychiatrists but only about 40% are actual members. When the American Board of Medical Specialties decided that they would introduce a new and onerous procedure to certify physicians in an ongoing manner instead of for life, the APA clearly sided with the ABMS despite widespread dissatisfaction by the membership. The conflict of interest considerations here are considerable and heavily financial. There is no scientific evidence that the proposed ABMS recertification process is a valid approach. There is certainly no evidence that a less onerous approach that would be less stressful to physicians would not achieve the goal of ongoing professional education and public safety.
The next time you read a story in the press about wealthy physicians being paid off to prescribe unnecessary medications or to perform unnecessary surgeries, pull up the COI diagram and print it out. The truth is that physicians are caught in a web of conflict of interest. Those conflicts of interest are generally set up to ration services to patients; ration or deny reimbursement to physicians; maximize the profits of middlemen (MCOs, HMOs, PBMs, Insurance companies); make politicians, think tanks, journalists and critics look good; and distribute a large chunk of the health care dollar to people who are not involved in providing the services. The impact is the greatest by far in the area of psychiatric services but at some level it affects all of medicine. The impact on physicians is also significant. All of the pressures on physicians as a result of these conflicts of interest widen dissatisfaction with the field and increase burnout. Both of those factors can potentially impact physician availability and intellectual resources necessary for optimal performance. So if your physician looks burned out - he or she may well be. It is probably directly related to doing an additional 2 or 3 hours of work every day to satisfy the requirements of all of these extraneous conflicts of interest. Of course that is all generally unreimbursed time. How would most workers react to putting in a full day and then an additional 2 - 3 hours off the clock to satisfy the requirements of some outside company? It is like working for free for another company.
That is the real cost of conflict of interest and one of the reasons that health care premiums are essentially another tax on all Americans.
Happy New Year!
George Dawson, MD, DFAPA
Institute of Medicine (US) Committee on Conflict of Interest in Medical Research, Education, and Practice; Lo B, Field MJ, editors. Conflict of Interest in Medical Research, Education, and Practice. Washington (DC): National Academies Press (US); 2009. Available from: http://www.ncbi.nlm.nih.gov/books/NBK22942/
Saturday, December 21, 2013
GSK Eliminates Appearance of Conflict of Interest - Who Is Next?
Glaxo Smith Kline came out with a major announcement a few days ago. It will no longer pay doctors to promote its drugs and it will no longer tie the compensation of its sales force to the number of prescriptions written by doctors who have been detailed about those drugs. These are both standard practices in the pharmaceutical industry and this is the first announcement of its kind within the industry. GSK will continue to to provide "unsolicited independent educational grants" to educational institutions or medical societies. Pharmaceutical reps will be paid on the basis of technical knowledge and customer service rather than sales. GSK has been fined heavily lately about promoting off label use of its products and is currently under investigation in China.
My immediate reaction to the piece was "good riddance". For the past decade there has been no bigger issue in psychiatry than the appearance of conflict of interest with the pharmaceutical industry. Psychiatry has been targeted more than any other medical specialty by prominent politicians, the news media, and even by psychiatrists themselves. There are endless blogs and opinion pieces about how the practice of psychiatry has been defined by this appearance of conflict of interest. There are several blogs out there that have gained prominence by endlessly reviewing all of these details. It has affected the way the APA does business. It has affected the way local district branches do business. In the end the politicians are grandstanding on it, because the PPACA (Obamacare) will apparently list any physician receiving money from a pharmaceutical company. That was suggested as a motivating factor in the NY Times article. Those public lists have existed in some states like the one I have practiced in for years.
To me the arguments have always come down to advertising and ethics. From an advertising perspective would we expect people to be affected by product advertising? Of course we would. The buying habits of the American population are shaped by advertising. Selling products is more of a science than people think. The American public can easily change its buying habits and can purchase products that are unnecessary and will be discarded after a brief period of time. They can also be sold on products like junk food that are unhealthy but designed to be sold in large quantities. Advertising would not seem to be the ideal basis for marketing drugs to physicians, but with many new products physicians are now bypassed and the drug is sold directly to the consumer. If the epidemiology of a particular problem like "low-T" is known, direct-to-consumer marketing probably leads to many, many more physician visits than a physician suggesting to their patient that they probably have primary or hypogonadotropic hypogonadism. All a patient has to do is go to the web site and take a non-specific checklist quiz on the features of "low-T" and be in their doctor's office to get the levels done within a week. Things will probably go a lot smoother without a physician intermediary in the loop and I am sure that much physician behavior will be shaped by the onslaught of men coming in to be tested for "low-T". I know for a fact that psychiatrists are approached for this problem because of the overlap between the syndrome and depression.
Part of the advertising argument has always been that there are unconscious factors in play. Really? That is the basis for all advertising in general. The main difference has been that pharmaceutical representatives have been schooled on the relationship aspects of the sale. They have been taught that basically if a physician likes them or feels indebted to them for free food, trinkets like poor quality pens that never seem to write very well, a round of golf, or tickets to the Lakers game that they may be more likely to prescribe their product. Most physicians were apparently naive enough to not realize that there was a huge marketing database out there that tracked their prescription writing to see if they were writing the required number of prescriptions for that product. In the real heyday of marketing bonuses to physicians, companies would pay for travel to important meetings.
