
“Brain fog” or “brain-fog” is a popular term that has
penetrated the medical literature fairly recently. In talking with hundreds of patients who have
used the term in my evaluations most of them mean an actual fogginess to their
mentation. That typically occurs in two
ways. The first is an underwater feeling and noticing that both the
speed and content of thought is not quite up to par. The second is more of a problem in
concentration and focus where it takes a noticeable effort to sustain both. I have personally had these experiences
during illness and probably on a developmental basis. In the case of the illness, I was running my
usual team meeting at about 8AM, and suddenly realized my thoughts were
clouded. I developed chills and knew that there was a mini-epidemic of
influenza in my staff. I told my team members that I had to stop due to illness
and went home. It took about 48 hours
for that to clear. Since that time, I
have been very interested in how infectious diseases and diseases in general have
that effect on the brain.
The closest term that I could think of that might
approximate brain fog is “clouding of consciousness”. This term from descriptive psychiatry and
psychopathology is commonly associated with neurocognitive disorders. It is typically
a criterion for delirium but in most texts, it is also associated with other
anatomical and functional brain disorders.
The best review of the psychopathology and phenomenology of clouding
of consciousness is from Lipowki’s text (1). Lipowski reviews the 2500 year history of
delirium and how confusion and clouding of consciousness became critical
concepts in advancing research in this area.
A lot of the current psychopathology texts have very little
to say about clouding of consciousness and symptoms of delirium. There are a few exceptions. Sims discusses it in a chapter “Consciousness
and Disturbed Consciousness”. He starts
with defining consciousness by three components an inner awareness of
experience, intentional reaction to objects, and knowledge of the conscious
self. He also has an excellent diagram
(Fig 3.1 p. 40) that ties together the medical use of the term, clinical
context, and changes that can occur in that context. Since I cannot get permission to post the diagram
I will describe it. Normal consciousness
is the central component and it is transitioned to reduced wakefulness, sleep,
and stages of sleep and deep sleep.
There is another transition to the unconscious mind (via
preconsciousness). The final transition
is to clouding of consciousness, drowsiness, stupor, and coma. The latter
transition is obviously the only pathological one, but in terns of
psychopathology there is obvious overlap between reduced wakefulness
transitioning to normal sleep and drowsiness that may be a prelude to
neurocognitive disorders. That is also a
critical decision point in thinking about brain fog. Is the underlying mechanism one of reduced
wakefulness or a focal or global decrease in brain metabolism seen in
neurocognitive disorders? Sims also
defines clouding of consciousness as: “most intellectual functions are
impaired including attention and concentration, comprehension and recognition,
understanding, forming associations, logical judgement, communication by speech
and purposeful action”. (p. 41). Sims
definition is most consistent with an early delirious state but not “brain fog”
described by a person who is going to work every day and subjectively feels
that their work performance could be better.
I have followed the evolution of Neuropsychiatric Systemic
Lupus Erythematosus (NPSLE) across the last 3 versions of Lahita’s text on
SLE. There are generally 2 chapters
dedicated to this topic in each text.
Over the years, there has been much more specificity in terms of the
biological mechanisms involved in NPSLE.
There are 19 separate neuropsychiatric syndromes involving
neurocognitive symptoms and constellations of more pure psychiatric symptoms
like anxiety and depression. From a
purely cognitive standpoint, an interesting concept is that many of the
mechanisms that are thought to moderate cognitive function like long term
potentiation (LTP), synaptic plasticity, and neurogenesis are immune cells and
inflammatory molecules. The diagram
below illustrates some upstream perturbations in the cytokine system that can
result in impaired learning and memory.
There are additional immune systems affecting neurogenesis.

