I was reading a copy of JAMA the other day and a story written by a transplant surgeon Jeremy M. Blumberg, MD. It was an excellent description of surgical training to the point of autonomy and then the nagging uncertainty of whether the surgery you have trained for years to do will go well. Will you avoid mistakes? He describes his first transplant as an attending:
"This operating room was new to me; the nurses were friendly but foreign. The instruments were familiar, but somehow felt different - was there just a barely palpable increase in tension in the muscles of my hand causing this effect? The patient's blood vessels were hard, thickened from years of dialysis and diabetes. She bled more than usual when we reperfused the kidney. It felt as if every last molecule of epinephrine had rushed out of my glands and nerves, squeezing my blood vessels and taunting my intestines to detonate...." (p. 1676)
I hear you brother. I thought that level of anxiety over the balance between doing the impossible and not doing harm might fade away over the years but it has not. In psychiatry a lot of it depends on the level of complexity that your patients have. It can be an acute situation but more often than not - it is a problem throughout the day that you take home with you. Additional medical conditions, non psychiatric medications, polypharmacy, and difficult to treat disorders all compound the problem. I have designed a hierarchy to illustrate what I mean. It turns out that when I think about it, the acute problems seen by psychiatrists are not at the top. The problems at the top are typically problems where there is no good guidance, where you are on your own, left with biologically determined probabilities and you need to come up with your best estimate of what will happen given current circumstances. The problems encompass both psychiatry and the medicine associated with psychiatry.
Let me provide an example of both. In the case of the psychiatric problem the usual scenario is a case of impaired judgment. Is the person at risk for death or self injury? Are they able to cooperate with the assessment and treatment plan. Do they seem changed to the point that you can no longer accept their responses as being accurate? Are you treating them for acute and chronic suicidal ideation and behavior? Any acute care psychiatrist ends up assessing thousands of the situations across the course of their career. It is often much more complex than an acute assessment. Many of these scenarios unfold in the context of ongoing psychotherapy and in order for the patient to be able to improve some risk is taken. In other cases there are calls to warn people and in extreme cases - calls to the police to check on a person who might be in trouble. I have not seen it studied but the stress of these situations for the psychiatrist involved is well known. Overthinking the situation in order to avoid the unexpected call that one of your patients has suicided or killed someone is common. In my conversations with medical students over the years, one of the main deterrents to psychiatric residency is the worry about suicide prediction.
The medical situations are as complex and they frequently have no clear solution. A common scenario is that the person has a severe mental illness and they develop a problem that leads to to rethinking the medication they are taking. A common scenario is a person on maintenance therapy who suddenly develops a renal or hepatic problem necessitating a change in therapy. The best example is bipolar disorder and lithium therapy. Lithium remains the drug of choice for many people with bipolar disorder and it can be highly effective. When I first started to practice it was common to see people who had repeated institutionalizations for bipolar disorder suddenly stabilized on lithium. Their functional capacity was restored and they were able to return to work and establish families. In those early days, the issue of lithium nephrotoxicity was not clearly observed. There was a major study of people on lithium maintenance for decades that showed no difference in renal function. In the last 15-20 years most nephrologists agree that lithium can lead to renal insufficiency and failure in a minority of patients on lithium therapy. In the case of a person that lithium has been working well for 30 years, there is no guarantee that anything else will work as good. That translates to no hospitalizations in a long time to frequent hospitalizations every year. Monitoring that therapy and in some cases following the patient while they are in dialysis or after transplantation is on example of a situation that you can't leave at the office.
In many ways, the stress and anxiety in psychiatric practice is a measure of attempting to predict the unpredictable. Psychiatry has accurately said that psychiatrists can't predict future behavior or rare events to explain why all suicides and homicides cannot be prevented. But some sort of probability statement is inherent in all medical practice. I would estimate it still happens to me about every three weeks. Something isn't right and I don't have an exact answer. It becomes an obsession to an extent. Laying awake in bed. Getting up to do some additional research but realizing ahead of time that the yield is low. Realizing that no matter what decision you make - all of the outcomes are probably going to be suboptimal. You always get to the point where you can feel the adrenaline molecules rushing and your heart pounding. You know you are tense and starting to break into a light sweat. You readjust yourself in bed and realize your back and shoulders are as tight as a frozen hydraulic jack. You might actually check your pulse and blood pressure and find that they are elevated. It goes on like this until something happens and the intellectual crisis abates. Sometimes that takes a while - at one point months and a beta blocker to break up the stress induced tachycardia and hypertension.
No I don't have generalized anxiety disorder - I am a doctor trying to deal with the uncertainties of being human.
George Dawson, MD, DFAPA
Saturday, October 26, 2013
Tuesday, October 22, 2013
APA Continues to Hype Managed Care
This YouTube video is fresh off my Facebook feed this morning from the APA. It features American Psychiatric Association (APA) President Jeffrey Lieberman, MD discussing the advantages of a so-called collaborative care model that brings psychiatrists into primary care clinics. I have critiqued this approach in the past and will continue to do so because it is basically managed care taken to its logical conclusion. As opposed to Dr. Lieberman's conclusion, the logical conclusion here is to simply take psychiatrists out of the picture all together.
A prototypical example of what I am talking about is the Diamond Project in Minnesota. It is an initiative by a consortium of managed care companies to use on of these models to monitor and treat depression in primary care clinics in the state of Minnesota. In this model, patients are screened and monitored using the PHQ-9 a rating scale for depressive symptoms. Their progress is monitored by a care manager and if there is insufficient progress as evidence by those rating scales, a psychiatrist is consulted about medication doses and other potential interventions. The model is described in this Wall Street Journal article. As is very typical of articles praising this approach it talks about the "shortage" of psychiatrists and how it will require adjustments. In the article for example, the author points out that there would no longer be "one-to-one" relationships. There are two major problems with this approach that seem to never be not considered.
The first is the standard of care. There are numerous definitions but the one most physicians would accept is care within a certain community that is the agreed upon standard provided by the same physician peers. In this case care provided by all psychiatrists for a specific condition like depression. There are professional guidelines for the care of depression and in the case of primary care guidelines for care provided by both family physicians and internal medicine specialists. One of the tenants of this care is that physicians generally base treatment of an assessment that they have done and documented. The only exception to that is an acceptable surrogate like a colleague in the same group covering a physician's patients when they are not available. That colleague generally has access to the documented assessment and plan to base decisions on. This is the central feature of all treatment provided by physicians and is also the basis for continuity of care. As such it also forms the basis of disciplinary action by state medical boards and malpractice claims for misdiagnosis and maltreatment. An example of disciplinary action based on this standard of care is inappropriate prescribing with no documented assessment or plan - a fairly common practice in the 1980s.
In all of my professional life, the standard of care has been my first and foremost consideration. It is basically a statement of accountability to a specific patient and that is what physicians are trained to be. Curiously it is not explicit in ethics literature and difficult to find in many state statutes regulating medical practice. That may be due to the entry of managed care and the introduction of business ethics rather than medical ethics. It also may be due in part to an old community mental health center practice of hiring psychiatrists essentially to refill prescriptions rather than assess patients. This is addressed from a malpractice perspective by Gutheil and Appelbaum in their discussion of malpractice considerations and how they changed with the advent of managed care:
"Managed care is one omnipresent constraint. Patients and clinicians must work together to fashion an appropriate treatment plan to take into account available resources and given the contingencies faced by the patient. If that plan-properly implemented-fails to prevent harm to the patient, the clinician should not face liability as a result." (p 164).
They go on to explain how ERISA - the Employee Retirement Income Security Act of 1974 indemnifies managed care companies and their reviewers from the same liability that individual physicians have. They cannot be sued for negligence and the resulting harm. So managed care can take risks without concern about penalties as opposed to physicians who are obliged to discuss risks with the patient. Managed care organizations can also implement broad programs like depression screening and treatment without a physician assessment and consider that their standard of care.
The second problem with the so-called collaborative care approach is that there is no evidence that it is effective on a large scale. I pointed out this criticism by a group of co-authors including one of the most frequently cited epidemiologists in the medical literature. That group has the common concern that a rating scale is a substitute for an actual diagnosis and everything that involves and given the recent FDA warning on citalopram.
Both of these concerns bring up an old word that nobody uses anymore - quality. It is customary today to use a blizzard of euphemisms instead. Words like "behavioral health", "managed care", accountable care organizations", "evidence-based", "cost-effective" and now "collaborative care". According to Orwell, the success of such political jargon and euphemism requires
"an uncritical or even unthinking audience. A 'reduced state of consciousness' as he put it, was 'favorable to political conformity'." (3 p. 124)
Dr. Lieberman uses a lot of that language in his video. The critics of psychiatry in the business community do the same. There appears to be a widespread uncritical acceptance of these euphemisms by politicians, businesses and even professional organizations.
An actual individualized psychiatric diagnosis and quality psychiatric care gets lost in that translation.
George Dawson, MD, DFAPA
1. Beck M. Getting mental health care at the doctor's office. Wall Street Journal September 24, 2013.
2. Gutheil TG, Appelbaum PS. Clinical Handbook Of Psychiatry And The Law. 3rd edition. Philadelphia: Lippincott Williams & Wilkens. 2000, p 164.
3. Nunberg G. Going Nucular: language, politics, and culture in confrontational times. Cambridge: Perseus Books Group, MA 2004.
4. American Psychiatric Association Principles of Medical Ethics with Annotations Espcially Applicable to Psychiatry. 2009 version.
A prototypical example of what I am talking about is the Diamond Project in Minnesota. It is an initiative by a consortium of managed care companies to use on of these models to monitor and treat depression in primary care clinics in the state of Minnesota. In this model, patients are screened and monitored using the PHQ-9 a rating scale for depressive symptoms. Their progress is monitored by a care manager and if there is insufficient progress as evidence by those rating scales, a psychiatrist is consulted about medication doses and other potential interventions. The model is described in this Wall Street Journal article. As is very typical of articles praising this approach it talks about the "shortage" of psychiatrists and how it will require adjustments. In the article for example, the author points out that there would no longer be "one-to-one" relationships. There are two major problems with this approach that seem to never be not considered.
The first is the standard of care. There are numerous definitions but the one most physicians would accept is care within a certain community that is the agreed upon standard provided by the same physician peers. In this case care provided by all psychiatrists for a specific condition like depression. There are professional guidelines for the care of depression and in the case of primary care guidelines for care provided by both family physicians and internal medicine specialists. One of the tenants of this care is that physicians generally base treatment of an assessment that they have done and documented. The only exception to that is an acceptable surrogate like a colleague in the same group covering a physician's patients when they are not available. That colleague generally has access to the documented assessment and plan to base decisions on. This is the central feature of all treatment provided by physicians and is also the basis for continuity of care. As such it also forms the basis of disciplinary action by state medical boards and malpractice claims for misdiagnosis and maltreatment. An example of disciplinary action based on this standard of care is inappropriate prescribing with no documented assessment or plan - a fairly common practice in the 1980s.
In all of my professional life, the standard of care has been my first and foremost consideration. It is basically a statement of accountability to a specific patient and that is what physicians are trained to be. Curiously it is not explicit in ethics literature and difficult to find in many state statutes regulating medical practice. That may be due to the entry of managed care and the introduction of business ethics rather than medical ethics. It also may be due in part to an old community mental health center practice of hiring psychiatrists essentially to refill prescriptions rather than assess patients. This is addressed from a malpractice perspective by Gutheil and Appelbaum in their discussion of malpractice considerations and how they changed with the advent of managed care:
"Managed care is one omnipresent constraint. Patients and clinicians must work together to fashion an appropriate treatment plan to take into account available resources and given the contingencies faced by the patient. If that plan-properly implemented-fails to prevent harm to the patient, the clinician should not face liability as a result." (p 164).
They go on to explain how ERISA - the Employee Retirement Income Security Act of 1974 indemnifies managed care companies and their reviewers from the same liability that individual physicians have. They cannot be sued for negligence and the resulting harm. So managed care can take risks without concern about penalties as opposed to physicians who are obliged to discuss risks with the patient. Managed care organizations can also implement broad programs like depression screening and treatment without a physician assessment and consider that their standard of care.
The second problem with the so-called collaborative care approach is that there is no evidence that it is effective on a large scale. I pointed out this criticism by a group of co-authors including one of the most frequently cited epidemiologists in the medical literature. That group has the common concern that a rating scale is a substitute for an actual diagnosis and everything that involves and given the recent FDA warning on citalopram.
Both of these concerns bring up an old word that nobody uses anymore - quality. It is customary today to use a blizzard of euphemisms instead. Words like "behavioral health", "managed care", accountable care organizations", "evidence-based", "cost-effective" and now "collaborative care". According to Orwell, the success of such political jargon and euphemism requires
"an uncritical or even unthinking audience. A 'reduced state of consciousness' as he put it, was 'favorable to political conformity'." (3 p. 124)
Dr. Lieberman uses a lot of that language in his video. The critics of psychiatry in the business community do the same. There appears to be a widespread uncritical acceptance of these euphemisms by politicians, businesses and even professional organizations.
An actual individualized psychiatric diagnosis and quality psychiatric care gets lost in that translation.
George Dawson, MD, DFAPA
1. Beck M. Getting mental health care at the doctor's office. Wall Street Journal September 24, 2013.
2. Gutheil TG, Appelbaum PS. Clinical Handbook Of Psychiatry And The Law. 3rd edition. Philadelphia: Lippincott Williams & Wilkens. 2000, p 164.
3. Nunberg G. Going Nucular: language, politics, and culture in confrontational times. Cambridge: Perseus Books Group, MA 2004.
4. American Psychiatric Association Principles of Medical Ethics with Annotations Espcially Applicable to Psychiatry. 2009 version.
Sunday, October 20, 2013
SNL Keeps the Stigma Going
I suppose I was one of millions of disappointed viewers who tuned in to Saturday Night Live last night. One of the skits was to show the first used car commercial. The commercial uses the familiar "crazy" motif, implying that the business uses an irrational pricing strategy that favors the customer. Practically every television market has a business that uses this approach for selling cars, appliances, stereos, you name it. I suppose that some comedians would suggest that this is commentary on these commercials as a rationale for the video. In the same show there was a skit about a drunk uncle. At one point the drunk uncle introduces meth nephew - portrayed by an actor for the AMC series Breaking Bad. I can recall the comedic placement of an alcoholic dating back to The Andy Griffith Show's Otis.
Associating comedy with mental illness is stigmatizing. That is not an original thought and I am sure that some people have written about it before. I am sure there is a thesis somewhere submitted for degree requirements that looks at the rationale and the pros and the cons. For me the straightforward analysis is that it is a reflection of the disproportionate noise in the media about psychiatry and mental health. That is closely followed by the fact that there are no similar comedic approaches to other diseases. Where are the skits about an uncle with cirrhosis, chronic pancreatitis or cancer? Or the uncle in prison for vehicular homicide while intoxicated?
I also can't help but notice if you were not laughing at the Tina Fey character in the commercial what were you thinking? I was thinking about a situation where a family might notice a personality change or a change in thinking like the one described in this skit and what they would do about it. There are no clearly defined public health approaches to these problems. People get concerned, they get very uneasy, they don't know what to do about it, and complications happen. They may actually bring their relative down to the local Emergency Department only to find that they are declared "not imminently dangerous" and discharged with a number to call for an outpatient appointment. If their family member is in need of medical detoxification from alcoholism, they may be discharged with a bottle of lorazepam and instructed on how to detox them at home. I was thinking about the millions of Americans out there who have had this happen, have inadequate treatment, and never recover. Their role in the family is permanently altered or disrupted.
I was thinking about the legal approach to some of these problems and the issue of criminal responsibility. That dovetails with the lack of a public health approach because one of the possible complications is that a crime gets committed during an episode of mental illness. Of course it is a crime based on the assumption that the person is able to appreciate what they are doing and that it is unlawful. In the majority of cases it is not likely that a severe crime will be understood that way and the defendant will typically get psychiatric treatment in prison or a county jail. The civil legal approach is as problematic. An actual or practical "imminent dangerousness" standard for treatment leaves huge numbers of people untreated and acutely mentally ill.
For all of these reasons, these skits were not funny to me. I like Tina Fey and think that she is a comedic genius, but I didn't crack a smile. I think it will be a test of mental health advocacy groups everywhere to see what they say about this. Some have criticized SNL before but I have not seen anything about this skit so far. All of the discussions about the problems with the lack of adequate mental health treatment in this country and the associated public health disasters have no traction as long as we continue to think of mental illnesses and addictions as comedy.
George Dawson, MD, DFAPA
Associating comedy with mental illness is stigmatizing. That is not an original thought and I am sure that some people have written about it before. I am sure there is a thesis somewhere submitted for degree requirements that looks at the rationale and the pros and the cons. For me the straightforward analysis is that it is a reflection of the disproportionate noise in the media about psychiatry and mental health. That is closely followed by the fact that there are no similar comedic approaches to other diseases. Where are the skits about an uncle with cirrhosis, chronic pancreatitis or cancer? Or the uncle in prison for vehicular homicide while intoxicated?
I also can't help but notice if you were not laughing at the Tina Fey character in the commercial what were you thinking? I was thinking about a situation where a family might notice a personality change or a change in thinking like the one described in this skit and what they would do about it. There are no clearly defined public health approaches to these problems. People get concerned, they get very uneasy, they don't know what to do about it, and complications happen. They may actually bring their relative down to the local Emergency Department only to find that they are declared "not imminently dangerous" and discharged with a number to call for an outpatient appointment. If their family member is in need of medical detoxification from alcoholism, they may be discharged with a bottle of lorazepam and instructed on how to detox them at home. I was thinking about the millions of Americans out there who have had this happen, have inadequate treatment, and never recover. Their role in the family is permanently altered or disrupted.
I was thinking about the legal approach to some of these problems and the issue of criminal responsibility. That dovetails with the lack of a public health approach because one of the possible complications is that a crime gets committed during an episode of mental illness. Of course it is a crime based on the assumption that the person is able to appreciate what they are doing and that it is unlawful. In the majority of cases it is not likely that a severe crime will be understood that way and the defendant will typically get psychiatric treatment in prison or a county jail. The civil legal approach is as problematic. An actual or practical "imminent dangerousness" standard for treatment leaves huge numbers of people untreated and acutely mentally ill.
For all of these reasons, these skits were not funny to me. I like Tina Fey and think that she is a comedic genius, but I didn't crack a smile. I think it will be a test of mental health advocacy groups everywhere to see what they say about this. Some have criticized SNL before but I have not seen anything about this skit so far. All of the discussions about the problems with the lack of adequate mental health treatment in this country and the associated public health disasters have no traction as long as we continue to think of mental illnesses and addictions as comedy.
George Dawson, MD, DFAPA
Sunday, October 13, 2013
UW Update - the Rest of the Story
I am back at my usual computer tonight and feeling much better after attending the UW Psychiatric Update. It was well attended and I estimate there were about 400 people there - mostly psychiatrists. The conference brought in several people who were instrumental in the DSM-5 to talk about the thinking and research that went into it. The resulting story is one that you will never hear in the press or other media. The story is based on science as opposed to the irrational criticisms in the media and that science is written about and discussed by brilliant people. I will try to post a few examples, and wish that it had been presented to the public. The discussion produced for public consumption was not close to reality and it was a further example of how stigmatization of the profession prevents relevant information from reaching the public. It seems that the most we can hope for is an actual expert being placed in a staged debate or responding to some off-the-wall criticism - hoping to interject a few valid points. That is a recipe for selling the sensational and leaving out the scientific and rational. Just how far off the media is on this story is a mark of how skewed that perspective is.
Let me start with the disclosures. There were 14 presenters and 10 of them had no potential conflicts of interest to report. That included one work group chair. One of the presenters suggested that the political backlash against psychiatrists affiliated with the industry and the DSM limit on the amount of money that could be earned from the industry limited access to some experts and probably limits drug development. His question to the audience was: "What if it means that 10 years from, all we have to prescribe is generic paroxetine and generic citalopram? What if we have no better drugs?" It would be interesting to know who was specifically not able to participate in the process due to these restrictions. There were primarily 2 presenters with extensive industry support primarily in their role as consultants to the industry. One of them joked about his level of involvement: "Based on my disclosures you should probably not believe a thing that I say." He went on to give an excellent presentation replete with references to peer reviewed research.

Before I go on to talk about specific speakers I want to address another frequent illusion about psychiatrists and that is that they are primarily medication focused and have minimal interest in other treatments. That is convenient rhetoric if you are trying to build a case that psychiatrists are all dupes for the pharmaceutical industry and that drives most of their waking decisions. During the presentation of the pharmacological treatment of obsessive compulsive disorder, the presenter clearly stated: "It could probably be said that we are still waiting for an effective medication for obsessive compulsive disorder." Certainly, the section on autism spectrum disorder presented the current AACAP practice parameters and the fact that there is no medication that treats the core features but some that that have a "mild to modest" effect on some features or comorbidities. Three of the four breakout sessions in the early afternoon of day 1 were psychotherapy focused. I attended Mindfulness Based Cognitive Therapy and Recurrent Major Depression with about 200 other participants. We were guided through two interventions that could be used in follow up individual sessions as well as groups. The efficacy of preventing recurrent major depression with this modality alone was discussed. The Psychotherapeutic Treatment of Insomnia and Pediatric Post Traumatic Stress Disorder were discussed in parallel sessions. In the PTSD lecture, it was pointed out that there is no FDA approved medication for the treatment of this disorder and that the gold standard of treatment is Trauma Focused Cognitive Behavior Therapy (CBT). That's right a psychiatric conference where the treatment of choice is psychotherapy and not medications.
What about he individual presentations on the thinking behind the DSM? I was thoroughly impressed by Katharine A. Phillips, MD Chair of the DSM-5 Anxiety, Obsessive-Compulsive Spectrum, Post Traumatic Stress Disorder Work Group. Reviewing the structure of the DSM-5 as opposed to the DSM-IV shows that all of these disorder previously considered anxiety disorders are now all broken out into their own categories. She discussed the rationale for that change as well as the parameters that were considered in grouping disorders in chapters - clearly an advance over DSM-IV. She talked about the two new disorders Hoarding and Excoriation (Skin Picking) Disorder and why they were OCD spectrum disorders. She talked about insight and how it varies in both OCD and Body Dysmorphic Disorder (BDD). She discussed the new OCD Tic-Related Specifier and its importance. Most importantly she discussed how the decisions of the Workgroup will improve patient care. The most obvious example, is the case of BDD where both the delusional and non-delusional types respond to SSRIs and those are the drugs of choice and not antipsychotics. By grouping BDD in with Obsessive Compulsive Disorder and Related Disorders recognition and appropriate treatment will probably be enhanced. Dr. Phillips is the researcher who initially discovered the treatment response of BDD to SSRIs. She is also a rare lecturer who does not pay much attention to the PowerPoint slides but speaks extemporaneously and authoritatively on the subject in a parallel manner.
Susan E. Swedo, MD was the Chair DSM-5 Neurodevelopmental Disorder Work Group. She talked in detail about the elimination of the Pervasive Developmental Disorders diagnosis and how the Autism Spectrum Disorder diagnosis reflected current terminology in the field over the past ten years and how it basically eliminated 5 DSM-IV diagnoses (Autistic Disorder, Asperger Disorder, Pervasive Developmental Disorder, Childhood Disintegrative Disorder, and Rett Disorder). She pointed out that the Workgroup could only locate 24 cases of anyone who had ever been diagnosed with Childhood Disintegrative Disorder and that the CDC's epidemic of Autism was probably related to diagnostic confusion and overlap between PDD-NOS and Attention Deficit Hyperactivity Disorder. She gave a detailed response to the "publicized concerns about DSM-5" including decreased sensitivity to improve specificity, the loss of the uniqueness of the Asperger Diagnosis, and the fact that pre/post research in this area won't be comparable. She showed a detailed graphic and comparison of DSM-IV and DSM-5 criteria to show why that is not accurate.
I came away from this conference refreshed and more confident than ever about the reason for writing this blog. I had just seen some of the top scientists and minds in the field and why the DSM was really changed - not what you read in the New York Times. If you are a psychiatrist - there were plenty of reasons for a DSM-5 and if you read this far, it is only the tip of the iceberg.
George Dawson, MD, DFAPA
Let me start with the disclosures. There were 14 presenters and 10 of them had no potential conflicts of interest to report. That included one work group chair. One of the presenters suggested that the political backlash against psychiatrists affiliated with the industry and the DSM limit on the amount of money that could be earned from the industry limited access to some experts and probably limits drug development. His question to the audience was: "What if it means that 10 years from, all we have to prescribe is generic paroxetine and generic citalopram? What if we have no better drugs?" It would be interesting to know who was specifically not able to participate in the process due to these restrictions. There were primarily 2 presenters with extensive industry support primarily in their role as consultants to the industry. One of them joked about his level of involvement: "Based on my disclosures you should probably not believe a thing that I say." He went on to give an excellent presentation replete with references to peer reviewed research.

Before I go on to talk about specific speakers I want to address another frequent illusion about psychiatrists and that is that they are primarily medication focused and have minimal interest in other treatments. That is convenient rhetoric if you are trying to build a case that psychiatrists are all dupes for the pharmaceutical industry and that drives most of their waking decisions. During the presentation of the pharmacological treatment of obsessive compulsive disorder, the presenter clearly stated: "It could probably be said that we are still waiting for an effective medication for obsessive compulsive disorder." Certainly, the section on autism spectrum disorder presented the current AACAP practice parameters and the fact that there is no medication that treats the core features but some that that have a "mild to modest" effect on some features or comorbidities. Three of the four breakout sessions in the early afternoon of day 1 were psychotherapy focused. I attended Mindfulness Based Cognitive Therapy and Recurrent Major Depression with about 200 other participants. We were guided through two interventions that could be used in follow up individual sessions as well as groups. The efficacy of preventing recurrent major depression with this modality alone was discussed. The Psychotherapeutic Treatment of Insomnia and Pediatric Post Traumatic Stress Disorder were discussed in parallel sessions. In the PTSD lecture, it was pointed out that there is no FDA approved medication for the treatment of this disorder and that the gold standard of treatment is Trauma Focused Cognitive Behavior Therapy (CBT). That's right a psychiatric conference where the treatment of choice is psychotherapy and not medications.
What about he individual presentations on the thinking behind the DSM? I was thoroughly impressed by Katharine A. Phillips, MD Chair of the DSM-5 Anxiety, Obsessive-Compulsive Spectrum, Post Traumatic Stress Disorder Work Group. Reviewing the structure of the DSM-5 as opposed to the DSM-IV shows that all of these disorder previously considered anxiety disorders are now all broken out into their own categories. She discussed the rationale for that change as well as the parameters that were considered in grouping disorders in chapters - clearly an advance over DSM-IV. She talked about the two new disorders Hoarding and Excoriation (Skin Picking) Disorder and why they were OCD spectrum disorders. She talked about insight and how it varies in both OCD and Body Dysmorphic Disorder (BDD). She discussed the new OCD Tic-Related Specifier and its importance. Most importantly she discussed how the decisions of the Workgroup will improve patient care. The most obvious example, is the case of BDD where both the delusional and non-delusional types respond to SSRIs and those are the drugs of choice and not antipsychotics. By grouping BDD in with Obsessive Compulsive Disorder and Related Disorders recognition and appropriate treatment will probably be enhanced. Dr. Phillips is the researcher who initially discovered the treatment response of BDD to SSRIs. She is also a rare lecturer who does not pay much attention to the PowerPoint slides but speaks extemporaneously and authoritatively on the subject in a parallel manner.
Susan E. Swedo, MD was the Chair DSM-5 Neurodevelopmental Disorder Work Group. She talked in detail about the elimination of the Pervasive Developmental Disorders diagnosis and how the Autism Spectrum Disorder diagnosis reflected current terminology in the field over the past ten years and how it basically eliminated 5 DSM-IV diagnoses (Autistic Disorder, Asperger Disorder, Pervasive Developmental Disorder, Childhood Disintegrative Disorder, and Rett Disorder). She pointed out that the Workgroup could only locate 24 cases of anyone who had ever been diagnosed with Childhood Disintegrative Disorder and that the CDC's epidemic of Autism was probably related to diagnostic confusion and overlap between PDD-NOS and Attention Deficit Hyperactivity Disorder. She gave a detailed response to the "publicized concerns about DSM-5" including decreased sensitivity to improve specificity, the loss of the uniqueness of the Asperger Diagnosis, and the fact that pre/post research in this area won't be comparable. She showed a detailed graphic and comparison of DSM-IV and DSM-5 criteria to show why that is not accurate.
I came away from this conference refreshed and more confident than ever about the reason for writing this blog. I had just seen some of the top scientists and minds in the field and why the DSM was really changed - not what you read in the New York Times. If you are a psychiatrist - there were plenty of reasons for a DSM-5 and if you read this far, it is only the tip of the iceberg.
George Dawson, MD, DFAPA
Saturday, October 12, 2013
DSM 5 Total Diagnoses Revealed
As any reader of this blog can recall one of my foci is to expose the anti DSM 5 rhetoric for what is was. One the the main points by DSM detractors was diagnostic proliferation or more total diagnoses. This implies more diagnoses, more prescriptions, and more money for psychiatrists and pharmaceutical companies. Another spin was that it was the intent of organized psychiatry to "pathologize" the population. I put up a table on this issue in a previous post and at that time did not have the final number of diagnoses. As of today I have the final number and it is 157. According to the presenter that means that a total of 15 diagnoses were eliminated from DSM-IV to DSM 5. The total diagnoses in DSM 5 did not increase as the detractors predicted - they decreased by 15.
I was at a conference today put on by the University of Wisconsin Department of Psychiatry entitled Annual Update and Advances In Psychiatry. The Introduction by Art Walaszek, MD acknowledged that this was the first in a series that replaces a long tradition of courses run by John H. Greist, MD and James W. Jefferson, MD: "Jeff Jefferson and John Greist ran this conference for 31 years." That is an amazing track record and record of achievement and a contribution to psychiatry in the Midwest. I don't know of many psychiatrists who were not aware of this conference with the alliterative titles like: "Quaffing Quanta of Quality from Quick Witted Quinessentialists" or the Door County Course they regularly taught. They have been a model of scholarship and professionalism and continue to be.
The first speaker today was Alan Schatzberg, MD. He posted the information about the total diagnostic categories in DSM 5 an other important changes and how they occurred. Per my previous post about the DSM 5 lectures by Jon Grant, MD the DSM 5 effort was outlined in addition to some critical information on how stigma affects psychiatric diagnosis. For example, when the DSM 5 work group wanted to add mild neurocognitive disorder a well known historian of psychiatry came out and said it would add countless people who had normal memory impairment associated with aging. When neurologists added mild cognitive disorder to their diagnostic nomenclature (an equivalent diagnosis) no such claims were made about neurologists. In terms of the effort, Dr. Schatzberg pointed out that there were 13 conferences from 2003-2008 that produced 10 monographs and over 200 journal articles.
Dr. Schatzberg and his colleagues presented a ton of information today on what really happened with DSM 5 development. I will try to summarize and post additional comments when I can post from a more user friendly computer. I wanted to keep the post more on the scientific and debunk another common refrain from the naysayers before the DSM 5 was printed. That involved the so called "bereavement exclusion" that basically says that a person cannot be diagnosed with major depression if they are seen during an episode of grief. One question that was never brought up in the popular press "Where did this convention came into the diagnostic criteria in the first place?" I quoted a text from about the same time (see third from last paragraph) that makes this convention seem even more arbitrary. It turns out the original bereavement exclusion began in DSM-III not from any research basis but from convention that was subjectively determined by the authors of DSM-III. Contrast that with the research done by Zisook, et al. You would think that some of the self proclaimed level headed skeptics out there would have referred to this critical paper on the issue rather than speculative attacks on the field. Incorporating these scientific findings was one of the reasons that the DSM was updated.
Stay tuned for more of the hard data and insider info on DSM 5.
George Dawson, MD, DFAPA
1: Zisook S, Corruble E, Duan N, Iglewicz A, Karam EG, Lanouette N, Lebowitz B, Pies R, Reynolds C, Seay K, Katherine Shear M, Simon N, Young IT. The bereavement exclusion and DSM-5. Depress Anxiety. 2012 May;29(5):425-43. doi: 10.1002/da.21927. Epub 2012 Apr 11. Review. Erratum in: Depress Anxiety. 2012 Jul;29(7):665. PubMed PMID: 22495967.
Supplementary 1: The DSM-5 Guidebook by Donald W. Black, MD and Jon E. Grant, MD came out in March 2014. Table 1. (p. xxiii) lists the total diagnoses is DSM-5 as 157 excluding "other specified and unspecified disorders".
I was at a conference today put on by the University of Wisconsin Department of Psychiatry entitled Annual Update and Advances In Psychiatry. The Introduction by Art Walaszek, MD acknowledged that this was the first in a series that replaces a long tradition of courses run by John H. Greist, MD and James W. Jefferson, MD: "Jeff Jefferson and John Greist ran this conference for 31 years." That is an amazing track record and record of achievement and a contribution to psychiatry in the Midwest. I don't know of many psychiatrists who were not aware of this conference with the alliterative titles like: "Quaffing Quanta of Quality from Quick Witted Quinessentialists" or the Door County Course they regularly taught. They have been a model of scholarship and professionalism and continue to be.
The first speaker today was Alan Schatzberg, MD. He posted the information about the total diagnostic categories in DSM 5 an other important changes and how they occurred. Per my previous post about the DSM 5 lectures by Jon Grant, MD the DSM 5 effort was outlined in addition to some critical information on how stigma affects psychiatric diagnosis. For example, when the DSM 5 work group wanted to add mild neurocognitive disorder a well known historian of psychiatry came out and said it would add countless people who had normal memory impairment associated with aging. When neurologists added mild cognitive disorder to their diagnostic nomenclature (an equivalent diagnosis) no such claims were made about neurologists. In terms of the effort, Dr. Schatzberg pointed out that there were 13 conferences from 2003-2008 that produced 10 monographs and over 200 journal articles.
Dr. Schatzberg and his colleagues presented a ton of information today on what really happened with DSM 5 development. I will try to summarize and post additional comments when I can post from a more user friendly computer. I wanted to keep the post more on the scientific and debunk another common refrain from the naysayers before the DSM 5 was printed. That involved the so called "bereavement exclusion" that basically says that a person cannot be diagnosed with major depression if they are seen during an episode of grief. One question that was never brought up in the popular press "Where did this convention came into the diagnostic criteria in the first place?" I quoted a text from about the same time (see third from last paragraph) that makes this convention seem even more arbitrary. It turns out the original bereavement exclusion began in DSM-III not from any research basis but from convention that was subjectively determined by the authors of DSM-III. Contrast that with the research done by Zisook, et al. You would think that some of the self proclaimed level headed skeptics out there would have referred to this critical paper on the issue rather than speculative attacks on the field. Incorporating these scientific findings was one of the reasons that the DSM was updated.
Stay tuned for more of the hard data and insider info on DSM 5.
George Dawson, MD, DFAPA
1: Zisook S, Corruble E, Duan N, Iglewicz A, Karam EG, Lanouette N, Lebowitz B, Pies R, Reynolds C, Seay K, Katherine Shear M, Simon N, Young IT. The bereavement exclusion and DSM-5. Depress Anxiety. 2012 May;29(5):425-43. doi: 10.1002/da.21927. Epub 2012 Apr 11. Review. Erratum in: Depress Anxiety. 2012 Jul;29(7):665. PubMed PMID: 22495967.
Supplementary 1: The DSM-5 Guidebook by Donald W. Black, MD and Jon E. Grant, MD came out in March 2014. Table 1. (p. xxiii) lists the total diagnoses is DSM-5 as 157 excluding "other specified and unspecified disorders".
Sunday, October 6, 2013
"Some Sort of Mental Health Issue"
I was getting ready for work yesterday morning and watching The Today Show in the background as usual. Suddenly there was the story of a young woman trying to ram the security barriers at the White House and then being pursued in a high speed chase down Pennsylvania Avenue. It eventually showed a direct confrontation with law enforcement and them opening fire on her through the window of her vehicle. There was an initial report saying that she had fired shots but she was unarmed. The police discovered her one year old daughter in the car and removed her. The acute reaction captured on film was surreal. There were descriptions of some of her recent behavior and thoughts. A police official commented that the security barriers "worked" as though this was an assault by a terrorist. A different official commented how her daughter was "rescued" by the police. People were talking as though this was an actual assault by a terrorist. The last person I heard was a politician who made the quote at the top of this post and finally suggested the real problem.
Confrontation between people with severe mental illnesses and law enforcement are very common. During my years of acute inpatient work I have talked with many people who have been injured in every imaginable way during these confrontations. In some cases they were themselves engaged in very dangerous and aggressive behavior as the direct result of a mood disorder or a psychosis. In other cases law enforcement just misinterpreted their behavior. That happened most commonly when the person refused to comply with what the officer wanted them to do. These confrontations are always high risk situations because most people in society know that it is in their best interest to be law abiding and comply with the police. The people who don't are criminals or people with impaired judgment due to mental illness or intoxication states. Even if the police can make that distinction rapidly that does not mean they can easily use a different approach to the person with mental illness. Police officers have been injured or killed in these situations.
There seems to be a great deal of misunderstanding and continued bias about how these situations can occur. It can happen as rapidly as waking up one morning finding out that your entire state of consciousness has changed. That gas company truck across the street is there to monitor you and direct microwaves at you. The phones and your computer are bugged. Going to work that morning you decide you need to take evasive action because it seems like you are being followed. Your anxiety levels build all day and that night at home you can't sleep. You decide you need to move the refrigerator in front of the door because you had the thought that it would be too easy for government agents to kick the door down and grab you. You do a Google search on microwaves and decide these people are trying to do a lot more than harass you - they are trying to kill you. You start to make plans on that basis.
That is how paranoid delusions evolve and how they change your behavior. You are no longer making rational assessments of the environment. Your brain has come up with a theory and you are now interpreting all of the environmental information according to that theory. When I approach the problem psychotherapeutically, I generally explain that delusional thoughts are very low probability explanations or interpretations of an event in the environment. I illustrate this by asking the question: "If we had 100 people in the room right now - how many of them would agree with what you just told me?" Many people know that hardly anyone would agree with them, but that doesn't stop them from continuing to misinterpret the data or trying to cast me with everyone else who either doesn't believe them or is just saying that they are "crazy".
Before I outline an approach to the problem of people experiencing episodes of psychosis or mania and running into problems with law enforcement consider what gets in the way of any of early intervention? Keeping with my cardiology comparison from a previous post - most people know that chest pain is a warning sign for a possible heart attack. With continued public health interventions most people know cardiac risk factors. Public health intervention has been so effective that the current campaign is focused on decreasing the denial in women and decreasing cardiac sudden death in women. Two generations of public health intervention are associated with a decreasing rate of cardiac mortality.