While the people focused on the advertising influence kept chipping away mostly at psychiatrists, they seemed to ignore two important developments that made detailing or selling to individual physicians much less relevant. The first was restricted formularies. I was on the Pharmacy and Therapeutics Committee (P&T) of one of the largest health plans in the state and an affiliated hospital for a total of 10 years. During that time, the predominant factor in the decision about whether to put a drug on a formulary that would make it available to prescribing physicians was the cost. There were very few instances where a drug was so unique that it was made available even if it was very expensive. In those cases a drug might be available for an incurable illness that had a negligible benefit but it was included basically for public relations. One of the other overriding themes of the P & T Committee was that all drugs in a particular class (like antidepressants) were equivalent and therefore the least expensive drug in the class could be substituted for anything else. This potentially led to a lot of unnecessary chaos when medications fell out of favor due to pricing and patients needed to be shifted en masse to the least expensive drug. It gave hospitals and health plans leverage in dealing with pharmaceutical companies, but in some cases the deals were complex. As an example, in order to get a new blockbuster drug at a good price, the health plan would need to accept the same company's generic in a different class that had been removed because it was considered too expensive. Over a decade ago, business entrepreneurs decided that there was money to be made rationing medications to health plan enrollees and now a lot of that is done by pharmaceutical benefit managers (PBMs). PBMs are currently a multibillion dollar industry.
The second important development was generic drugs. Practically all of the blockbuster psychiatric medications of the past two decades are now generic drugs. Many generic drugs are easily affordable even as direct out of pocket purchases. At that point they are no longer actively marketed by the pharmaceutical company that held the exclusive patents. They are more likely to be the preferred drugs of PBMs and health plan formularies. They are in that role because of a scientific approximation. That approximation is that all drugs in a certain class, like antidepressants that have the same purported mechanism of action are equivalent and one can be substituted for another. That is clearly false but it allows the health plan to to provide you with the least expensive medication or charge you a hefty copay for one that is not. It also seems to not consider after market information that can even affect generic drugs. The best example I can think of there is the FDA warnings on citalopram. I would guess that despite the warnings, it remains a preferred drug by most health plans. Health plans in general seem to be geared up to prescribe antidepressants at higher and higher rates. I would take it a step further and venture a guess that most health plans have not taken a look at the data in their systems on whether or not they have observed problems related to the FDA warning on citalopram.
The ethical argument goes something like this. Physicians should have the best interests of their patients in mind and an advertising based conflict-of-interest to prescribe a certain drug creates an ethical concern. On the face of it, it seems like a straightforward argument. But there are several problems with it. For example, what is the direct evidence that this occurs - if any? Is it really believable that a physician would prescribe a decidedly suboptimal medication to a patient based on schmoozing with a pharmaceutical representative? There are often other factors in play. It is common to treat people with chronic illnesses who have suboptimal response to the current therapy and who are looking for the "next biggest thing" to try. A physician who has been detailed on the "next biggest thing" is likely to prescribe it if asked. There is a similar dynamic with the issue of overprescribing in general. If a patient persists in their request for an opioid, an antibiotic, a stimulant or any other drug are they likely to get it? The recent declaration that the CDC initiative to decrease antibiotic prescribing has failed would suggest that they will. Finally there is the dynamic of "see the doctor and leave with a pill." There are any number of scenarios where medications are used in medical practice and other options are not even discussed. The psychiatric cases are highlighted but it happens as frequently in cases of mild diabetes mellitus, back pain, chronic pain of various causes, hypercholesterolemia, mild hypertension and others. Many people have described this as "the doctor was poised over his prescription pad" but the healthcare industry is set up to see people in brief medication focused visits and physician reimbursement is tied to it. There are also patient related factors and a recent Tom Hanks interview is illustrative. He was on a late night talk show discussing his recent diagnosis of diabetes mellitus and he said his physician told him that if he could get back to his high school body weight he probably would not have it. His reply was: "Well I'm going to have Type II diabetes."
The ethical arguments, especially the ones I have seen constructed by physicians also ignore the general case of conflicts of interest at the professional level. Practically every major university department allows its faculty to supplement their salaries by consulting in private industry. In many cases that is a major source of additional income. In some cases those professionals are involved in setting standards and their approach is much different than the wall that is currently being constructed between the medical profession and the pharmaceutical industry. As an example, academic and industry professionals within the engineering profession are often on committees responsible for setting standards that govern all of the products within that industry. Their approach is to include as many industry professionals as necessary rather than suggesting the academics can set the standards themselves. Considering that pharmaceutical companies employ some of the top scientists in the world it would seem that medicine has a lot to lose if it goes along with the prevailing assumption. The prevailing assumption is that physicians are powerless to stop prescribing expensive medications that are of questionable benefit for their patients based solely on advertising and no scientific merit.
I applaud the GSK decision even though the above cited factors would suggest that for most physicians it has only historical relevance. I would encourage all of Big Pharma to adopt the same policies toward physicians. But this doesn't really go far enough and it is basically a token gesture at this point. To really make a difference I would suggest that they stop giving money to politicians. GSK spent $1.9 million on candidates and $4.9 million in lobbying last year. All of that money was directed at a few politicians. It is a part of a massive industry wide contribution to politicians. What do you think buys more influence, giving free pizza and pens to doctors or giving thousands to tens of thousands of dollars to politicians?
George Dawson, MD, DFAPA
Katie Thomas. Glaxo Says It Will Stop Paying Doctors To Promote Drugs. New York Times December 16, 2013.
My immediate reaction to the piece was "good riddance". For the past decade there has been no bigger issue in psychiatry than the appearance of conflict of interest with the pharmaceutical industry. Psychiatry has been targeted more than any other medical specialty by prominent politicians, the news media, and even by psychiatrists themselves. There are endless blogs and opinion pieces about how the practice of psychiatry has been defined by this appearance of conflict of interest. There are several blogs out there that have gained prominence by endlessly reviewing all of these details. It has affected the way the APA does business. It has affected the way local district branches do business. In the end the politicians are grandstanding on it, because the PPACA (Obamacare) will apparently list any physician receiving money from a pharmaceutical company. That was suggested as a motivating factor in the NY Times article. Those public lists have existed in some states like the one I have practiced in for years.
To me the arguments have always come down to advertising and ethics. From an advertising perspective would we expect people to be affected by product advertising? Of course we would. The buying habits of the American population are shaped by advertising. Selling products is more of a science than people think. The American public can easily change its buying habits and can purchase products that are unnecessary and will be discarded after a brief period of time. They can also be sold on products like junk food that are unhealthy but designed to be sold in large quantities. Advertising would not seem to be the ideal basis for marketing drugs to physicians, but with many new products physicians are now bypassed and the drug is sold directly to the consumer. If the epidemiology of a particular problem like "low-T" is known, direct-to-consumer marketing probably leads to many, many more physician visits than a physician suggesting to their patient that they probably have primary or hypogonadotropic hypogonadism. All a patient has to do is go to the web site and take a non-specific checklist quiz on the features of "low-T" and be in their doctor's office to get the levels done within a week. Things will probably go a lot smoother without a physician intermediary in the loop and I am sure that much physician behavior will be shaped by the onslaught of men coming in to be tested for "low-T". I know for a fact that psychiatrists are approached for this problem because of the overlap between the syndrome and depression.
Part of the advertising argument has always been that there are unconscious factors in play. Really? That is the basis for all advertising in general. The main difference has been that pharmaceutical representatives have been schooled on the relationship aspects of the sale. They have been taught that basically if a physician likes them or feels indebted to them for free food, trinkets like poor quality pens that never seem to write very well, a round of golf, or tickets to the Lakers game that they may be more likely to prescribe their product. Most physicians were apparently naive enough to not realize that there was a huge marketing database out there that tracked their prescription writing to see if they were writing the required number of prescriptions for that product. In the real heyday of marketing bonuses to physicians, companies would pay for travel to important meetings.
While the people focused on the advertising influence kept chipping away mostly at psychiatrists, they seemed to ignore two important developments that made detailing or selling to individual physicians much less relevant. The first was restricted formularies. I was on the Pharmacy and Therapeutics Committee (P&T) of one of the largest health plans in the state and an affiliated hospital for a total of 10 years. During that time, the predominant factor in the decision about whether to put a drug on a formulary that would make it available to prescribing physicians was the cost. There were very few instances where a drug was so unique that it was made available even if it was very expensive. In those cases a drug might be available for an incurable illness that had a negligible benefit but it was included basically for public relations. One of the other overriding themes of the P & T Committee was that all drugs in a particular class (like antidepressants) were equivalent and therefore the least expensive drug in the class could be substituted for anything else. This potentially led to a lot of unnecessary chaos when medications fell out of favor due to pricing and patients needed to be shifted en masse to the least expensive drug. It gave hospitals and health plans leverage in dealing with pharmaceutical companies, but in some cases the deals were complex. As an example, in order to get a new blockbuster drug at a good price, the health plan would need to accept the same company's generic in a different class that had been removed because it was considered too expensive. Over a decade ago, business entrepreneurs decided that there was money to be made rationing medications to health plan enrollees and now a lot of that is done by pharmaceutical benefit managers (PBMs). PBMs are currently a multibillion dollar industry.
The second important development was generic drugs. Practically all of the blockbuster psychiatric medications of the past two decades are now generic drugs. Many generic drugs are easily affordable even as direct out of pocket purchases. At that point they are no longer actively marketed by the pharmaceutical company that held the exclusive patents. They are more likely to be the preferred drugs of PBMs and health plan formularies. They are in that role because of a scientific approximation. That approximation is that all drugs in a certain class, like antidepressants that have the same purported mechanism of action are equivalent and one can be substituted for another. That is clearly false but it allows the health plan to to provide you with the least expensive medication or charge you a hefty copay for one that is not. It also seems to not consider after market information that can even affect generic drugs. The best example I can think of there is the FDA warnings on citalopram. I would guess that despite the warnings, it remains a preferred drug by most health plans. Health plans in general seem to be geared up to prescribe antidepressants at higher and higher rates. I would take it a step further and venture a guess that most health plans have not taken a look at the data in their systems on whether or not they have observed problems related to the FDA warning on citalopram.