In the review that I constructed this diagram from, the
author states: “‘‘Lupus brain fog’’
is
an extremely common patient complaint that refers to periods of forgetfulness
and confusion that are related to impaired cognition.” She cites the range of 21-80% of SLE patients
having some degree of cognitive impairment leading to some degree of disability
or impaired quality of life. NPSLE and
the associated studies of how inflammation and immune function impair learning
and memory is an excellent example of how various disease processes can have
effects on cognition. It is also a good example of how the term “brain fog” has
developed recently in this clinical population with clear CNS pathology. It also suggests a lack of specificity for
the term given the range of impairment.
At this point – a few clinical vignettes of “brain fog” can
be considered as additional examples:
Vignette 1:
60-year-old man referred for assessment and treatment of mania and
possible bipolar disorder. He gives a
history of drinking 750 ml/day of alcohol and appears intoxicated at the time
of the evaluation. As part of the
initial evaluation, he is given a standard cognitive exam and scores a perfect
30/30 points indicating no deficits in orientation, attention span, short term
memory or language skills (comprehension, repetition, or naming). He has no subjective cognitive symptoms. He returns a week later for reassessment and
does not recall meeting the same physician or doing any cognitive testing. He
does not believe he was ever at the clinic in the past.
This patient essentially blacked out or was amnestic
for the initial interview with the psychiatrist. Like many heavy drinkers he has a sustained
mood disturbance at times that resembles manic episodes, but these symptoms
resolve after detoxification and abstinence from alcohol. Patient with these
problems are likely to described brain fog during episodes of
intoxication, withdrawal, detoxification, sleep deprivation from the effects of
alcohol, decreased attention span and concentration that is probably multifactorial
and during mood changes that are alcohol induced. Heavy alcohol consumption can lead to
profound and persistent cognitive changes, most notable from untreated Wernicke
encephalopathy the result of Vitamin B1 deficiency that can accompany persistent
alcohol use.
Vignette 2: 40 yr old woman referred for
assessment of severe anxiety and panic. She attributes both symptoms to
“chronic Lyme disease” despite extended course of antibiotic treatment by
experts and extended treatment by non-medical personnel using more atypical
types of treatment. She was previously
very vigorous and physically active but that is no longer the case. She describes fatigue, hypersomnia, and
“brain fog” that puts her job at risk because of decreasing productivity and
performance. She is being treated with benzodiazepines for anxiety and z-drugs
for sleep.
This is a familiar scenario for psychiatrists. In this case
the patient is diagnosed with a controversial illness and has not recovered
despite very aggressive treatment. She
is anxious because of the decrease in her level of functioning and describes
fatigue, hypersomnia, and brain fog.
It is often difficult to determine the progression of symptoms without detailed
records – depending only on the patient’s recollection of what happened over a
number of years. In these cases I have
found that it is best to track all of these symptoms and see how they fluctuate
with logical changes based on the patients current clinical status. In these
cases I would typically proceed with tapering and discontinuing the
benzodiazepines and z-drugs and monitoring the fatigue, hypersomnia, and brain
fog while simultaneously providing psychotherapy that I thought would be most
effective for the target symptoms.
Vignette 3: 50 yr old man being seen for severe
alcohol use disorder, persistent depression disorder, major depression, chronic
insomnia, and possible attention- deficit/hyperactivity disorder. He has had
lifelong insomnia, onset of chronic depression at age 18, and heavy daily
drinking for the past 15 years. He describes inattentiveness, distractibility,
procrastination, and “brain fog”. He is
requesting that treatment for the “brain fog” be prioritized since it is
currently his most significant problem.
Very common scenario in treatment settings. The ADHD diagnosis is more controversial
lately based on the idea that some people may develop it as an adult. I always ask adults about childhood sleep
problems and it is a very common finding.