How does that compare with psychosis and mania? I have never seen a public service ad advising about the warning signs of psychosis or mania. There are countless euphemisms for acute changes in a persons mental status. The public treats it like a mystery. When a tragedy occurs there is often no explanation or an inadequate one like "some sort of mental illness." The cultural approach is an obstacle to a rational approach to helping affected individuals. Stigma is considered to be a factor, but it could as easily be an artifact of the process. What would be a better approach?
I have been advocating a public health approach to the problem for a long time now. At a political level there is a lot of confusion about whether this is a firearms issue. Firearms are just a subset of the problem. The overriding public health goal is to get people the help that they need as soon as possible. Our current system of care is set up to provide minimal care to people with severe mental illnesses. The level of care and condition of the facilities where the care occurs is widely known in communities and most people do not want to access these facilities for help. I hear a lot about the concern that someone is going to be stigmatized by treatment at a psychiatric facility. I think it is as likely that many facilities are substandard physical plants that are poorly managed. Based on the length of stay policies alone, nobody wants to bring their relative to a facility that has a reputation for discharging partially stabilized people back into the community. The long term goal needs to be improving the quality of psychiatric facilities in addition to changing the culture about severe mental illness.
I thought of a public service announcement that would potentially have the same advertising power as some of the more popular health spots like the "7 warning signs of cancer". I call it the 4 warning signs of severe mental illness. A concerted effort to focus on severe mental illnesses that can potentially lead to errors in judgment is a logical way to approach this problem. Based on my previous paragraph it takes a much more enlightened approach to treating the problem. Health care systems in general are not friendly to people with severe mental illnesses. There are no specialty centers designed to cater to their needs like the high margin businesses get. Many of these health care organizations sponsor walks for mental illness and other programs like National Depression Screening day. But none of them say - if you have these symptoms we want to see you and treat you in a hospitable environment.
That attitude has to change to prevent the loss of innocent lives as the direct result of severe mental illness.
George Dawson, MD, DFAPA
Confrontation between people with severe mental illnesses and law enforcement are very common. During my years of acute inpatient work I have talked with many people who have been injured in every imaginable way during these confrontations. In some cases they were themselves engaged in very dangerous and aggressive behavior as the direct result of a mood disorder or a psychosis. In other cases law enforcement just misinterpreted their behavior. That happened most commonly when the person refused to comply with what the officer wanted them to do. These confrontations are always high risk situations because most people in society know that it is in their best interest to be law abiding and comply with the police. The people who don't are criminals or people with impaired judgment due to mental illness or intoxication states. Even if the police can make that distinction rapidly that does not mean they can easily use a different approach to the person with mental illness. Police officers have been injured or killed in these situations.
There seems to be a great deal of misunderstanding and continued bias about how these situations can occur. It can happen as rapidly as waking up one morning finding out that your entire state of consciousness has changed. That gas company truck across the street is there to monitor you and direct microwaves at you. The phones and your computer are bugged. Going to work that morning you decide you need to take evasive action because it seems like you are being followed. Your anxiety levels build all day and that night at home you can't sleep. You decide you need to move the refrigerator in front of the door because you had the thought that it would be too easy for government agents to kick the door down and grab you. You do a Google search on microwaves and decide these people are trying to do a lot more than harass you - they are trying to kill you. You start to make plans on that basis.
That is how paranoid delusions evolve and how they change your behavior. You are no longer making rational assessments of the environment. Your brain has come up with a theory and you are now interpreting all of the environmental information according to that theory. When I approach the problem psychotherapeutically, I generally explain that delusional thoughts are very low probability explanations or interpretations of an event in the environment. I illustrate this by asking the question: "If we had 100 people in the room right now - how many of them would agree with what you just told me?" Many people know that hardly anyone would agree with them, but that doesn't stop them from continuing to misinterpret the data or trying to cast me with everyone else who either doesn't believe them or is just saying that they are "crazy".
Before I outline an approach to the problem of people experiencing episodes of psychosis or mania and running into problems with law enforcement consider what gets in the way of any of early intervention? Keeping with my cardiology comparison from a previous post - most people know that chest pain is a warning sign for a possible heart attack. With continued public health interventions most people know cardiac risk factors. Public health intervention has been so effective that the current campaign is focused on decreasing the denial in women and decreasing cardiac sudden death in women. Two generations of public health intervention are associated with a decreasing rate of cardiac mortality.
How does that compare with psychosis and mania? I have never seen a public service ad advising about the warning signs of psychosis or mania. There are countless euphemisms for acute changes in a persons mental status. The public treats it like a mystery. When a tragedy occurs there is often no explanation or an inadequate one like "some sort of mental illness." The cultural approach is an obstacle to a rational approach to helping affected individuals. Stigma is considered to be a factor, but it could as easily be an artifact of the process. What would be a better approach?
I have been advocating a public health approach to the problem for a long time now. At a political level there is a lot of confusion about whether this is a firearms issue. Firearms are just a subset of the problem. The overriding public health goal is to get people the help that they need as soon as possible. Our current system of care is set up to provide minimal care to people with severe mental illnesses. The level of care and condition of the facilities where the care occurs is widely known in communities and most people do not want to access these facilities for help. I hear a lot about the concern that someone is going to be stigmatized by treatment at a psychiatric facility. I think it is as likely that many facilities are substandard physical plants that are poorly managed. Based on the length of stay policies alone, nobody wants to bring their relative to a facility that has a reputation for discharging partially stabilized people back into the community. The long term goal needs to be improving the quality of psychiatric facilities in addition to changing the culture about severe mental illness.
I thought of a public service announcement that would potentially have the same advertising power as some of the more popular health spots like the "7 warning signs of cancer". I call it the 4 warning signs of severe mental illness. A concerted effort to focus on severe mental illnesses that can potentially lead to errors in judgment is a logical way to approach this problem. Based on my previous paragraph it takes a much more enlightened approach to treating the problem. Health care systems in general are not friendly to people with severe mental illnesses. There are no specialty centers designed to cater to their needs like the high margin businesses get. Many of these health care organizations sponsor walks for mental illness and other programs like National Depression Screening day. But none of them say - if you have these symptoms we want to see you and treat you in a hospitable environment.
That attitude has to change to prevent the loss of innocent lives as the direct result of severe mental illness.
George Dawson, MD, DFAPA
Friday, October 4, 2013
The Dog Quadrant

Before anyone gets the wrong idea, this post is not about pet therapy. It is not about the purported advantages of owning a dog. It is not even about the new research on dog intelligence that I was frankly surprised by, especially the research showing how easily dogs can beat non-human primates on specific tasks. So much for that massive frontal cortex conferring supreme advantage over the animal kingdom. No - this is about managed care and using the term "dog" in its pejorative context.
Several years ago, I was burned out and suffering from the type of large scale mismanagement that is so common in organizations that run on managed care principles. I attempted to approach the problem with humor by reading Dilbert cartoons. Read the first few pages in the Dogbert Management Handout to see what I mean. I soon realized that this stuff was too close to the truth about health care management and decided to look for other management styles.
I happened across the work of Peter Drucker and his ideas about managing knowledge workers that were considered revolutionary. There was certainly nothing like that going on in health care. The managed care approach to managing physicians was to actually treat them like they were not knowledge workers but assembly line workers. Drucker's stroke of genius was in recognizing that managers know much less about products and processes than knowledge workers and that the business was essentially the product of the knowledge workers. Managed care techniques are diametrically opposed and are based on the fact that business guidelines are somehow relevant to medical care and even may actually be called medical quality. There is no health care process more autocratic and primitive than managed care. I have reviewed how this bizarre set of circumstances evolved in several posts on this blog.
Along the way, I also interviewed a health care business management expert and asked him if there were any definitive texts that are used to train business people about managing health care and he referred me to the text Strategic Management of Health Care Organizations. I started to read and study the text, initially trying to find out why Drucker was completely ignored by health care managers. That was when I encountered the BCG Analysis for a Health Care Institution (p 254). BCG is an abbreviation for Boston Consulting Group who came up with this technique for analyzing products and services. In this case, there was a four quadrant graph that differences in market growth rate and relative market share position. I don't have permission to reproduce it here so I will do my best to describe it briefly. The high growth/high market share quadrant was termed "Stars" and contained services like orthopedics, cardiology, oncology, and women's service. The medium/high and high/low quadrants were called "Cash Cows" and "Problem Children". The lower right hand quadrant of the graphic were the "Dogs" and they included psychiatry, ENT, pediatrics and others.
I am no financial analyst, but what is wrong with this picture? Let me give you a hint. If you have a portfolio of medical services and one of them is selected for rationing and the others are not - it should easily end up in the Dog quadrant. The selective rationing of psychiatric and mental health services is a known fact for the last 30 years. When you ration a service you naturally slow its growth and reduce the market share. The market share is reduced even more precipitously when you start shutting down bed capacity and hospitals. Early in the course of all of these events some high profile teaching units in hospitals affiliated with prestigious medical schools were shut down and it was described as being secondary to a lack of reimbursement from companies using managed care models. If you are in a business that severely distorts the market by controlling growth and market share it makes little sense to pretend that you can analyze portfolios across an imaginary market and make decisions about resource allocation in an organization.
If you were a physician unlucky enough to be trapped in this process it played out in several ways. There were endless meetings that formed the base of misinformation. There was the suggestion that productivity was the only fair way to reimburse physicians and the implication that some physicians were much less productive than others. That was a good way to provoke the competitive, even though in practically all cases that was not true. Then there was the usual barrage of financial information. Overhead figures from who knows where. The suggestion that physicians may need to cover the salaries of any physician assistants working with them. It was an unending painful process designed to give the appearance that physicians had a say in the business, except at every critical decision they did not. In the end all there were was a long series of Dogbert management PowerPoints.
I have not seen the latest edition of the book and I wonder if there have been any additional pejorative classifications for mental health or psychiatry. One thing is for sure. You don't end up in the Dog quadrant because of lack of real demand or free markets. You end up in the Dog quadrant because of managed care and their supporters in the government.
And then they can use this analysis to remove even more resources.
George Dawson, MD, DFAPA
Thursday, October 3, 2013
Psychotherapy Has No Image Problem - Psychotherapy Has a Managed Care Problem
There was an opinion piece in the New York Times a few days ago entitled "Psychotherapy's Image Problem". The author goes on to suggest that despite empirical evidence of effectiveness and a recent study showing a patient preference for psychotherapy - it appears to be in decline. He jumps to the conclusion that this is due to an image problem, namely that primary care physicians, insurers, and therapists are unaware of the empirical data. That leads to a lack of referrals and for some therapists use of therapies that are not evidence based - further degrading the field. He implicates Big Pharma in promoting the image of medications and that the evidence base for medication has been marketed better. He implicates the American Psychiatric Association in promoting medications and suggests that the guidelines are biased against psychotherapies.
I am surprised how much discussion this post has received as though the contention of the author is accurate. Psychotherapy has no image problem as evidenced by one the references he cites about the fact that most patients prefer it. It wasn't that long ago that the famous psychotherapy journal Consumer Reports surveyed people and concluded that not only were psychotherapy services preferred, they were found as tremendously helpful by the majority of people who used them. That study was not scientifically rigorous but certainly was effective from a public relations standpoint.
The idea that psychiatry is promoting drugs over psychotherapy seems erroneous to me. The APA Guidelines certainly suggest psychotherapy as first line treatments and treatments that are part of selecting a therapeutic approach to the patient's problems. Psychopharmacology is also covered and in many cases there are significant qualifications with the psychopharmacology. Further there are a number of psychiatrists who lecture around the country who are strong advocates for what are primarily psychotherapeutic approaches to significant disorders like borderline personality disorder and obsessive compulsive disorder. Psychiatrists have also been leaders in the field of psychotherapy of severe psychiatric disorders and have been actively involved in that field for decades. Even psychopharmacology seminars include decision points for psychotherapy either as an alternate modality to pharmacological approaches or a complementary one. What is omitted from the arguments against psychiatry is that many payers do not reimburse psychiatrists for doing psychotherapy.
The author's action plan to politically promote the idea that psychotherapy is evidence based and deserves more utilization is doomed to fail because the premises of his argument are inaccurate. There is no image problem based on psychiatry - if anything the image is enhanced. There is definitely a lack of knowledge about psychotherapy by primary care physicians and it is likely that is a permanent deficit. Primary care physicians don't have the time, energy, or inclination to learn about psychotherapy. In many cases they have therapists in their clinic and just refer any potential mental health problems to those therapists. In other cases, the health plan that primary care physicians work for has an algorithm that tells them to give the patient a 2 minute depression rating scale and prescribe them an antidepressant or an anxiolytic.
And that is the real problem here. Psychotherapists just like psychiatrists are completely marginalized by managed care and business tactics. If you are a managed care company, why worry about insisting that therapists send you detailed treatment plans and notes every 5 visits for a maximum of 20 visits per year when you can just eliminate them and suggest that you are providing high quality services for depression and anxiety by following rating scale scores and having your primary care physicians prescribe antidepressants?. The primary care physicians don't even have to worry if the diagnosis is accurate anymore. The PHQ-9 score IS the diagnosis. Managed care tactics have decimated psychiatric services and psychotherapy for the last 20 years.
It has nothing to do with the image of psychotherapy. It has to do with big business and their friends in government rolling over professionals and claiming that they know more than those professionals. If you really want evidence based - they can make up a lot of it. Like the equation:
rating scale + antidepressants = quality
If I am right about the real cause of the decreased provision of psychotherapy, the best political strategy is to expose managed care and remember that current politicians and at least one federal agency are strong supporters of managed care.
George Dawson, MD, DFAPA
Brandon A. Guadiano. Psychotherapy's Image Problem. New York Times September 29, 2013.
I am surprised how much discussion this post has received as though the contention of the author is accurate. Psychotherapy has no image problem as evidenced by one the references he cites about the fact that most patients prefer it. It wasn't that long ago that the famous psychotherapy journal Consumer Reports surveyed people and concluded that not only were psychotherapy services preferred, they were found as tremendously helpful by the majority of people who used them. That study was not scientifically rigorous but certainly was effective from a public relations standpoint.
The idea that psychiatry is promoting drugs over psychotherapy seems erroneous to me. The APA Guidelines certainly suggest psychotherapy as first line treatments and treatments that are part of selecting a therapeutic approach to the patient's problems. Psychopharmacology is also covered and in many cases there are significant qualifications with the psychopharmacology. Further there are a number of psychiatrists who lecture around the country who are strong advocates for what are primarily psychotherapeutic approaches to significant disorders like borderline personality disorder and obsessive compulsive disorder. Psychiatrists have also been leaders in the field of psychotherapy of severe psychiatric disorders and have been actively involved in that field for decades. Even psychopharmacology seminars include decision points for psychotherapy either as an alternate modality to pharmacological approaches or a complementary one. What is omitted from the arguments against psychiatry is that many payers do not reimburse psychiatrists for doing psychotherapy.
The author's action plan to politically promote the idea that psychotherapy is evidence based and deserves more utilization is doomed to fail because the premises of his argument are inaccurate. There is no image problem based on psychiatry - if anything the image is enhanced. There is definitely a lack of knowledge about psychotherapy by primary care physicians and it is likely that is a permanent deficit. Primary care physicians don't have the time, energy, or inclination to learn about psychotherapy. In many cases they have therapists in their clinic and just refer any potential mental health problems to those therapists. In other cases, the health plan that primary care physicians work for has an algorithm that tells them to give the patient a 2 minute depression rating scale and prescribe them an antidepressant or an anxiolytic.
And that is the real problem here. Psychotherapists just like psychiatrists are completely marginalized by managed care and business tactics. If you are a managed care company, why worry about insisting that therapists send you detailed treatment plans and notes every 5 visits for a maximum of 20 visits per year when you can just eliminate them and suggest that you are providing high quality services for depression and anxiety by following rating scale scores and having your primary care physicians prescribe antidepressants?. The primary care physicians don't even have to worry if the diagnosis is accurate anymore. The PHQ-9 score IS the diagnosis. Managed care tactics have decimated psychiatric services and psychotherapy for the last 20 years.
It has nothing to do with the image of psychotherapy. It has to do with big business and their friends in government rolling over professionals and claiming that they know more than those professionals. If you really want evidence based - they can make up a lot of it. Like the equation:
rating scale + antidepressants = quality
If I am right about the real cause of the decreased provision of psychotherapy, the best political strategy is to expose managed care and remember that current politicians and at least one federal agency are strong supporters of managed care.
George Dawson, MD, DFAPA
Brandon A. Guadiano. Psychotherapy's Image Problem. New York Times September 29, 2013.
Tuesday, October 1, 2013
What JAMA Psychiatry Doesn't Know About Patient Dumping
JAMA Psychiatry recently posted commentary on a form of patient dumping that I described in a previous post as Greyhound therapy. The authors' post an impressive chart of state mental health budget cuts and some of the associated problems. Their solution to the problem "opening a dialogue among providers, funding agencies, and Congress" is a non solution that suggests a lack of appreciation for the details of the problems and how the system of care for people with serious mental illnesses has been systematically dismantled and is no longer capable of providing quality or innovative psychiatric care. To illustrate my point consider the following 8 points:
1. The myth of dangerousness is all encompassing. At some point the government and the managed care industry wanted to make the rationale for admissions to psychiatric units as difficult as possible to ration inpatient psychiatric care. The standard question is: "Is this person a danger to themselves or anyone else." This bias has completely disrupted inpatient care. We now have desperate people who should have been admitted who are lying about suicidal ideation in order to get admitted. We have people who don't need to be admitted saying they are suicidal and getting admitted. The point is that this criteria is irrelevant for a whole range of indications for inpatient treatment. As an example, anyone with a familiy member who has severe mental illness recognizes that there are times when they are completely unable to function due to their illness. Leaving that person at home to fend for themselves in that condition is not only a bad idea it is inhumane and yet they may not meet somebody's criteria for "dangerousness".
2. Length of stay in all community based psychiatric units is based on DRG payments. That means there is a set reimbursement for a diagnosis related stay independent of how long the patient is in the hospital. As an example a psychosis DRG is one of the commonest DRGs and the last reliable figure I have is that it pays $4,500 per DRG. That is set by the federal regulatory agency for Medicare reimbursement but practically every managed care and insurance company pays the same way either per admission or per discharge. If the patient stays 5 days that is nearly the mythical "$1,000/day" that most people believe the hospital is reimbursed. If the stay is 30 days that is $150/day and less that the cost of most board and care homes. This is a strong financial incentive for the hospital to discharge the patient as soon as possible.
3. Despite an emphasis on biological treatments in inpatient settings, there really are no biological treatments that work in the 5 days. That is the length of stay most hospitals want their patients discharged in. Most inpatient experts will tell you that severe mental illnesses (as opposed to crisis intervention) often require at least 2 - 4 weeks for stabilization.
4. Available social service providers have no incentive to assist the hospital with placement irrespective of whether there is adequate housing or not. The hospital is the least expensive place to house the patient, even if they are stable for discharge.
5. The economic incentives result in a large patient population that circulates from homelessness to emergency departments to inpatient care. These same incentives result in the patient being exposed to no single environment that results in their stabilization. In fact providing thousands of dollars of discharge medications to people who will probably never take them is a massive inefficiency that creates an illusion that inpatient treatment has done something. My personal conversations and correspondence with many outpatient psychiatrists confirms that most of them consider inpatient care to be a complete waste of time and they acknowledge that they have no good place to send their patients anymore for stabilization.
6. The same managed care companies that denied hospital claims many years ago currently own the facilities. They now have case managers essentially running their inpatient treatment and telling the physicians there when a patient must be discharged. If the doctors working in that environment don't go along they can be forced out or placed in an uncomfortable enough position that they quit. Managed care companies frequently have proprietary and arbitrary guidelines that dictate when people are discharged. It is not a coincidence that the suggested lengths of stay are expected to maximize profits and have nothing to do with quality psychiatric care.
7. Utilization reviewers still exist. Their job is basically to argue with inpatient physicians and harass them enough so that they discharge the patient. These physicians were supposed to be "peers" but in my experience talking with them over the years, it was apparent that I was not talking with anyone who had actually worked in an inpatient unit. Their job was clearly to force me to get the person out of the hospital or play the trump card by denying payment and getting the hospital to force me to get the patient out. You might ask yourself why they are necessary if their company is paying a fixed fee for inpatient care and I think that is a good question.
8. The trivial reimbursement for inpatient care deincentivizes access to other assessment and treatment modalities that the patient may need such as specialty consultation, brain imaging, and electroencepaholgraphy. Patients may be told to come back for outpatient appointments when the treating psychiatrist knows that patient will not return for the necessary appointments and will probably be readmitted soon with the exact same medical problem.
All of these issues combined are why people are discharged to the street or put on a bus. You can see that the common theme here is actually the rationing of services by the government and managed care industry as well as psychiatry's inability to deliver the quality of care that psychiatrists are trained to provide in this restricted environment. The suggested solutions in the authors article seem to be written by Joint Commission bureaucrats and will have little impact.
This is a problem that can be solved by psychiatrists but it has to start with a quality approach. Inpatient specialty training in psychiatry with a focus on providing state of the art assessment and care is necessary. It is an ideal place to begin to attend to the cognitive dimension of psychotic disorders and mood disorders. Civil commitment laws need to be reformed with a focus on treatment rather than dangerousness. There needs to be an appropriate hand-off from the hospital team to a community team and a housing team. It is the time to stop demanding "cost effective" treatment from a system that has been practically rationed into non-existence. It is time to invest in quality to the point that patients with severe mental illness and their families can expect that there will be psychiatric services available as a resource on par with the cardiology services they expect for any middle aged person with chest pain.
George Dawson, MD, DFAPA
1. Das S, Fromont SC, Prochaska JJ. Bus Therapy: A Problematic Practice in Psychiatry. JAMA Psychiatry. 2013 Sep 25. doi: 10.1001/jamapsychiatry.2013.2824. [Epub ahead of print] PubMed PMID: 24068366.
1. The myth of dangerousness is all encompassing. At some point the government and the managed care industry wanted to make the rationale for admissions to psychiatric units as difficult as possible to ration inpatient psychiatric care. The standard question is: "Is this person a danger to themselves or anyone else." This bias has completely disrupted inpatient care. We now have desperate people who should have been admitted who are lying about suicidal ideation in order to get admitted. We have people who don't need to be admitted saying they are suicidal and getting admitted. The point is that this criteria is irrelevant for a whole range of indications for inpatient treatment. As an example, anyone with a familiy member who has severe mental illness recognizes that there are times when they are completely unable to function due to their illness. Leaving that person at home to fend for themselves in that condition is not only a bad idea it is inhumane and yet they may not meet somebody's criteria for "dangerousness".
2. Length of stay in all community based psychiatric units is based on DRG payments. That means there is a set reimbursement for a diagnosis related stay independent of how long the patient is in the hospital. As an example a psychosis DRG is one of the commonest DRGs and the last reliable figure I have is that it pays $4,500 per DRG. That is set by the federal regulatory agency for Medicare reimbursement but practically every managed care and insurance company pays the same way either per admission or per discharge. If the patient stays 5 days that is nearly the mythical "$1,000/day" that most people believe the hospital is reimbursed. If the stay is 30 days that is $150/day and less that the cost of most board and care homes. This is a strong financial incentive for the hospital to discharge the patient as soon as possible.
3. Despite an emphasis on biological treatments in inpatient settings, there really are no biological treatments that work in the 5 days. That is the length of stay most hospitals want their patients discharged in. Most inpatient experts will tell you that severe mental illnesses (as opposed to crisis intervention) often require at least 2 - 4 weeks for stabilization.
4. Available social service providers have no incentive to assist the hospital with placement irrespective of whether there is adequate housing or not. The hospital is the least expensive place to house the patient, even if they are stable for discharge.
5. The economic incentives result in a large patient population that circulates from homelessness to emergency departments to inpatient care. These same incentives result in the patient being exposed to no single environment that results in their stabilization. In fact providing thousands of dollars of discharge medications to people who will probably never take them is a massive inefficiency that creates an illusion that inpatient treatment has done something. My personal conversations and correspondence with many outpatient psychiatrists confirms that most of them consider inpatient care to be a complete waste of time and they acknowledge that they have no good place to send their patients anymore for stabilization.
6. The same managed care companies that denied hospital claims many years ago currently own the facilities. They now have case managers essentially running their inpatient treatment and telling the physicians there when a patient must be discharged. If the doctors working in that environment don't go along they can be forced out or placed in an uncomfortable enough position that they quit. Managed care companies frequently have proprietary and arbitrary guidelines that dictate when people are discharged. It is not a coincidence that the suggested lengths of stay are expected to maximize profits and have nothing to do with quality psychiatric care.
7. Utilization reviewers still exist. Their job is basically to argue with inpatient physicians and harass them enough so that they discharge the patient. These physicians were supposed to be "peers" but in my experience talking with them over the years, it was apparent that I was not talking with anyone who had actually worked in an inpatient unit. Their job was clearly to force me to get the person out of the hospital or play the trump card by denying payment and getting the hospital to force me to get the patient out. You might ask yourself why they are necessary if their company is paying a fixed fee for inpatient care and I think that is a good question.
8. The trivial reimbursement for inpatient care deincentivizes access to other assessment and treatment modalities that the patient may need such as specialty consultation, brain imaging, and electroencepaholgraphy. Patients may be told to come back for outpatient appointments when the treating psychiatrist knows that patient will not return for the necessary appointments and will probably be readmitted soon with the exact same medical problem.
All of these issues combined are why people are discharged to the street or put on a bus. You can see that the common theme here is actually the rationing of services by the government and managed care industry as well as psychiatry's inability to deliver the quality of care that psychiatrists are trained to provide in this restricted environment. The suggested solutions in the authors article seem to be written by Joint Commission bureaucrats and will have little impact.
This is a problem that can be solved by psychiatrists but it has to start with a quality approach. Inpatient specialty training in psychiatry with a focus on providing state of the art assessment and care is necessary. It is an ideal place to begin to attend to the cognitive dimension of psychotic disorders and mood disorders. Civil commitment laws need to be reformed with a focus on treatment rather than dangerousness. There needs to be an appropriate hand-off from the hospital team to a community team and a housing team. It is the time to stop demanding "cost effective" treatment from a system that has been practically rationed into non-existence. It is time to invest in quality to the point that patients with severe mental illness and their families can expect that there will be psychiatric services available as a resource on par with the cardiology services they expect for any middle aged person with chest pain.
George Dawson, MD, DFAPA
1. Das S, Fromont SC, Prochaska JJ. Bus Therapy: A Problematic Practice in Psychiatry. JAMA Psychiatry. 2013 Sep 25. doi: 10.1001/jamapsychiatry.2013.2824. [Epub ahead of print] PubMed PMID: 24068366.
Sunday, September 29, 2013
A Familiar Story - Another Shooting
The story is familiar and the media writes about it the same way. A mass shooting and the shooter has anger control problems, social problems, and finally probable symptoms of psychosis. The "ELF" considerations here were interesting. ELF is extremely low frequency as specified in this Wiki primer that covers most of the relevant facts. I grew up about 30 miles away from the original ELF site in Clam Lake, Wisconsin and there were plenty of conspiracy theories and environmental concerns right in the area at the time that surrounded this project including the effect of ELF on the residents.
The usual interviews with politicians about gun access and psychiatrists about whether or not violence can be predicted. It is a very familiar sequence of events. The White House is less vocal this time because I think everyone realizes that the government has no interest in solving the problem. You can click on mass homicide and mass shooting and see my previous posts on the matter for a more complete elaboration. There seems to be nothing new in the response to this mass shooting other than the question of security at American military installations.
My response is also the same and it is basically the following:
1. Mass homicide is a public health problem that can be addressed with public health interventions.
2. Violence and homicide prevention can occur even in the absence of firearm legislation.
3. Violence and homicide prevention does not require prediction of future events but the capacity to recognize markers of violence and psychiatric disorders and respond to them appropriately.
4. There need to be accessible speciality programs for the safe assessment and treatment of people with severe mental illnesses and aggressive behavior. That includes the assessment of threats since they are the precursors to the actual violence.
5. A standardized legal approach to the problem of the potentially dangerous person and whether or not mental illness is a factor is necessary.
6. A comprehensive policy that addresses the issues of progressively inadequate mental health funding is necessary to reverse these trends will provide the funding.
All of the above elements require a standardized approach to the care of the aggressive person and there are several clear reasons why that does not happen. The so-called mental health systems is fragmented and it has been for decades. It is basically designed to ration rather than provide care. That is a massive conflict of interest. Until that is acknowledged by the politicians and advocates nothing will be accomplished. It is very hard for politicians to acknowledge when they are backing a national agency that essentially endorses rationing and managed care. You can also compare my writing and suggested solutions to this problem to a recent "call to action" by American Psychiatric Association President Jeffrey A. Lieberman, MD.
How many "calls to action" does the APA need?
George Dawson, MD, DFAPA
The usual interviews with politicians about gun access and psychiatrists about whether or not violence can be predicted. It is a very familiar sequence of events. The White House is less vocal this time because I think everyone realizes that the government has no interest in solving the problem. You can click on mass homicide and mass shooting and see my previous posts on the matter for a more complete elaboration. There seems to be nothing new in the response to this mass shooting other than the question of security at American military installations.
My response is also the same and it is basically the following:
1. Mass homicide is a public health problem that can be addressed with public health interventions.
2. Violence and homicide prevention can occur even in the absence of firearm legislation.
3. Violence and homicide prevention does not require prediction of future events but the capacity to recognize markers of violence and psychiatric disorders and respond to them appropriately.
4. There need to be accessible speciality programs for the safe assessment and treatment of people with severe mental illnesses and aggressive behavior. That includes the assessment of threats since they are the precursors to the actual violence.
5. A standardized legal approach to the problem of the potentially dangerous person and whether or not mental illness is a factor is necessary.
6. A comprehensive policy that addresses the issues of progressively inadequate mental health funding is necessary to reverse these trends will provide the funding.
All of the above elements require a standardized approach to the care of the aggressive person and there are several clear reasons why that does not happen. The so-called mental health systems is fragmented and it has been for decades. It is basically designed to ration rather than provide care. That is a massive conflict of interest. Until that is acknowledged by the politicians and advocates nothing will be accomplished. It is very hard for politicians to acknowledge when they are backing a national agency that essentially endorses rationing and managed care. You can also compare my writing and suggested solutions to this problem to a recent "call to action" by American Psychiatric Association President Jeffrey A. Lieberman, MD.
How many "calls to action" does the APA need?
George Dawson, MD, DFAPA
Saturday, September 28, 2013
Lessons About Clarity and Boundaries from a Sound Engineer
I read Jason Kottke's blog on a regular basis, probably because he posts a lot of stuff that is just interesting from the standpoint of human communication and analysis. The latest item that caught my eye was this 20 year old letter to the band Nirvana by their prospective sound engineer - Steve Albini. To set the context for this letter, Nirvana had released one of the the highest selling rock albums of all time two years earlier, so at the time this letter was penned the group was huge. There is also a documentary out there about the production of that album with commentary from that sound engineer (Butch Vig) and his analysis of the group and the recording that is very interesting. So the group was huge and they probably had access to the same sound engineer who made the most successful rock album of all time. I looked at my copy of In Utero and confirmed that the band did in fact hire Albini. The hiring and ultimate product was not without controversy and there are 48 references to Albini in the Wiki piece on In Utero, some of them referring back to the original letter. I thought it was a remarkable document about providing service, the parameters of that service and the associated philosophy. I will use a brief excerpt of this letter as an example:
"#2: I do not consider recording and mixing to be unrelated tasks which can be performed by specialists with no continuous involvement. 99 percent of the sound of a record should be established while the basic take is recorded. Your experiences are specific to your records; but in my experience, remixing has never solved any problems that actually existed, only imaginary ones. I do not like remixing other engineer's recordings, and I do not like recording things for someone to remix. I have never been satisfied with either version of that methodology......"
This letter does contain the rough language that you would expect to hear from young men before they recognize the value of language that never needs to be censored, but there are potentially important lessons.
I have had the privilege of talking with people in considerable detail about their medical, psychiatric, social and family histories since about 1978. That is a long time by anybody's standard. There are some things that jump out of those interviews that seem to not change over time. I am always surprised by the implicit rather than explicit agreements between physicians and their patients. That is especially true since managed care companies started dictating the practice parameters of their physician employees on a large scale basis. I wonder if things might be a lot better if the relationship between a doctor and his/her patient was not spelled out as clearly as the letter from this sound engineer. I thought I would compose a parallel letter. It might go something like this .
That is my first attempt to write a letter about what you might expect in seeing me for psychiatric treatment. I intentionally wrote it in a manner similar to Steve Albini when he described what it might be like to employ him as a sound engineer. The whole idea of being very clear with people about what they can expect and how they need to interact with psychiatrists in treatment has never been more critical. For all of my career (so far) I have been an employee of a healthcare organization. In that situation that adds a dimension to the treatment contract. For example, do the organization that employs you have the same priorities and the same approach to patient care? If not, it might be very difficult for you to pen a sample letter like the one I have written. You can't really talk about psychotherapy or even lengthy evaluations if your organization allows you to see patients in 10-20 minute appointments to refill their medications.
I am very interested in hearing what other psychiatrists would add or subtract to what I have so far. I would also be interested in hearing about any existing letters. I think they would also be very useful for psychiatrists starting out of residency or psychiatrists going into private practice after years of working as an employee.
George Dawson, MD, DFAPA
If you send me a letter, with your permission I will scan them into Dropbox and post the links right here with any title that you want me to use including "anonymous":
"#2: I do not consider recording and mixing to be unrelated tasks which can be performed by specialists with no continuous involvement. 99 percent of the sound of a record should be established while the basic take is recorded. Your experiences are specific to your records; but in my experience, remixing has never solved any problems that actually existed, only imaginary ones. I do not like remixing other engineer's recordings, and I do not like recording things for someone to remix. I have never been satisfied with either version of that methodology......"
This letter does contain the rough language that you would expect to hear from young men before they recognize the value of language that never needs to be censored, but there are potentially important lessons.
I have had the privilege of talking with people in considerable detail about their medical, psychiatric, social and family histories since about 1978. That is a long time by anybody's standard. There are some things that jump out of those interviews that seem to not change over time. I am always surprised by the implicit rather than explicit agreements between physicians and their patients. That is especially true since managed care companies started dictating the practice parameters of their physician employees on a large scale basis. I wonder if things might be a lot better if the relationship between a doctor and his/her patient was not spelled out as clearly as the letter from this sound engineer. I thought I would compose a parallel letter. It might go something like this .
That is my first attempt to write a letter about what you might expect in seeing me for psychiatric treatment. I intentionally wrote it in a manner similar to Steve Albini when he described what it might be like to employ him as a sound engineer. The whole idea of being very clear with people about what they can expect and how they need to interact with psychiatrists in treatment has never been more critical. For all of my career (so far) I have been an employee of a healthcare organization. In that situation that adds a dimension to the treatment contract. For example, do the organization that employs you have the same priorities and the same approach to patient care? If not, it might be very difficult for you to pen a sample letter like the one I have written. You can't really talk about psychotherapy or even lengthy evaluations if your organization allows you to see patients in 10-20 minute appointments to refill their medications.
I am very interested in hearing what other psychiatrists would add or subtract to what I have so far. I would also be interested in hearing about any existing letters. I think they would also be very useful for psychiatrists starting out of residency or psychiatrists going into private practice after years of working as an employee.
George Dawson, MD, DFAPA
If you send me a letter, with your permission I will scan them into Dropbox and post the links right here with any title that you want me to use including "anonymous":
Sunday, September 22, 2013
Violence and Voices
One of my colleagues posted this NYTimes reference to my Facebook feed this morning. It is written by anthropologist T.M. Luhrmann. She has a number of references in Medline relevant to this article. Her basic thesis is that violent or aggressive auditory hallucinations experienced by people with psychotic disorders are culturally determined. She concludes with the irony that the cultural factors responsible for a lack of will to initiate any meaningful gun control measures may be responsible for more violent auditory hallucinations than are experienced in other cultures.
What is the evidence? She sites a cross cultural study of 40 people with schizophrenia in India and the United States. Across cultures the horrible voice in India were focused on sexual themes and in the US they were focused more on aggression and torture. There were other directive voices focused on routine directions. Not a lot of detail. As a guy who has talked with hundreds of people who were experiencing voices - the common ones are basically background noise like people mumbling or talking at a volume that cannot be understood. Clearer voices clearly comment on the person experiencing them. The comments can vary from routine such as what the person is doing to very negative commentary or ridiculing them. At the extremes voices tell people to harm themselves or others or commit suicide. Those are the typical voices that psychiatrists are trained to ask about for the purpose of assessing dangerousness, but recent studies show that they are probably poor predictors of actual violent acts in clinical settings.
What about the larger observation that voices would incorporate culturally relevant elements? It seems to me that would be a given. As I considered the problem I recalled reading J. Allan Hobson's book The Dreaming Brain when it first came out. He describes acquiring the dream journal of the Engine Man who recorded his dreams in great detail and without interpretation in 1939. The Engine Man was "fascinated by railway trains" and the content of his dreams that he describes and draws contains a lot of that subject material. Railway trains were the technology of the day. They were part of the culture and the conscious states of me interested in technology. Like the Engine Man it is difficult to conceive of a person experiencing voices or delusions without a cultural context.
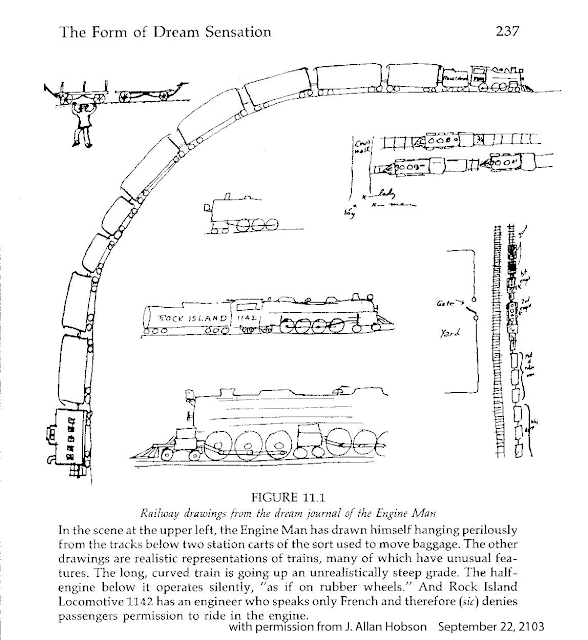
It is difficult to imagine scenarios that lead to voices de novo without exposure to a plausible or even science fiction origin. Hence the common scenario that there is an agency projecting these voices as the most likely cause. It can also imply motivation for the perceptual changes as well as the content. I doubt that voices originating as a beam from the police, the CIA, the FBI or Homeland Security occurred before these agencies were invented.