The ethical argument goes something like this. Physicians should have the best interests of their patients in mind and an advertising based conflict-of-interest to prescribe a certain drug creates an ethical concern. On the face of it, it seems like a straightforward argument. But there are several problems with it. For example, what is the direct evidence that this occurs - if any? Is it really believable that a physician would prescribe a decidedly suboptimal medication to a patient based on schmoozing with a pharmaceutical representative? There are often other factors in play. It is common to treat people with chronic illnesses who have suboptimal response to the current therapy and who are looking for the "next biggest thing" to try. A physician who has been detailed on the "next biggest thing" is likely to prescribe it if asked. There is a similar dynamic with the issue of overprescribing in general. If a patient persists in their request for an opioid, an antibiotic, a stimulant or any other drug are they likely to get it? The recent declaration that the CDC initiative to decrease antibiotic prescribing has failed would suggest that they will. Finally there is the dynamic of "see the doctor and leave with a pill." There are any number of scenarios where medications are used in medical practice and other options are not even discussed. The psychiatric cases are highlighted but it happens as frequently in cases of mild diabetes mellitus, back pain, chronic pain of various causes, hypercholesterolemia, mild hypertension and others. Many people have described this as "the doctor was poised over his prescription pad" but the healthcare industry is set up to see people in brief medication focused visits and physician reimbursement is tied to it. There are also patient related factors and a recent Tom Hanks interview is illustrative. He was on a late night talk show discussing his recent diagnosis of diabetes mellitus and he said his physician told him that if he could get back to his high school body weight he probably would not have it. His reply was: "Well I'm going to have Type II diabetes."
The ethical arguments, especially the ones I have seen constructed by physicians also ignore the general case of conflicts of interest at the professional level. Practically every major university department allows its faculty to supplement their salaries by consulting in private industry. In many cases that is a major source of additional income. In some cases those professionals are involved in setting standards and their approach is much different than the wall that is currently being constructed between the medical profession and the pharmaceutical industry. As an example, academic and industry professionals within the engineering profession are often on committees responsible for setting standards that govern all of the products within that industry. Their approach is to include as many industry professionals as necessary rather than suggesting the academics can set the standards themselves. Considering that pharmaceutical companies employ some of the top scientists in the world it would seem that medicine has a lot to lose if it goes along with the prevailing assumption. The prevailing assumption is that physicians are powerless to stop prescribing expensive medications that are of questionable benefit for their patients based solely on advertising and no scientific merit.
I applaud the GSK decision even though the above cited factors would suggest that for most physicians it has only historical relevance. I would encourage all of Big Pharma to adopt the same policies toward physicians. But this doesn't really go far enough and it is basically a token gesture at this point. To really make a difference I would suggest that they stop giving money to politicians. GSK spent $1.9 million on candidates and $4.9 million in lobbying last year. All of that money was directed at a few politicians. It is a part of a massive industry wide contribution to politicians. What do you think buys more influence, giving free pizza and pens to doctors or giving thousands to tens of thousands of dollars to politicians?
George Dawson, MD, DFAPA
Katie Thomas. Glaxo Says It Will Stop Paying Doctors To Promote Drugs. New York Times December 16, 2013.
Sunday, September 1, 2013
Happy Labor Day II - To All of the Docs on the Assembly Line
Last year I posted a Labor Day greeting to all of the docs laboring in American medicine. I used the assembly line metaphor for obvious reasons - physicians were no longer being treated like knowledge workers but were being treated like assembly line workers. Circumscribed patient visits were the widgets. In the case of proceduralists the procedure was the widget. One of my friends referred to himself as a "scope monkey" based on the expectation for the number of procedures he was supposed to produce every year. Have there been any substantial changes in the last year?
The bad news is that there have not been. Managed care continues to consolidate its monopoly. The final product under the Affordable Care Act (PPACA) will result in unprecedented leverage on the part of that industry over physicians and patients. I often compare the healthcare industry to the financial services industry when it comes to an example of government determined monopolies. The 401K is a great example of how this works. The 401K was sold to the American public as a great way to save for retirement. When the choices in 401K were limited it was sold as a way to simplify the 401K for most people. The truth about 401Ks is that they have not been a very successful investment vehicle. They put trillions of dollars of retiree savings at risk and the fees they charge are even more outrageous than medical fees. I just looked at a bond fund prospectus this morning that shows on an investment of $10,000 I could expect to pay $1,000 in fees every 10 years. Considering that there are about $9 trillion dollars in 401Ks and IRAs that generates about a trillion dollars in fees (about $90 billion a year) for the financial services industry. Those fees are generated independent of the general goal of retirement funds - actually having money for retirement. My prospectus has the usual disclaimer: "The value of your investment in the fund can go up or down. You can lose money by investing money in the fund." As many baby boomers found out that can be 30-40% of your principal.
How does managed care compare? The most interesting game has been the idea that all fees will increase substantially with the implementation of the PPACA. This bill allows for unprecedented merger and efficiencies. It allows for only 80% of the health care premium to be devoted to the actual provision of health care services. It is logical to assume that a greater percentage of the health care dollar devoted to health care would also decrease premiums. There will be significant hidden savings associated with a model of care that is integrated and minimizes the amount of physician billing. Insurance company rhetoric suggests that provided additional services to the uninsured with no limitations on pre-existing conditions will more than cancel out the monopoly advantages. If that was true why lobby for large monopolies?
One of the indicators to me of just how much leverage the managed care industry has is the expected out of pocket costs for a retired couple on Medicare. That number is currently $220,000 not including nursing home costs. That is roughly more than four times the average retirement savings for most Americans.