Childhood sleep disturbance also results in erroneous diagnoses of ADHD,
but it is often difficult to establish that diagnosis in generations where it
was not emphasized on school. The
diagnosis of alcohol use disorder is a complicating factor. In the case of
heavy drinkers, they are often drinking all day long, in a state of intoxication
or withdrawal, and typically wake up in the middle of the night and need to
decide whether to drink in order to fall back asleep or tolerate withdrawal
until the morning and then drink to reduce more severe withdrawal
symptoms. Clearly, every one of those
transitional states is associated with some cognitive impairment and some have
described it as “brain fog”. An
additional patient-based bias is wish that a medication can correct all of this
cognitive impairment. That wish is
complicated by the fact that many heavy drinkers have used cocaine or
amphetamines to drink more and improve their concentration and attention. They have also used benzodiazepines as a way
to treat insomnia and withdrawal symptoms, especially withdrawal symptoms in
the morning that could otherwise lead driving to work with high blood alcohol
levels and risking legal problems. In all
of these cases, the patient needs to be followed and serially reassessed up to
the 60-day mark. In my experience, the
transient cognitive symptoms should be clear at that point and the baseline symptoms
and their severity can be determined.
If brain fog exists can it be phenomenologically separated from
other psychiatric diagnostic terms?
Sedation or excess somnolence is a common form of clouding of
consciousness. There is a temporal
aspect to both related to a combination of both alerting mechanisms and circadian
rhythms and the biological basis of both has been grossly determined (6). I would anticipate that sedation or
somnolence would fluctuate over the course of the day, with the exception
excessive sleep deprivation or external sources of sedation like a sleeping
agent. Most people tend to describe
brain fog as unrelenting.
In the final analysis, is brain fog a useful term? Is it a colloquialism rather than a technical
term that should be used in medicine? My argument suggests that it may be a
useful descriptor of a sub delirious state or very early clouding of
consciousness. There are multiple
associated etiologies and conditions including some that are just a temporary
disruption in normal physiology. Based
on my clinical experience it is clearly a word that patients frequently use.
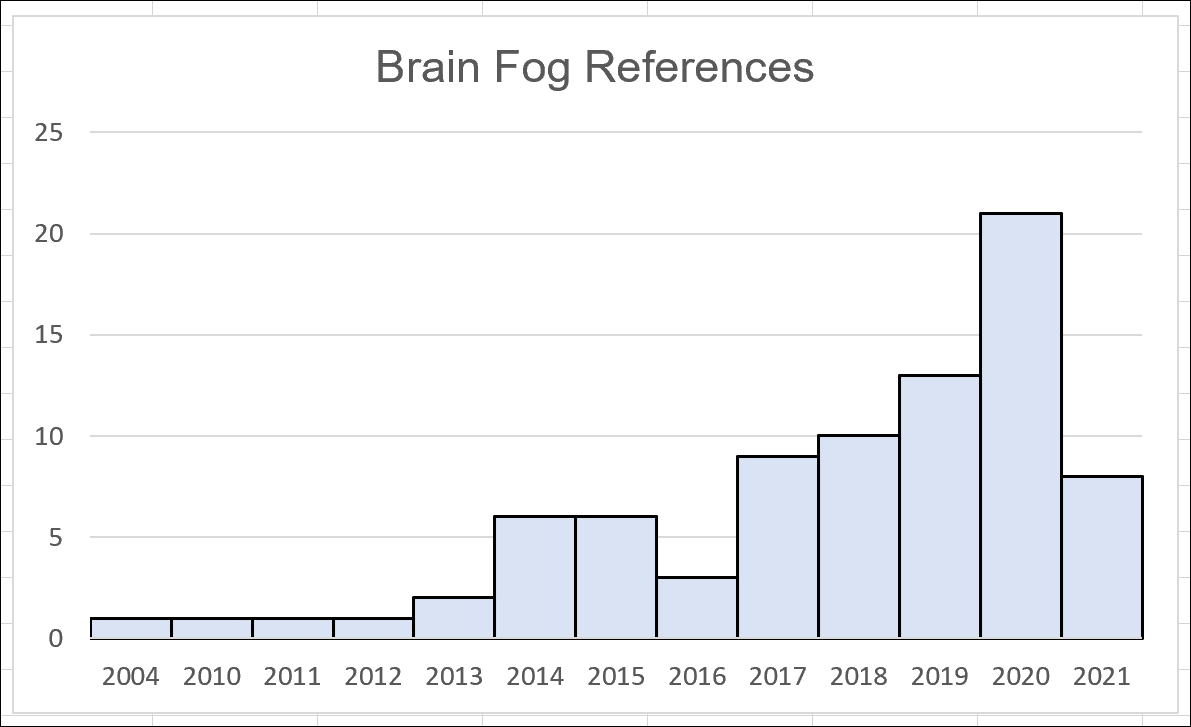
From the PubMed search, it is also being used more frequently in the medical
literature, just over the past 20 years.