The other association I had is the theory (or axiom) that the prognosis of schizophrenia is much better in the developing world. This idea came about as the result of a number of World Health Organization Studies and others done in the 1970s to 2000s. Those studies suggest a better prognosis for schizophrenia in the developing world. That theory has been called into question based on methodological considerations by Cohen et al. At the anthropological level, the argument by Dr. Luhrmann reminds me of a similar argument about whether or not primitive peoples were inherently peaceful and became aggressive only after being influenced by social organization. Large scale warfare only becomes possible as the institutions of civilized society grow. Primitive man by nature was inherently peaceful and would get involved only in small scale conflicts around issues like marriage and property. Kealy refers to this as the Myth of the Peaceful Savage. He dispels that myth in his book War Before Civilization and points out that prehistoric man was as aggressive and violent as modern man. Violent and aggressive solutions appear to be universal and it is likely that the culture in America is no more violent than what people experience across the world. The only plausible cultural argument that is rapidly vanishing is the exposure to media violence on a 24/7 basis. At anthropological level, the basic question seems to be why all human societies seem to regard warfare and aggression as an ultimate solution to unresolved conflict.
The larger issue of course is the fact that the experience of hearing voices is much more than that. The entire conscious state is affected. There is not a linear sequence of events that proceeds form a voice to an action. Practically everyone with that experience has a substantial change in their conscious state. The usual stream of consciousness is affected as well as mood state and decision making biases. At times that is detected there can be what appears to be a complete change in the personality of the affected person. The decisions that they currently make cannot be predicted by your past experience with them.
There are several psychotherapeutic approaches to the problem. From a psychiatrist's perspective is is generally necessary and advisable to discuss the voices at some level with the patient. An explanation is necessary that is more than an incomplete biological one as: "You are hearing voices - take this medication and it will get rid of them." Most people are interested in what it means and culturally and individually based meanings are often useful. Some of the preliminary cognitive behavioral therapy of hallucinations emphasizes the need to decrease personal meaning and when that occurs the voices may become less intense and disappear. It should really come as no surprise that talking about voices in certain ways modifies the experience of hearing them or even results in them disappearing. I would liken it to making a conscious decision to wake up during a dream that you don't want to have and then realizing that the dream is gone. Although it has not been investigated I would speculate that this ability would be proportional to the degree that a person's usual conscious state has been affected.
George Dawson, MD, DFAPA
Hobson JA. The Dreaming Brain. Basic Books, Inc. New York, 1988.
TM Luhrmann. The Violence in Our Heads. New York Times September 19, 2013.
Cohen A, Patel V, Thara R, Gureje O. Questioning an axiom: better prognosis for schizophrenia in the developing world? Schizophr Bull. 2008 Mar;34(2):229-44. Epub 2007 Sep 28. Review. PubMed PMID: 17905787; PubMed Central PMCID: PMC2632419.
Kleinman A. Commentary on Alex Cohen et al: "Questioning an axiom: better prognosis for schizophrenia in the developing world". Schizophr Bull. 2008 Mar;34(2):249-50. Epub 2007 Dec 3. PubMed PMID: 18056682; PubMed Central PMCID: PMC2632393.
Keeley LH. War Before Civilization - The Myth of the Peaceful Savage. Oxford University Press, 1996.
What is the evidence? She sites a cross cultural study of 40 people with schizophrenia in India and the United States. Across cultures the horrible voice in India were focused on sexual themes and in the US they were focused more on aggression and torture. There were other directive voices focused on routine directions. Not a lot of detail. As a guy who has talked with hundreds of people who were experiencing voices - the common ones are basically background noise like people mumbling or talking at a volume that cannot be understood. Clearer voices clearly comment on the person experiencing them. The comments can vary from routine such as what the person is doing to very negative commentary or ridiculing them. At the extremes voices tell people to harm themselves or others or commit suicide. Those are the typical voices that psychiatrists are trained to ask about for the purpose of assessing dangerousness, but recent studies show that they are probably poor predictors of actual violent acts in clinical settings.
What about the larger observation that voices would incorporate culturally relevant elements? It seems to me that would be a given. As I considered the problem I recalled reading J. Allan Hobson's book The Dreaming Brain when it first came out. He describes acquiring the dream journal of the Engine Man who recorded his dreams in great detail and without interpretation in 1939. The Engine Man was "fascinated by railway trains" and the content of his dreams that he describes and draws contains a lot of that subject material. Railway trains were the technology of the day. They were part of the culture and the conscious states of me interested in technology. Like the Engine Man it is difficult to conceive of a person experiencing voices or delusions without a cultural context.

It is difficult to imagine scenarios that lead to voices de novo without exposure to a plausible or even science fiction origin. Hence the common scenario that there is an agency projecting these voices as the most likely cause. It can also imply motivation for the perceptual changes as well as the content. I doubt that voices originating as a beam from the police, the CIA, the FBI or Homeland Security occurred before these agencies were invented.
The other association I had is the theory (or axiom) that the prognosis of schizophrenia is much better in the developing world. This idea came about as the result of a number of World Health Organization Studies and others done in the 1970s to 2000s. Those studies suggest a better prognosis for schizophrenia in the developing world. That theory has been called into question based on methodological considerations by Cohen et al. At the anthropological level, the argument by Dr. Luhrmann reminds me of a similar argument about whether or not primitive peoples were inherently peaceful and became aggressive only after being influenced by social organization. Large scale warfare only becomes possible as the institutions of civilized society grow. Primitive man by nature was inherently peaceful and would get involved only in small scale conflicts around issues like marriage and property. Kealy refers to this as the Myth of the Peaceful Savage. He dispels that myth in his book War Before Civilization and points out that prehistoric man was as aggressive and violent as modern man. Violent and aggressive solutions appear to be universal and it is likely that the culture in America is no more violent than what people experience across the world. The only plausible cultural argument that is rapidly vanishing is the exposure to media violence on a 24/7 basis. At anthropological level, the basic question seems to be why all human societies seem to regard warfare and aggression as an ultimate solution to unresolved conflict.
The larger issue of course is the fact that the experience of hearing voices is much more than that. The entire conscious state is affected. There is not a linear sequence of events that proceeds form a voice to an action. Practically everyone with that experience has a substantial change in their conscious state. The usual stream of consciousness is affected as well as mood state and decision making biases. At times that is detected there can be what appears to be a complete change in the personality of the affected person. The decisions that they currently make cannot be predicted by your past experience with them.
There are several psychotherapeutic approaches to the problem. From a psychiatrist's perspective is is generally necessary and advisable to discuss the voices at some level with the patient. An explanation is necessary that is more than an incomplete biological one as: "You are hearing voices - take this medication and it will get rid of them." Most people are interested in what it means and culturally and individually based meanings are often useful. Some of the preliminary cognitive behavioral therapy of hallucinations emphasizes the need to decrease personal meaning and when that occurs the voices may become less intense and disappear. It should really come as no surprise that talking about voices in certain ways modifies the experience of hearing them or even results in them disappearing. I would liken it to making a conscious decision to wake up during a dream that you don't want to have and then realizing that the dream is gone. Although it has not been investigated I would speculate that this ability would be proportional to the degree that a person's usual conscious state has been affected.
George Dawson, MD, DFAPA
Hobson JA. The Dreaming Brain. Basic Books, Inc. New York, 1988.
TM Luhrmann. The Violence in Our Heads. New York Times September 19, 2013.
Cohen A, Patel V, Thara R, Gureje O. Questioning an axiom: better prognosis for schizophrenia in the developing world? Schizophr Bull. 2008 Mar;34(2):229-44. Epub 2007 Sep 28. Review. PubMed PMID: 17905787; PubMed Central PMCID: PMC2632419.
Kleinman A. Commentary on Alex Cohen et al: "Questioning an axiom: better prognosis for schizophrenia in the developing world". Schizophr Bull. 2008 Mar;34(2):249-50. Epub 2007 Dec 3. PubMed PMID: 18056682; PubMed Central PMCID: PMC2632393.
Keeley LH. War Before Civilization - The Myth of the Peaceful Savage. Oxford University Press, 1996.
Saturday, September 21, 2013
American Psychosis - The Final Take
I finished reading E. Fuller Torrey's recently released book American Psychosis - How the Federal Government Destroyed the Mental Illness Treatment System . I recommended it on the basis of a a quick initial read of a brief section on managed care but can provide additional details at this time. I will start with the conclusion. Criticizing an expensive, fragmented, and poorly conceived system of care for severe mental illness is a fairly easy task for any psychiatrist who tries to provide care for the target population of people with schizophrenia, bipolar disorder and severe mood disorders. This book concentrates many of the references about deinstitutionalization, incarceration of the mentally ill, victimization of the mentally ill, and aggression and violence by the mentally ill in one place. In the conclusion Dr. Torrey also recommends some 10 potential solutions to the problems and more importantly suggests the some of these need to be implemented on a small scale rather system wide.
I am sure that Dr. Torrey and the publisher of this book would not be very happy if I put all 10 of his proposed solutions on this blog, so I am going to focus on one that is consistent with my initial post and one of the major themes of this blog:
"For profit funding of of public mental illness services has been tried and it does not work."
This is the real experience of anyone who has worked in psychiatric acute care and by that I mean the hospital in your community where people are brought in by the police on emergency holds. Even in that setting there are levels of acuity. In a metropolitan area there may be 8 or 10 psychiatric inpatient units but only one or two of them will accept patients with high levels of aggression or suicidal behavior. In an ideal world these would be units where there are staff with high levels of expertise in treating these severe conditions, but the reality is that economic considerations are at the top of the list. There needs to be adequate staffing for close supervision and the staff have to be able to deal with high levels of aggression toward self or others. There also needs to be expertise in recognizing and treating alcohol and drug intoxication and withdrawal states. There is usually minimal attention paid to the therapeutic aspects of the environment.
When I first started working in that environment it was the late 1980s. I had just completed a three year stint as the medical director of a very good community mental health clinic that offered case management and Assertive Community Treatment. I was well trained in community psychiatry at the University of Wisconsin Psychiatry Department and it was good to actually practice it with a team of highly motivated people.
The first months on the inpatient unit resulted in several "denials" by insurance company intermediaries functioning to ration care. Keep in mind that all of these patients were in the highest acuity unit in the hospital, had problems with suicidal and aggressive behavior, and many needed detoxification. The rationale of the "peer reviewers" was the the patient did not require acute care or the care could be provided at a less intensive facility. Apart from county detox facilities that had policies against admitting suicidal or aggressive patients - no less intensive facilities existed.
When you are in that environment trying to provide care, it is pretty obvious that this peer review process is basically an insurance company game to make money. In the small print in the denial letters there was an option to appeal all denials to an administrative law judge within the state. I asked my colleagues and nobody had tried that route. I collected 12 denials and requested a hearing in front of the administrative law judge. I took a day of vacation to go to court. A week before the hearing I was informed that my hearing was cancelled and the administrative law judge decided in favor of the insurance company. I appealed to the Attorney General on the basis of conflict of interest stating that the peer reviewers worked for a competing organization and therefore this was anticompetitive activity. The AG informed me that they were independent contractors. How can you be an independent contractor if you collect a paycheck from the organization that is denying care by your competitor? It was clear to me that the state government was very friendly to the managed care industry.
The whole managed care strategy for rationing care or in extreme cases shutting down entire psychiatric units was outlined in my previous post on overutilization. It is the basic money making strategy of managed care organizations. It essentially doubles down on rationing. That occurs because hospitals are paid a set amount for taking care of people regardless of how long they are there and that amount is denied in as many as 10% of cases. If there is one deficiency of this book it is a lack of granularity on this issue. Dr. Torrey approaches the problem as a top down problem of policy deficiency, driven by an ideology that bed capacity could be shut down and not missed either because of the toxicity of state hospital settings or too much faith in the federal initiated community mental health movement.
Assuming that a patient can actually get the level of acute care that they need without being thrown out of the hospital by an insurance company, the fragmentation of care does not stop there. Even though insurance companies say they are emphasizing outpatient care, getting an appointment may be impossible. The prescribed medications may be denied. Housing options or community case management for people with severe mental illness are not usually available unless the insurance changes to a public option.
American Psychosis covers the funding and policy issues on a global level before it gets to the suggested solutions. Excellent examples are given to illustrate these points. For example, North Carolina is given as the example of what happens when a state mental health system is privatized (p 158). The parameters of the dramatic deterioration in services that resulted from this maneuver is a well documented example of what happens when a for-profit entity begins to manage care and shift the responsibility for care of serious mental illnesses to the correctional system.
American Psychosis is a well organized analysis of the problems that occurred as the result of an initiative in the Kennedy administration. It contains a lot of information and references about what has happened as the result of these decisions. There is also a subtext and that is it is written from the perspective of a psychiatrist who has been a thought leader on the issue of treating people with severe mental illness. Only a minority of people in the United States understand that perspective and I think that there will be predictable backlash from the constituencies that believe a severe mental illness is a preferred state and that everyone should have the right to enjoy it.
That is not the experience of any acute care psychiatrist and Dr. Torrey presents that perspective very well.
George Dawson, MD, DFAPA
I am sure that Dr. Torrey and the publisher of this book would not be very happy if I put all 10 of his proposed solutions on this blog, so I am going to focus on one that is consistent with my initial post and one of the major themes of this blog:
"For profit funding of of public mental illness services has been tried and it does not work."
This is the real experience of anyone who has worked in psychiatric acute care and by that I mean the hospital in your community where people are brought in by the police on emergency holds. Even in that setting there are levels of acuity. In a metropolitan area there may be 8 or 10 psychiatric inpatient units but only one or two of them will accept patients with high levels of aggression or suicidal behavior. In an ideal world these would be units where there are staff with high levels of expertise in treating these severe conditions, but the reality is that economic considerations are at the top of the list. There needs to be adequate staffing for close supervision and the staff have to be able to deal with high levels of aggression toward self or others. There also needs to be expertise in recognizing and treating alcohol and drug intoxication and withdrawal states. There is usually minimal attention paid to the therapeutic aspects of the environment.
When I first started working in that environment it was the late 1980s. I had just completed a three year stint as the medical director of a very good community mental health clinic that offered case management and Assertive Community Treatment. I was well trained in community psychiatry at the University of Wisconsin Psychiatry Department and it was good to actually practice it with a team of highly motivated people.
The first months on the inpatient unit resulted in several "denials" by insurance company intermediaries functioning to ration care. Keep in mind that all of these patients were in the highest acuity unit in the hospital, had problems with suicidal and aggressive behavior, and many needed detoxification. The rationale of the "peer reviewers" was the the patient did not require acute care or the care could be provided at a less intensive facility. Apart from county detox facilities that had policies against admitting suicidal or aggressive patients - no less intensive facilities existed.
When you are in that environment trying to provide care, it is pretty obvious that this peer review process is basically an insurance company game to make money. In the small print in the denial letters there was an option to appeal all denials to an administrative law judge within the state. I asked my colleagues and nobody had tried that route. I collected 12 denials and requested a hearing in front of the administrative law judge. I took a day of vacation to go to court. A week before the hearing I was informed that my hearing was cancelled and the administrative law judge decided in favor of the insurance company. I appealed to the Attorney General on the basis of conflict of interest stating that the peer reviewers worked for a competing organization and therefore this was anticompetitive activity. The AG informed me that they were independent contractors. How can you be an independent contractor if you collect a paycheck from the organization that is denying care by your competitor? It was clear to me that the state government was very friendly to the managed care industry.
The whole managed care strategy for rationing care or in extreme cases shutting down entire psychiatric units was outlined in my previous post on overutilization. It is the basic money making strategy of managed care organizations. It essentially doubles down on rationing. That occurs because hospitals are paid a set amount for taking care of people regardless of how long they are there and that amount is denied in as many as 10% of cases. If there is one deficiency of this book it is a lack of granularity on this issue. Dr. Torrey approaches the problem as a top down problem of policy deficiency, driven by an ideology that bed capacity could be shut down and not missed either because of the toxicity of state hospital settings or too much faith in the federal initiated community mental health movement.
Assuming that a patient can actually get the level of acute care that they need without being thrown out of the hospital by an insurance company, the fragmentation of care does not stop there. Even though insurance companies say they are emphasizing outpatient care, getting an appointment may be impossible. The prescribed medications may be denied. Housing options or community case management for people with severe mental illness are not usually available unless the insurance changes to a public option.
American Psychosis covers the funding and policy issues on a global level before it gets to the suggested solutions. Excellent examples are given to illustrate these points. For example, North Carolina is given as the example of what happens when a state mental health system is privatized (p 158). The parameters of the dramatic deterioration in services that resulted from this maneuver is a well documented example of what happens when a for-profit entity begins to manage care and shift the responsibility for care of serious mental illnesses to the correctional system.
American Psychosis is a well organized analysis of the problems that occurred as the result of an initiative in the Kennedy administration. It contains a lot of information and references about what has happened as the result of these decisions. There is also a subtext and that is it is written from the perspective of a psychiatrist who has been a thought leader on the issue of treating people with severe mental illness. Only a minority of people in the United States understand that perspective and I think that there will be predictable backlash from the constituencies that believe a severe mental illness is a preferred state and that everyone should have the right to enjoy it.
That is not the experience of any acute care psychiatrist and Dr. Torrey presents that perspective very well.
George Dawson, MD, DFAPA
Tuesday, September 17, 2013
Buy This Book
I was out of town at a Mayo Clinic seminar and while I was gone, Amazon sent me an e-mail. My copy of American Psychosis - How the Federal Government Destroyed the Mental Illness Treatment System by E. Fuller Torrey had shipped. This is the only book I have really been eager to read for some time. The title is almost exactly what I have been saying for the past 25 years. At last I had somebody who was finally seeing the real problems with the treatment of mental illness in this country. After putting up with obnoxious blogs about how psychiatrists had been bought and paid for by drug companies, manufacturing catastrophes designed by psychiatrists like the recent DSM-5 apocalypse, and an endless number of side shows I was looking for an anchor point that looked at the real problems and what to do about them.
For the purpose of this post I was interested in one thing. What did Dr. Torrey say about managed care? As any reader here should know by now I view managed care as the single worst thing (by far) that has happened to psychiatric care and the treatment of severe mental illness in the United States. Managed care tactics are responsible for decimating psychiatric care, especially hospital based care. Managed care has destroyed psychotherapy and removed practically all of the creativity and innovation from mental health care. Managed care has rationed both access and treatment resources to my patients who have few resources themselves. In order for this book to impress me, it would need to say something about managed care.
Turning to the index there were exactly two pages about "managed care organizations". What exactly did Dr. Torrey say? The introduction to the section is introducing Medicaid as "the largest single fiscal impediment to improving services for mentally ill persons in the United States." The system is gamed by the states to optimize Medicaid reimbursement by the federal government. The example given is the IMD (institute for mental disease) exclusion that disallows Medicaid reimbursement for state hospitals. The states responded by closing down state hospitals and shifting admissions to Medicaid covered acute care settings in community hospitals. According to Torrey cost shifting based on Medicaid has been the driving force behind public services for 40 years.
Managed care enters the picture in paragraph 2: "At least 34 states deliver 'some or all mental health services through managed care arrangements, including care outs and comprehensive managed care organizations (MCOs). States such as California, Utah, Colorado, Pennsylvania, New York, and Massachusetts have used capitation funding, under which providers are paid a fixed amount to deliver all necessary services." Throw Minnesota in there. And also throw in the idea that practically all states ration using managed care strategies to save money - even if there is no formal contract with an MCO.
He goes on to outline the three features that these programs have in common (my comments in italics):
1. The priority is cost savings and not patient care.
Yes! Managed care has nothing to do with increased access or quality. It is all about rationing access to care including access to medications necessary to treat severe mental illness. There is a reference from the NEJM from 1994 that illustrates that rationing these medications has an unfair impact on patient with severe mental illness and increases overall costs but the industry continued the practice unabated despite that study. Cost savings after all is just a politically correct way to designate profits for the MCO. After all, nobody ever realizes any savings in health care it just ends up on the bottom line of the MCO, the pharmaceutical company or the provider.
2. The sickest patients suffer the most under managed care rationing.
Yes! It should be fairly obvious that if you move the group of patients with the most severe problems at a high rate into a rationed system, they are getting proportionately less resources than the severely disabled of any disease category. Dr. Torrey points out that individuals with severe mental illness represent only 11% of all Medicaid beneficiaries but they are 1/3 of all of the high cost beneficiaries.
3. This is a very profitable segment for managed care companies.
Yes! The example given in the book is United Behavioral Health and their claim to 'oversee behavioral health benefits for more than 23 million beneficiaries' including Medicaid patients. He goes on to illustrate the the difference in outcomes for executives of these companies and the mentally ill whose benefits they oversee and points out that the difference in patient outcomes is directly related to that disparity. (see par 19).
He goes on to conclude that the PPACA (aka Obamacare) will change nothing basically because: "It is likely to lead managed care companies finding new and creative ways to not provide services to mentally ill individuals who need the services the most." Talk about innovation.
I could not have said it better myself, but have said it in a number of ways in the past 20 years. I plan to continue to read and analyze this book. I have already purchased it and can certify that the managed care section is accurate if brief. Any objective observer realizes that the government paying the managed care industry for not providing services is the central problem with the provision of treatment to persons with the most severe forms of mental illness. These days it also extends to more common anxiety and depressive disorders treated in a primary care clinic and diagnosed by a very brief screening.
Keep that in mind when you are reading the latest trivia about the DSM, the pharmaceutical industry involvement with psychiatry, debates about clinical trials data for FDA approval, or any number of psychiatric non events that are furiously debated around the Internet. Tax dollars given to an industry to ration services is money that should have gone to provide services to the mentally ill.
George Dawson, MD, DFAPA
For the purpose of this post I was interested in one thing. What did Dr. Torrey say about managed care? As any reader here should know by now I view managed care as the single worst thing (by far) that has happened to psychiatric care and the treatment of severe mental illness in the United States. Managed care tactics are responsible for decimating psychiatric care, especially hospital based care. Managed care has destroyed psychotherapy and removed practically all of the creativity and innovation from mental health care. Managed care has rationed both access and treatment resources to my patients who have few resources themselves. In order for this book to impress me, it would need to say something about managed care.
Turning to the index there were exactly two pages about "managed care organizations". What exactly did Dr. Torrey say? The introduction to the section is introducing Medicaid as "the largest single fiscal impediment to improving services for mentally ill persons in the United States." The system is gamed by the states to optimize Medicaid reimbursement by the federal government. The example given is the IMD (institute for mental disease) exclusion that disallows Medicaid reimbursement for state hospitals. The states responded by closing down state hospitals and shifting admissions to Medicaid covered acute care settings in community hospitals. According to Torrey cost shifting based on Medicaid has been the driving force behind public services for 40 years.
Managed care enters the picture in paragraph 2: "At least 34 states deliver 'some or all mental health services through managed care arrangements, including care outs and comprehensive managed care organizations (MCOs). States such as California, Utah, Colorado, Pennsylvania, New York, and Massachusetts have used capitation funding, under which providers are paid a fixed amount to deliver all necessary services." Throw Minnesota in there. And also throw in the idea that practically all states ration using managed care strategies to save money - even if there is no formal contract with an MCO.
He goes on to outline the three features that these programs have in common (my comments in italics):
1. The priority is cost savings and not patient care.
Yes! Managed care has nothing to do with increased access or quality. It is all about rationing access to care including access to medications necessary to treat severe mental illness. There is a reference from the NEJM from 1994 that illustrates that rationing these medications has an unfair impact on patient with severe mental illness and increases overall costs but the industry continued the practice unabated despite that study. Cost savings after all is just a politically correct way to designate profits for the MCO. After all, nobody ever realizes any savings in health care it just ends up on the bottom line of the MCO, the pharmaceutical company or the provider.
2. The sickest patients suffer the most under managed care rationing.
Yes! It should be fairly obvious that if you move the group of patients with the most severe problems at a high rate into a rationed system, they are getting proportionately less resources than the severely disabled of any disease category. Dr. Torrey points out that individuals with severe mental illness represent only 11% of all Medicaid beneficiaries but they are 1/3 of all of the high cost beneficiaries.
3. This is a very profitable segment for managed care companies.
Yes! The example given in the book is United Behavioral Health and their claim to 'oversee behavioral health benefits for more than 23 million beneficiaries' including Medicaid patients. He goes on to illustrate the the difference in outcomes for executives of these companies and the mentally ill whose benefits they oversee and points out that the difference in patient outcomes is directly related to that disparity. (see par 19).
He goes on to conclude that the PPACA (aka Obamacare) will change nothing basically because: "It is likely to lead managed care companies finding new and creative ways to not provide services to mentally ill individuals who need the services the most." Talk about innovation.
I could not have said it better myself, but have said it in a number of ways in the past 20 years. I plan to continue to read and analyze this book. I have already purchased it and can certify that the managed care section is accurate if brief. Any objective observer realizes that the government paying the managed care industry for not providing services is the central problem with the provision of treatment to persons with the most severe forms of mental illness. These days it also extends to more common anxiety and depressive disorders treated in a primary care clinic and diagnosed by a very brief screening.
Keep that in mind when you are reading the latest trivia about the DSM, the pharmaceutical industry involvement with psychiatry, debates about clinical trials data for FDA approval, or any number of psychiatric non events that are furiously debated around the Internet. Tax dollars given to an industry to ration services is money that should have gone to provide services to the mentally ill.
George Dawson, MD, DFAPA
Subscribe to:
Posts (Atom)