The financial services industry and the medical industry are basically government mandated hidden taxes on the American people. In exchange for that huge subsidy we get an industry that charges us significant fees to place our retirement funds at risk all of the time and another industry that rations health care and charges whatever they want in order to make money. In the case of the medical industry the overriding philosophy is not consistent with an enlightened approach to employees that probably know a lot more about the provision of quality medical services than the administrators.
That conflict of interest is central to the deterioration of the practice environment and a diminished focus on quality care and a continued focus of the study and academic aspects of medicine. Having medical care dictated by administrators using business guidelines or managed care reviewers using the same approach is demoralizing. Unless this conflict of interest is adequately addressed - the focus of health care will be turning out widgets. Only the widget producers will be valued. Administrators making arbitrary decisions run the whole show.
All of this remains decidedly grim in terms of the practice environment where most physicians work. It is only fair to consider some solutions. I will try to avoid the political decisions I have advanced in APA and other medical forums over the past 20 years. Physicians are uniquely oblivious to the fact that the science of medicine is routinely trumped by business and politics. Are there any possible solutions? For many years private practice was always considered an option. With the PPACA that route will be more difficult because the solo practitioners and groups will probably be off the network and professionally isolated, but some will be able to practice in this environment. There is still niche work where physicians can be paid professional salaries and still have adequate time to complete all of the administrative tasks and focus on quality work, but they are rare.
A single exciting model that I think can disrupt the usual managed care and government restrictions that I expect to flow from the PPACA comes from the University of Wisconsin and their Memory Clinics approach. This is a statewide network of clinics focused on providing state-of-the-art and quality care across a number of settings. Guidelines, continuing education, and consultation is provided from a University based department and there is a minimum requirement for for ongoing education every year. I don't see why this model cannot be widely applied across psychiatry and all other medical specialties. It brings the academic focus back into medicine instead of the current focus by governments and business. The practice environment of medicine needs this academic focus and it would greatly enhance the practice environment and get us out of widget production.
That is my hope between this Labor Day and the next.
George Dawson, MD, DFAPA
The bad news is that there have not been. Managed care continues to consolidate its monopoly. The final product under the Affordable Care Act (PPACA) will result in unprecedented leverage on the part of that industry over physicians and patients. I often compare the healthcare industry to the financial services industry when it comes to an example of government determined monopolies. The 401K is a great example of how this works. The 401K was sold to the American public as a great way to save for retirement. When the choices in 401K were limited it was sold as a way to simplify the 401K for most people. The truth about 401Ks is that they have not been a very successful investment vehicle. They put trillions of dollars of retiree savings at risk and the fees they charge are even more outrageous than medical fees. I just looked at a bond fund prospectus this morning that shows on an investment of $10,000 I could expect to pay $1,000 in fees every 10 years. Considering that there are about $9 trillion dollars in 401Ks and IRAs that generates about a trillion dollars in fees (about $90 billion a year) for the financial services industry. Those fees are generated independent of the general goal of retirement funds - actually having money for retirement. My prospectus has the usual disclaimer: "The value of your investment in the fund can go up or down. You can lose money by investing money in the fund." As many baby boomers found out that can be 30-40% of your principal.
How does managed care compare? The most interesting game has been the idea that all fees will increase substantially with the implementation of the PPACA. This bill allows for unprecedented merger and efficiencies. It allows for only 80% of the health care premium to be devoted to the actual provision of health care services. It is logical to assume that a greater percentage of the health care dollar devoted to health care would also decrease premiums. There will be significant hidden savings associated with a model of care that is integrated and minimizes the amount of physician billing. Insurance company rhetoric suggests that provided additional services to the uninsured with no limitations on pre-existing conditions will more than cancel out the monopoly advantages. If that was true why lobby for large monopolies?
One of the indicators to me of just how much leverage the managed care industry has is the expected out of pocket costs for a retired couple on Medicare. That number is currently $220,000 not including nursing home costs. That is roughly more than four times the average retirement savings for most Americans.
The financial services industry and the medical industry are basically government mandated hidden taxes on the American people. In exchange for that huge subsidy we get an industry that charges us significant fees to place our retirement funds at risk all of the time and another industry that rations health care and charges whatever they want in order to make money. In the case of the medical industry the overriding philosophy is not consistent with an enlightened approach to employees that probably know a lot more about the provision of quality medical services than the administrators.
That conflict of interest is central to the deterioration of the practice environment and a diminished focus on quality care and a continued focus of the study and academic aspects of medicine. Having medical care dictated by administrators using business guidelines or managed care reviewers using the same approach is demoralizing. Unless this conflict of interest is adequately addressed - the focus of health care will be turning out widgets. Only the widget producers will be valued. Administrators making arbitrary decisions run the whole show.
All of this remains decidedly grim in terms of the practice environment where most physicians work. It is only fair to consider some solutions. I will try to avoid the political decisions I have advanced in APA and other medical forums over the past 20 years. Physicians are uniquely oblivious to the fact that the science of medicine is routinely trumped by business and politics. Are there any possible solutions? For many years private practice was always considered an option. With the PPACA that route will be more difficult because the solo practitioners and groups will probably be off the network and professionally isolated, but some will be able to practice in this environment. There is still niche work where physicians can be paid professional salaries and still have adequate time to complete all of the administrative tasks and focus on quality work, but they are rare.
A single exciting model that I think can disrupt the usual managed care and government restrictions that I expect to flow from the PPACA comes from the University of Wisconsin and their Memory Clinics approach. This is a statewide network of clinics focused on providing state-of-the-art and quality care across a number of settings. Guidelines, continuing education, and consultation is provided from a University based department and there is a minimum requirement for for ongoing education every year. I don't see why this model cannot be widely applied across psychiatry and all other medical specialties. It brings the academic focus back into medicine instead of the current focus by governments and business. The practice environment of medicine needs this academic focus and it would greatly enhance the practice environment and get us out of widget production.
That is my hope between this Labor Day and the next.
George Dawson, MD, DFAPA
Wednesday, January 2, 2013
A Psychiatrist Reads the Washington Post
There are an endless number of ways that the appearance of
conflict of interest can be spun to make any organization look bad. The obvious question is why that always seems
to occur with psychiatry? The arguments
all follow the general form that a financial benefit resulting from work
related to the pharmaceutical industry disqualifies those experts from writing
objective research about medication or rendering opinions about the treatment
of psychiatric disorders in general. That is the theme of the latest article
from The Washington Post entitled “Antidepressants treat grief? Psychiatry
panelists with ties to drug industry say yes." It is an old story with little variation and
I add some commentary based on the organization of the article.
"In what some
prominent critics have called a bonanza for drug companies, the American
Psychiatric Association this month voted to drop the old wording against
diagnosing depression in the bereaved, opening the way for more of them to be
diagnosed with major depression and thus, treated with antidepressants.”
This statement assumes that this practice is not occurring
right now. In fact, it is widely known that the diagnosis of depression is not
rigorously made in primary care settings. It is highly likely right now that
patients suffering from grief as well as psychological adaptations to acute
stress are being treated with antidepressants. There is no reason to believe
that the patients being treated in primary care resemble the patients with a
diagnosis of major depression in clinical trials of antidepressants.
"The change in
the handbook, which could have significant financial implications for the $10
billion US antidepressant market, was developed in large part by people
affiliated with the pharmaceutical industry, an examination of financial
disclosures shows.”
The previous statement talks about a "bonanza for drug
companies" and builds on this image in the second statement. It ignores
the fact that most commonly prescribed antidepressants are currently generics
and available for as little as four dollars per month. The only two major
antidepressants at this time that are not generics are Cymbalta (duloxetine) and Vibryd
(vilazodone). Where does the "10
billion dollar" figure come from? If
you read the entire article on page 5, that figure was from IMS America a
company that tracks total prescriptions from American retail pharmacies. Anyone knowing the applications for
antidepressants would know that they are prescribed for many conditions other
than depression including headaches, hot flashes, and chronic pain. The total
retail sales figure is unlikely to reflect either drug company profits or the
amount of depression being treated.
A little arithmetic is always instructive. If we assume that
a physician prescribes a generic antidepressant for a patient that costs four
dollars per month that translates to a total cost of $48 per year. The $10 billion/year
figure quoted here would represent 208 million prescriptions or 66% of the entire population of the U.S. taking antidepressants 12 months out of the year. Even if we take $2 billion out of the $10
billion figure for Cymbalta and Vibryd, that results in 53% of the
population taking antidepressants 12 months out of the year. Those figures are
5-8 times higher than any actual estimation of antidepressant use. The $10 billion dollar figure is certainly
eye-opening but there is plenty of evidence that it is not remotely accurate
and will not have the purported impact on the pharmaceutical industry.
"About 80% of the
prescriptions for antidepressants are written by primary-care physicians and
others, not psychiatrists, a fact that makes the APA handbook particularly
important. Faced with a patient complaining of depression-like symptoms, a
general practitioner may be likely to rely on the Association's handbook for
advice.”
This statement reveals the authors lack of knowledge about
the practice of medicine and about the DSM that he is criticizing. The DSM is
strictly a diagnostic manual and it contains no treatment recommendations.
Primary care physicians are not avid readers of the DSM and that has probably
led to the practice of using a DSM-based checklist – the PHQ-9. This practice has not been promoted by the
APA or the pharmaceutical industry (although the PHQ-9 is copyrighted by Pfizer
pharmaceuticals). Using a checklist to
make a rapid diagnoses (in minutes) and rapidly treat large numbers of patients
is promoted by managed care organizations and HMOs. That is probably the single
greatest factor contributing to antidepressant prescriptions but it is ignored
by the author - probably because it challenges his contention that this is all driven
by conflict of interest in psychiatry rather than the business world. It is cheaper for HMOs to treat depression with medications rather than detailed psychiatric assessments and psychotherapy.
"The Association
itself runs on a budget of about 50 million a year, and for years industry
funding has been critical to its operations. Today, about 14% of the
Association's budget comes from pharmaceutical companies, mainly in the form of
advertising at annual meetings and publications."
The author does a good job of providing no context here. Is
the APA any different from other medical specialty organizations? Does
advertising create a conflict of interest? Is any other print media outlet held to that
standard? There is information available in those areas. An Institute of Medicine report focused on
conflict of interest showed that the APA's revenue from the pharmaceutical
industry was in the middle of the pack with regard to medical specialty
societies. As an example, the year that report was done the APA reported that medical companies supplied 28% of their annual income. The American Academy of
Family Physicians reported that 42% of their annual income was from pharmaceutical companies (p 220). That same report
(Recommendation 6.1) noted that increasing work for the pharmaceutical industry
correlated with a 7% reduction in real physician wages and recommended that
there was nothing wrong with “consulting arrangements based on written
contracts for expert services to be paid for at fair market value”. Depending on the expert involved, restricting
the amount to $10,000 per year could practically mean anywhere from 2 to 10
presentations per year or about 2 1/2 weeks of contract work.
“Other members of the
committee have numerous ties to drug companies, too, and not simply conducting
research, according to disclosures from last year. One was holding stock in
Glaxo Smith Kline, one was a consultant to Servier and another consultant to
Pfizer; one had a grant from AstraZeneca
and another a grant from Pfizer and AstraZeneca.”
This is a paragraph from a poorly written section
illustrating ties between the 11 member Mood Disorders Work Group set up to
draft the guidelines on major depression. There is some explanation of the
selection criteria and conflict of interest criteria. It discusses conflictof interest criteria that the APA designed and made explicit in response to
this article. It provides no context
other than an off hand remark by the chairman that he probably regrets making.
The article provides no reasonable context for expected reimbursement for
experts as consultants to industries or the fact that this is a common practice
in many academic departments on any major university campus. In some of those
industries, the professional organizations actually make an effort to make sure
that businesses are well represented in any process that involves making
standards.
"The current handbook-the revised version will be
published in the Spring-recommended against diagnosing major depression in the
bereaved when the symptoms are milder and of less than two months duration.
This is known as the "bereavement exclusion". (If the signs of depression are severe-the
patient has thoughts of suicide, for example-major depression is supposed to be
diagnosed)….. The new handbook removes the bereavement exclusion."
There is really nothing new and nothing drastic as
anticipated with removing the "bereavement exclusion". To provide a
clear example I will quote a text copyrighted in 1982:
"There are many
publications that deal with treating psychiatric patients who report recent and
remote bereavement. It is possible to find a real or imagined loss in every
patient's past. However, for the most part, because there is little evidence
from reviewing normal bereavement that there is a strong correlation between
bereavement and first entry into psychiatric care, those bereaved who are seen by
psychiatrists should be treated for their primary symptoms. This is not to say
that the death should not be discussed, but because these people represent a
very small subset of all recently bereaved, they should be treated like other
patients with similar symptoms but no precipitating cause. A physician seeing
a recently bereaved with newly discovered hypertension might delay treatment
one or two visits to confirm its continued existence, but treat it if it persists.
So the psychiatrist should treat the patient with affective symptoms with
somatic therapy but only if the symptoms are major and persist unduly. A
careful history of past and present drug and alcohol intake is indicated. Then,
the safest and most appropriate drugs to use are the antidepressants.
Electroconvulsive therapy is indicated in the suicidal depressed."
(Paykel p413-414).
Any psychiatrist worth his or her salt knows the difference
between grief and depression and they should know the literature on treating
grief, the natural history of grief, and the research on proven non-medical
treatment of grief including Interpersonal Psychotherapy (IPT) and grief counseling. When you are seeing a
psychiatrist, you are seeing an expert who should know the literature on grief, depression, and the differential diagnosis of depression. Nothing in this article indicates that. In
fact, quotes are provided to suggest that the APA and psychiatry in general has an interest in redefining “the range of acceptable emotion” rather than using
clinical research done by psychiatrists to limit suffering and prevent suicide.
I think the reality here indicates that there is no scandal. The importance of the DSM-5, the appearance of conflict of interest, and the potential windfall for the pharmaceutical industry appear to be seriously overestimated. Organized psychiatry is certainly not responsible for what happens in primary care clinics under the direct guidance of business organizations. There is a responsibility to establish professional standards for patients referred to psychiatrists for the assessment and treatment of complicated depressions that may occur during bereavement. The suggestion that medications may be useful in some of these situations and the importance of treating depression in bereavement has been around for at least 30 years.
I think the reality here indicates that there is no scandal. The importance of the DSM-5, the appearance of conflict of interest, and the potential windfall for the pharmaceutical industry appear to be seriously overestimated. Organized psychiatry is certainly not responsible for what happens in primary care clinics under the direct guidance of business organizations. There is a responsibility to establish professional standards for patients referred to psychiatrists for the assessment and treatment of complicated depressions that may occur during bereavement. The suggestion that medications may be useful in some of these situations and the importance of treating depression in bereavement has been around for at least 30 years.
George Dawson, MD, DFAPA
Peter Whoriskey. Antidepressants
to treat grief? Psychiatry panelists with ties to drug industry say yes. The Washington Post, December 26, 2012.
Clayton PJ. Bereavement in Handbook of Affective of Disorders. Eugene S. Paykel (ed). The Guilford Press.
New York. 1982 pages 413-414.
APA Reiterates Stringent Rules on Accepting Pharma Support. Psychiatric
News. Monday December 31,2012.
Institute of Medicine (US) Committee on Conflict of Interest in Medical Research, Education, and Practice; Lo B, Field MJ, editors. Conflict of Interest in Medical Research, Education, and Practice. Washington (DC): National Academies Press (US); 2009. Available from: http://www.ncbi.nlm.nih.gov/books/NBK22942/
Institute of Medicine (US) Committee on Conflict of Interest in Medical Research, Education, and Practice; Lo B, Field MJ, editors. Conflict of Interest in Medical Research, Education, and Practice. Washington (DC): National Academies Press (US); 2009. Available from: http://www.ncbi.nlm.nih.gov/books/NBK22942/
Tuesday, October 23, 2012
Conflict of interest and psychiatry - what's missing?
A new article looking at conflict of interest in psychiatry
was presented on another blog to suggest that new rules are required to improve
transparency. The article takes a look at six cases and the process used by
Sen. Charles Grassley to publicize these cases. The article suggests
that the reason for publicizing these cases was in order to support Grassley
legislation (Physician Payment Sunshine
Provision). According to the article it was attached to the Patient Protection and Affordable Care Act
and was never voted on alone.
These cases were repeatedly publicized in the popular media and some of the problems with these cases and Grassley's analysis were never adequately discussed. The clearest example is the case of Alan F. Schatzberg, MD of Stanford University. He was the chairman of the Department of psychiatry and when Grassley investigated the matter at the level of Stanford University and several pharmaceutical companies. You can read the exact details in this paper but the bottom line is that Stanford University has always maintained that it handled potential conflicts of interest in an appropriate manner consistent with their policies. They actually published a statement on their web page at the time. He remained the department head and although he was apparently temporarily removed as the principal investigator on a federal grant but he was later reinstated. The authors of the article in this case suggest that exposing the conflict of interest had negligible effect on the outcomes in this case, but the fact is the case was handled according to university policy.
Chimonas S, Stahl F, Rothman DJ. Exposing conflict of interest in psychiatry:
Does transparency matter? Int J Law Psychiatry.
2012 Oct 1. pii: S0160-2527(12)00072-6. doi: 10.1016/j.ijlp.2012.09.009.
These cases were repeatedly publicized in the popular media and some of the problems with these cases and Grassley's analysis were never adequately discussed. The clearest example is the case of Alan F. Schatzberg, MD of Stanford University. He was the chairman of the Department of psychiatry and when Grassley investigated the matter at the level of Stanford University and several pharmaceutical companies. You can read the exact details in this paper but the bottom line is that Stanford University has always maintained that it handled potential conflicts of interest in an appropriate manner consistent with their policies. They actually published a statement on their web page at the time. He remained the department head and although he was apparently temporarily removed as the principal investigator on a federal grant but he was later reinstated. The authors of the article in this case suggest that exposing the conflict of interest had negligible effect on the outcomes in this case, but the fact is the case was handled according to university policy.
There are really two key elements in this paper that are
critical. The first is why Grassley went after psychiatry in the first place.
The article suggests this occurs because his aide Paul Thacker "Combed the media for stories of influential
physicians with industry ties. He then requested the physicians conflict of
interest disclosures from their AMCs and compared them to payment schedules
obtained from companies." I had
always wondered why physicians from other specialties were never mentioned or
consultants from other departments. It is fairly well known that scientists and
engineers can make substantial incomes to supplement their university salaries
based on their expertise. So why was the "media combing" restricted to
psychiatry?
If I had to speculate, I would suggest that media bias
against psychiatry is a well known fact. It has actually been investigated and
the frequency of negative press that psychiatry receives relative to other
specialties is well known. (see paragraph 4) The popular press has an automatic media bias
against psychiatry and it should come as no surprise that prominent
psychiatrists are investigated and reported more frequently than other
specialists. This is why “combing the media” is really not a legitimate
research method. It should be fairly obvious that prominent university
affiliated physicians of all specialties have similar conflicts of interest and
that the business stake in other specialties is probably significantly higher.
The second element that should be obvious to anyone
skeptical of Congress is Grassley's quote in the article "The whole field
of medicine is connected by a tangled web of drug company money. For the sake
of transparency and accountability should the American public know who their
doctor is taking money from?" That sounds like there is an obvious answer in there
somewhere but the U.S. Congress is the best case in point that transparency is
essentially meaningless. There is probably no better example than Sen. Grassley
himself. You don't have to look too far
to find campaign donations that align with the votes and the Senator's denial (see paragraph 8) that there is any connection.
These simple facts are left out of the Journal article and
that represents a serious flaw to me. Is the U.S. Congress is a shining example of
disclosure becoming a license to do whatever you want to do? If that is the
case you really don't have the basis to suggest that
transparency will allow the "power of sunlight to disinfect". It
clearly does not have that effect in Congress. That is at the minimum an appearance of a conflict of interest on par with any scenario described in this article. When I point this out - the usual rebuttal is that doctors should have a higher standard when it comes to the appearance of conflict of interest. Is that really true? Should a doctor who already has a fiduciary responsibility to a patient and the patient's well being have a higher conflict of interest standard than one of the 100 most important law makers in the country?
The other issue here of course is that psychiatrists are
conveniently thrown under the bus. Despite the qualifier in this paper is that
"Nor did Grassley ever assert that psychiatry was more problematic than
other specialties." (p 5). You
really don't have to make an assertion when psychiatry is apparently the only
field you are investigating. That bias is totally consistent with one of the
themes of this blog.
When all else fails you can more easily scapegoat psychiatrists. So why look for anybody else?
George Dawson, MD. DFAPA
Does transparency matter? Int J Law Psychiatry.
2012 Oct 1. pii: S0160-2527(12)00072-6. doi: 10.1016/j.ijlp.2012.09.009.
[Epub ahead of print] PubMed PMID: 23036364.
Subscribe to:
Posts (Atom)