A word of caution is needed before it is adopted on any
widespread basis. Lipowski points out how 19th century
psychopathologists advanced the field by specifying a class of disorders based
on clouding of consciousness and confusion arising in the context
of acute brain dysfunction. What
followed was a proliferation of terms that set back further research for
decades (p. 27). Time will tell if the
term becomes more widely adapted or it is fitted into existing nomenclature. Based on the recent tightening of the nomenclature for delirium (7) it is not likely. Since most people seem to be using it to cover
both mild and moderate subjective cognitive impairment - it does not add much precision. On the other hand psychiatrists are focused on the patient’s
subjective state and use of language so it is undoubtedly useful for beginning
the early exploration of the problem that led to the consultation.
George Dawson, MD, DFAPA
References:
1: Lipowski ZJ. Delirium: Acute Confusional States. New York: Oxford University Press, Inc; 1990.
2: Sims A. Symptoms in the Mind: An Introduction to
Descriptive Psychopathology. 3rd ed. Amsterdam: Elsevier Limited;
2003.
3: Mackay M, Ulug
AM, Volpe BT. Neuropsychiatric Systemic
Lupus Erythematosus: Mechanisms of Injury.
In: Lahita RG, Tsokos G, Buyon J,
Kolke T. Systemic Lupus Erythematosus. 5th
ed. London: Academic Press; 2011. p. 491- 512.
4: Hanley J. The Nervous System and Lupus. In: Lahita RG,
Tsokos G, Buyon J, Kolke T. Systemic
Lupus Erythematosus. 5th ed. London: Academic Press; 2011. p.
727-746.
5: Mackay M. Lupus brain fog: a biologic
perspective on cognitive impairment, depression, and fatigue in systemic lupus
erythematosus. Immunol Res. 2015 Dec;63(1-3):26-37. doi:
10.1007/s12026-015-8716-3. PMID: 26481913.
-Reference
5 is an excellent open access review of the relationship between inflammation,
immune systems, and cognition (especially memory and learning).
6: Valentino RJ, Volkow ND. Drugs, sleep, and the addicted brain. Neuropsychopharmacology. 2020 Jan;45(1):3-5. doi: 10.1038/s41386-019-0465-x. Epub 2019 Jul 16. PMID: 31311031; PMCID: PMC6879727.
7: Slooter AJC, Otte WM, Devlin JW, Arora RC, Bleck TP, Claassen J, Duprey MS, Ely EW, Kaplan PW, Latronico N, Morandi A, Neufeld KJ, Sharshar T, MacLullich AMJ, Stevens RD. Updated nomenclature of delirium and acute encephalopathy: statement of ten Societies. Intensive Care Med. 2020 May;46(5):1020-1022. doi: 10.1007/s00134-019-05907-4. Epub 2020 Feb 13. PMID: 32055887; PMCID: PMC7210231.
8: Servick K. COVID-19 ‘brain fog’ inspires search for causes and treatments. Science. 2021 Apr 27;372(6540):329. doi:10.1126/science.abj2105.
Graphic Credit:
Graphic was downloaded from Shutterstock per their standard
agreement. The artist in this case had
many similar brain fog graphics and these depictions are probably an indication
of how common this term has become.
Here is an additional graphic that I complied as I did the literature search for this post:





