I recently posted an early view of an approach to look at the treatment planning discussion that occurs at the end of a psychiatric interview. I thought that the next step would be to see if this approach works in the real world. My current real world involves doing 1 hour evaluations with anywhere from 15-20 minutes of that time focused on a discussion of the treatment plan and that does include the option of no psychiatric treatment and in many cases other suggested treatments. For example, some people seek treatment for acute stressors including grief that generally resolve spontaneously or are more adequately treated by individual or group counseling. In most treatment settings where there is a triage system, these people are frequently screened out and do not see psychiatrists. That consideration directly applies to the treatment planning discussion because it affects the discussion of diagnosis, medical complications, and suggested treatments.
The graphic above shows the results of 10 interviews and the distribution of what was discussed (indicated by the orange cells) varies with individuals and general headings. The graphic is more readable if you click on it and zoom. For example there were 13 bullet points that were covered in all 10 discussions and those points have to do with a diagnosis and specific treatments are expected. Some topics were less frequently discussed and that generally means there were less applicable or the discussion time was reduced by a more lengthy diagnostic interview. I have found over the years that the length of an interview depends on getting the necessary transfer of information that can lead to a working diagnosis so that treatment planning can be started. The information necessary can be compromised by a number of factors including the patient's emotional state, their ability to describe a history with enough detail, the ability to be relatively concise, and the ability of the physician to communicate based on eliciting the necessary information and empathic listening. That can vary significantly from physician-patient dyad to dyad.
In terms of coverage of all 50 bullet points, 30-58% of them were covered in the discussions with patients. I don't think there is an ideal number. The people I talked with all have unique needs and there is no cookie cutter approach to either the diagnostic process of treatment planning. In some cases my discussion may run a little over the 15-20 minutes but that is rare. I have received some feedback that this seems like an ivory tower approach that can only be used by psychiatrists who have unlimited time with patients. All of these interviews were conducted the same way I have interviewed and talked with people for the past 30 years. The interview was not modified in any way. This is not research (yet) it is real world experience.
I am in the process of modifying the form based on suggestions from other psychiatrists so this is not the final version. At some point I think it would be useful to consider research using this kind of format to document that points covered by setting, diagnosis, and time constraints. A basic skill that all psychiatrists need is knowing when to depart from the original reason for consultation to a more urgent need - like the need for assessing an acute medical problems, a medical problem that might represent the cause of the psychiatric presentation, or a complication of treatment.
For now, I think it works as good evidence that psychiatry is not as easy as it has been depicted. The original depiction was by the federal government when it suggested the structure of psychiatric evaluations and treatment were not like the rest of medicine. There were separate codes and reimbursement for psychiatric treatment that did not take into account even one section of the above template. The adaptation to that government and insurance company practice has been to reduce discussions to the amount of time congruent with the devaluation of the cognitive process. That also led to clinics scheduling patients too close together and for briefer appointments. There is a lower limit to the time necessary to assess and treat patients. I don't think anyone who is doing new evaluations every 20 minutes while they are talking to patients and checking off templates in the electronic health record is going to be having lengthy treatment planning discussions. This form suggests that psychiatrists need time to do what they were trained to do.
The form when it is completed with provide not only a good estimate of what was discussed with the patient but will also provide guidance on what is relevant to document.
I do psychiatric interviews all week long. At this point
I’ve been doing it for over three decades. I am always interested in improving
the process. I came up with this idea recently and wish I had thought about it
many years ago. My standard initial interviews are anywhere from 45 minutes to
60 minutes long and that includes a lot of information transfer. The actual
amount of information transferred and whether it can be used come up with
formulation and diagnosis is always an unknown variable. There are people who
can come in and succinctly produce that information in 30 minutes or less.
Other people will take several hours. At the end of every interview, I have to
dictate a report that contains fairly standardized sections including a
diagnosis and treatment plan.
When physicians are trained there is an implicit
understanding that they will be able to adhere to a specific protocol and come
up with a diagnosis and treatment plan. In the real-world things are never that
linear. In inpatient psychiatry, the patient may not be able to produce a
coherent history or any history at all if they are severely ill and the
diagnosis needs to be pieced together by collateral information and the medical
and behavioral presentation. In outpatient clinics, the format is much
different. It is still possible to interview a patient who communicates low
information content but it is much more likely that patients describe what is
necessary for diagnosis and treatment. One of the main problems is the
discussion at the end of the assessment. It is typically truncated by time
constraints. Many patients leave the assessment and realize they should have
mentioned specific concerns or asked more questions.I often have people tell me that they are
drawing a blank in the interview and want to know if they can call me if they
have additional questions. I reassure them that they can.
These brief observations highlight the need for adequate
time and structure following the diagnostic interview to facilitate the
discussion and make sure that the patient can send and receive the
communication that is both necessary and what they want beyond that. I came up
with the structure over the past two weeks and I think is a good starting point.
I also refer interested readers to the only post on this blog that was not made
by me. It was written by Cedric Skillon, MD one of my psychiatric colleagues
because I observed his superior treatment planning in all of his notes that I
encountered.
This exercise assumes that any psychiatrist reading this as
adequate time to do their work. I don’t think psychiatry can be reduced to a
checklist and I don’t think it can be done in a short period of time. I realize
that there are psychiatrists reading this who may have evaluations
scheduled back to back in the morning and 15-minute appointments scheduled back
to back all afternoon. We all know how that schedule gets accommodated and the
outcomes are not good. What typically happens is there is very little emphasis
on getting to know and understand patients and little emphasis on communicating
with them about their problem. I also understand that the people who really
control all psychiatrist practice these days don’t really care about quality
treatment. The emphasis here is always on quality and the obvious fact that
quality work is not easy and it takes time.
What follows is my proposed outline for the patient
discussion. I think that in even moderately complex cases at least 25% of the
allotted time should be for this discussion. I have not done it yet but I hope
to hand an outline to the patient in order to facilitate discussion. I’m very
interested in whether their psychiatrist have used this technique and also
speculation on why it may or may not be a good idea.
1.A discussion of
the diagnosis and/or formulation
Of the people I talk with very few seem interested in the
specific diagnosis. It does happen, and when it does, I think it is important
to cover most likely diagnosis and complicating factors. For example, when
seeing a patient to has been drinking excessively for 20 years and gives a
history of anxiety and depression prior to the onset of that alcohol use and
current anxiety and depression can there be a valid anxiety or depression
diagnosis given the intervening alcohol use. This is a basic level of
complexity that psychiatrists encounter. In covering the diagnosis, I will
typically talk about a most likely diagnosis as well as the provisional or
working diagnosis and my recommendations for clarifying the diagnosis. In some
cases, people are interested in whether or not they have a severe psychiatric
disorder. I encounter a lot of people at the end of the initial interview who
asked me “So am I nuts/crazy Doc?” Some people have a specific diagnosis in
mind that they either want or don’t want and I give them my best assessment.
Some people have studied diagnostic features online or in the DSM and use that
jargon during my interview. They may or may not be right.
I think a formulation is always necessary in addition to a
psychiatric diagnosis. I was first impressed with rapid formulations done in
brief psychodynamic psychotherapy. I also found several courses given at the
annual APA conference in diagnostic formulations to be useful. The patient may
have their own formulation or one that they worked on with the therapist that I
would typically discuss in the original interview. I don’t think the
formulation discussion has to be excessive or detailed and it may complement
the diagnostic assessment. As example the case of the diagnosis of major
depression, it is reasonable to discuss the interpersonal elements relevant to
the depression as well as psychosocial stressors.
2.A discussion of a
no treatment option
A no treatment option should be explicit. It should be
discussed as part of the informed consent process. The potential risks and
benefits of no treatment should be discussed but in many cases no treatment is
a viable option for people. The case that always comes to my mind is the person
who consulted with me decades ago after receiving years long psychoanalytic
treatment who wanted to know if he should find a new therapist and continue.
After reviewing course of therapy and how his anxiety had improved over the years,
he was very relieved to hear from me that he probably did not need to continue
psychoanalysis. He had formally terminated with a psychoanalyst and no further
treatment was recommended but he wanted a second opinion from a psychiatrist.
Other people have mild anxiety and depression but are still functional and they
had concerns about both medication and psychotherapy. With psychotherapy - the time, financial commitment, and past therapy
experience are generally the determining factors. With medication the main concern
is side effects and typically concerns about taking any medication. I commonly
hear “Doc - I don’t like to take any medication, not even aspirin.” I think it is
possible to discuss no treatment in a number of scenarios as well as the
contingencies. The common contingency might be returning for reassessment if
symptoms worsen or there are other complications.
3.A discussion of
potential medical treatments and medical concerns – especially those that may
affect treatment
Outpatient psychiatrists are generally seeing patients
after all the smoke has cleared. If they have access to an electronic health
record (EHR) there are often laboratory results, ECGs, and imaging results and
reports that the patient may or may not be aware of. After taking a complete medical
history and review of systems I generally ask the patient if they had any
questions about recent medical procedures or results and we have a discussion
at that time.
The medical treatment of the identified disorder is
reviewed. There are often several approaches to the problem and when I discuss
all those approaches patients generally want my recommendation. I provide them
with that, the necessary prescribing literature, and both short and long-term
plans. I also talk about rare but serious complications of psychiatric
pharmacology like antidepressant withdrawal, agranulocytosis, Stevens Johnson
syndrome, priapism, serotonin syndrome, akathisia, suicidal ideation, and
neuroleptic malignant syndrome. In a previous post, I describe some of the
discussion. I generally want to make sure that the patient is aware of any
black box warnings, contraindications, and warnings. I will often do a drug
interaction search in front of the patient so that I can discuss it with them
rather than doing it after the interview.
In some cases, my treatment will depend on my discussion
with their primary care physician, cardiologist, or other specialist. It may
also depend on me ordering tests that I view as critical and getting those test
results.
4.A discussion of
potential psychotherapy treatments
There are research proven psychotherapies that should be
part of any informed consent discussion. I commonly inform patients with
posttraumatic stress disorder (PTSD) that exposure therapy and the EMDR variant
are very good approaches to the disorder and may be superior to
pharmacotherapy. That does not mean that I won’t try to treat that patient for
PTSD symptomatology, but I want to give them a clear message that the
psychotherapy results may be much better. I have similar discussions regarding
the psychotherapy of anxiety and depressive disorders specific to those
conditions. The psychotherapy may include supportive and crisis intervention approaches that occur right in the initial interview. In psychiatry treatment interventions that involve psychotherapy can occur right at the time of the assessment.
5.A discussion of
potential environmental/social approaches
One of the commonest problems in outpatient psychiatry is
that there are clear environmental factors that are leading to anxiety,
depression, insomnia, and substance use morbidity. Practically all of the
people in those situations or consulting psychiatrists are looking for a
medical treatment to address those environmental and social factors. I
generally have detailed discussion about the evidence that medication works in
those situations (there is very little) and what can be done. I typically discuss examples like grief responses and the very common scenario of a stressful work environment or boss. I want to be sure that I emphasize the point that medical treatment of these acute and chronic stressors is almost always not enough to solve the problem.
6.General treatment
parameters
If the patient and I decide to proceed with treatment – a discussion
of the general parameters of treatment needs to occur.That would include indications for calling me
and how to address potential medical and psychiatric emergencies.In this day of external control of medical
treatment – prescription refill policy can be discussed and how insurance
company denials or prescriptions (prior authorization) will be handled.In large systems of care, a discussion of who
has access to the information in the chart and systems that deal with emergency
and crisis calls can be a topic for discussion. In the current Internet age modes of communication (email, texts, calls) also need to be discussed especially if there is no formal EHR portal. Limitations on privacy are typically part of the general permission to treat but may require additional explanation like the CFR42 regulations for drug and alcohol treatment.
7.Definition of the
treatment alliance
As part of the general treatment discussion, definition the
treatment alliance can be useful for many people.Physical appearance and the appearance of one’s
office can be a projective test for people entering treatment.When I started out, I would get a lot of
comments like: “You seem to be too young to be a doctor!”.Now that I am an old man, my introduction has
stayed the same.Within a few minutes
people know how long I have been in practice.Most people can get past that and engage in a dialogue, but some people
are overly deferential and seem intimidated.Others decide to challenge the old man to see what he knows or if he can
be pushed around. Both of those scenarios can be a topic of discussion but that
might be too confrontive for most and lead to more problems in communication.A more neutral approach is to discuss the
typical diagnostic interview and treatment alliance. I find a basic definition that works for most people is: “You and I working on a problem or set of problems
that you identify to see if we can find the solutions.”
There have been entire books written on this topic, but
most don’t focus on the ten or 15 minutes at the end that should be for the
benefit of the person seeking help. That is my outline so far. Over the years I have had these discussions but not in a structured way. It de-emphasizes the diagnostic template or checklist and puts the emphasis on information that is directly useful for the patient. I plan to take
the headings, add bullet points, and see if it adds to the discussion. I think
it will because it will at least define the boundaries of the discussion, what
I hope to communicate, and provide more solutions to people coming in to see
me. And mostly I hope that it will counter the implicit assumption that all psychiatrists do is prescribe medications and that it is an easy thing to do.
George Dawson, MD, DFAPA
Supplementary 1: The preliminary form described above is contained in the 3 PNG files below. There are 49 bullet points so far. I have it as a Word file and a PDF so if you are interested in it send me an email and I will send you the format you want. I consider this to be a work in progress. Click on the files below to enlarge for easy reading.
Supplementary 2: As a preliminary screen - I looked at one day of intakes in my practice and discovered that I am routinely covering 30-36% of the bullet points on this form. That seems like a sufficient number but it would be a good idea to run a trial looking at the baseline for a number of clinicians (rated by independent observers) and then a second rating after the patients were provided the form ahead of time.
A couple of years ago I was driving up to Minnesota resort country when I noticed something happened at gas stations. For decades, gas pump choices were arranged linearly with the lowest octane fuel on the left and the highest on the right. The only difference was the occasional pump with diesel or racing fuel options and they were typically on the far right. To illustrate I took this photo of a gas pump display on the way home form work yesterday. Three years ago the display would have been (left to right) 87-88-91. In this case, in addition to the octane shuffle there is a price dissociation. Motorists have been trained for year to expect that 87 octane to be the least expensive and now it is not - 88 octane is the least expensive. These changes at the pump reminded me of a paper I had read a few years ago by Wolfram Schultz one of the world experts in reward prediction error.
Reward prediction error is basically the difference between a prediction about the nature of the reward and what really happens. See all of the definitions in the diagram below that are taken directly from Schultz. Reward is clearly defined as well as predictions to both the positive and negative sides.
In the paper of interest Dr. Schultz introduces it by being confronted with a vending machine where he cannot read the language (Japanese). There are 6 choices and his expectation is low that he will get his preferred choice so he pushes the second button. He is surprised that it delivers exactly what he wants - black current juice. He points out that this experience will keep him pressing this second button until the machine is loaded differently and he does not get his expected juice. He uses this as an example of positive reward prediction error (RPE) or the difference between his low expectation and the ideal outcome that resulted. RPE systems are set up to optimize positive reward prediction error. When the eventual negative outcome results in negative prediction error decision making will change in order to return to the positive RPE scenario and then no reward prediction error scenarios.
Getting back to the gas pumps. They appear to have been designed to defeat RPE at two levels. First, the position of the buttons after everyone was conditioned to push the one at the far left. The second, is the dissociation of gas price from button position. There is no longer a linear correlation between octane and price. I am not sure if both of these trends have been occurring over time or just recently. I do know from studying various gas pumps that the button positions do not necessarily reflect linear price or octane changes, but in some cases they still do. The good news is that they can both be overcome by carefully studying the octane button position and posted per gallon price rather than depending on the old learned patterns. The other interesting aspect of the gas pump problem is that there don't have to be a lot of predictions. The prediction error occurs only if the purchaser depends on old patterns without paying close attention to details.
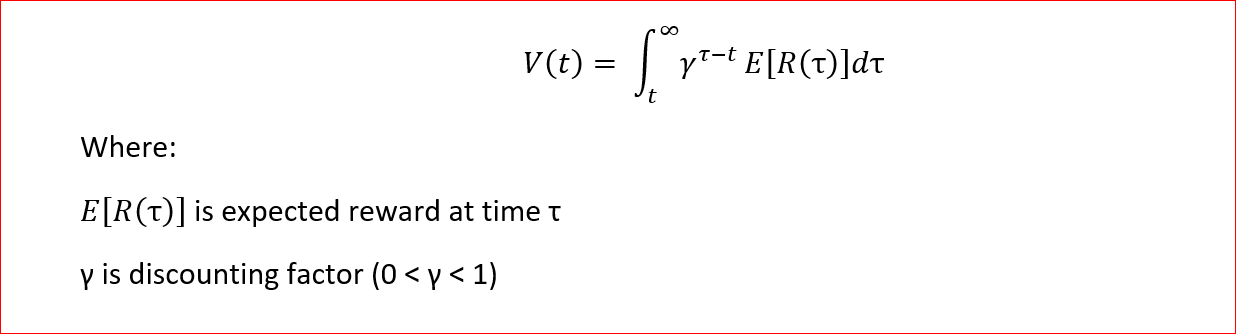
The neurobiology of RPE is more fascinating than the descriptive aspects. We know that the neurobiology of reward in the human brain is heavily dependent on dopaminergic systems in the ventral striatum. Dopaminergic neurons code reward in the form of prediction error even in complex tasks. What is even more interesting is that the coding is not in terms of quantifiable measures but subjective ones. Utility functions incorporate subjective measures and can be used to determine the potential values of the reward. Dopaminergic neurons code the utility of the received reward minus the utility of the predicted reward. Looking at a computational model of the addictive process, Redish (7) discusses a value function V[s(t)] dependent on the state of the world s(t) and presents it as the calculation of expected future reward discounted by the expected time of reward:
As noted the value of delayed rewards are reduced and the actual discounting applied is based on empirical work on discounting in human and animal models. The author in this case goes on to develop a computational model of addiction in this case that is based on reward prediction error and the fact that cocaine produces direct phasic increases in dopamine (DA). The model is termed a temporal-difference reinforcement learning (TDRL) model. According to RPE increases in DA occur after unexpected natural rewards. Over time DA release decreases, learning stops, and instead is paired with the cues for the reward. That does not occur with a pharmacological reaction at the level of the dopaminergic neurons. In that case, a drug like cocaine will release DA independent of the expected reward. That produces a final state where a unexpected natural reward, a cue for a learned reward, and cocaine will all produce DA.
The Redish paper also looks in detail at a couple of associated issues. The first is rational addiction theory defined as the user maximizing value or utility over time. Long term rewards for quitting are discounted more than the short term penalties and therefore the user remains addicted. In the author's model "the maximized function entails remaining addicted." (p 1946). TDRL theory suggests that addiction is always irrational because the pharmacological effects of cocaine (in this case) always outweigh the associated DA surges from the universe of value functions available in the real world. Addictive drugs will produce an increase in DA, so that the user will not be able to encounter and learn a value function that is associated with an equal or greater DA surge than is produced by the drug. Therefore the user remains addicted. This has been taught in addiction seminars for years as the Hijacked Brain Hypothesis - meaning that the dopamine signal produced by addictive drugs overwhelms the dopamine signal produced by natural stimuli like eating, drinking water, sexual behavior, and social affiliation. Both RPE and TDRL theory offer more explanatory power than the Hijacked Brain Hypothesis.
As I wrap up this post, I pulled down the latest editions of the two major addiction texts to see what they had to say about reward prediction error, computational models of addiction, and some of the authors referenced in this post, especially Wolfram Schultz. There were no references at all and the sections on the actual function of DA neurons in addiction was surprisingly thin. On the other hand a lot of concepts used in the field like salience are the direct product of these systems. In order to produce a more coherent picture of the neurobiology of addiction it is important to outline these DA systems and how they work normally and in addictive states.
I am hoping that addiction texts for clinicians will contain some of this information in the near future and ideally the chapters will be written by the scientists that have been studying these processes in some cases for decades.
George Dawson, MD, DFAPA
Supplementary 1:
Getting back to the gas pump example, considering the 3 octane ratings and the three prices that may or may not correspond to the octane ratings means that there are 6 possible combinations at any pump that need to be considered. Any real world actor at the pump needs to consider this carefully when the gas pump has undergone a transition from the expected correlation between increasing octane ratings and price to one where this relationship does not exist. The advantage to the actor in this case is that all of this information is explicit and that behavior is more likely to be affected by negative prediction error when automatic selection behavior results in the wrong octane or fuel cost being selected. That is unlike Dr. Schultz's example in the Japanese airport when he randomly chose a beverage and was unexpectedly rewarded. Supplementary 2:
I can't say enough about the writings of Wolfram Schultz. They are only peripherally mentioned in the addiction literature and yet his theories and experiments are some of the more important that I have read with regard to the neurobiological theories of addiction.
Papers of Wolfram Schultz - Journal of Neurophysiology Page Link
Home Page of Wolfram Schultz Link - contain some of the best PowerPoint slides that I have ever seen.
References:
1: Schultz W. Dopamine reward prediction error coding. Dialogues Clin Neurosci.2016 Mar;18(1):23-32. Review. PubMed PMID: 27069377 full text
2: Schultz W. Reward prediction error. Curr Biol. 2017 May 22;27(10):R369-R371.doi: 10.1016/j.cub.2017.02.064. PubMed PMID: 28535383 full text
3: Stauffer WR. The biological and behavioral computations that influence dopamine responses. Curr Opin Neurobiol. 2018 Apr;49:123-131. doi:
10.1016/j.conb.2018.02.005. Epub 2018 Mar 2. Review. PubMed PMID: 29505948. full text
4: Takahashi YK, Batchelor HM, Liu B, Khanna A, Morales M, Schoenbaum G. DopamineNeurons Respond to Errors in the Prediction of Sensory Features of Expected
Rewards. Neuron. 2017 Sep 13;95(6):1395-1405.e3. doi:
10.1016/j.neuron.2017.08.025. PubMed PMID: 28910622. full text
5: Keiflin R, Pribut HJ, Shah NB, Janak PH. Ventral Tegmental Dopamine Neurons Participate in Reward Identity Predictions. Curr Biol. 2019 Jan 7;29(1):93-103.e3. doi: 10.1016/j.cub.2018.11.050. Epub 2018 Dec 20. PubMed PMID: 30581025.
6: Tobler PN, Fiorillo CD, Schultz W. Adaptive coding of reward value by dopamine neurons. Science. 2005 Mar 11;307(5715):1642-5. PubMed PMID: 15761155.
7: Redish AD. Addiction as a computational process gone awry. Science. 2004 Dec10;306(5703):1944-7. PubMed PMID: 15591205.
8: Sweis BM, Thomas MJ, Redish AD. Beyond simple tests of value: measuring addiction as a heterogeneous disease of computation-specific valuation processes. Learn Mem. 2018 Aug 16;25(9):501-512. doi: 10.1101/lm.047795.118. Print 2018 Sep. PubMed PMID: 30115772.
When it comes
to solutions to the opioid epidemic - talk is cheap. The last 20 years
everybody has “the solution”. The AMA came up with a new version of theirs entitled “AMA Opioid Task
Force Recommendations for Policymakers.”
Inspection of this page shows that it is basically a rehash of
everything we have known over the past 10 years or longer. The only new message
is that the AMA is now suggesting that policymakers should follow these
recommendations. In this era of patient empowerment, direct advice to patients
is completely missing.
Drug
legalization advocates have apparently vilified the Reagan era “Just Say No”
campaign to the point that attempts at primary prevention of substance use are
now politically incorrect and forbidden. How can you possibly stop opioid and
methamphetamine epidemics when there is a large and vocal advocacy for
legalizing all drugs emboldened by the cannabis campaign? There are few reasonable voices out there saying “You know you can really live a better life
without drugs or alcohol”.
It should
probably come as no surprise that real action on the drug epidemic cannot be
expected from a government that is unable to end a decades long streak of mass
shootings. We hear the familiar refrain that people were “in the wrong place at
the wrong time” or that they are “fallen heroes” and that “now is the time to
move on”. A real adaptive response to mass shooting like even slightly tougher
gun laws would make a difference. Despite hearing that “this is the last time
that our children can be victimized” the mass shooting saga drags on - courtesy
of local and federal governments.
The resolution
of the opioid epidemic is another example of how our government doesn’t
work on serious public health issues. The epidemic has been in place for
the past 20 years. Using deaths by
overdose as a proxy measure suggests that things may be improving the last
couple of years, but the epidemic is far from resolved. The more recent problem has been that people
who started using prescription opioids have changed to heroin or fentanyl – the
supplies of both are plentiful and less expensive than the street value of typically
prescribed opioid pain tablets.
A few words
about the points the AMA has in their graphic:
1. MAT -
medication assisted treatment for opioid use disorder is considered a major
advance in treatment. That applies both to methadone maintenance treatment and
more recently buprenorphine maintenance with various preparations.
Sustained-release naltrexone injections are also an option but they are more
controversial due to the longer induction and wait time until the patient is
safely covered by opioid receptor antagonism. The current AMA position is to
remove prior authorization from these treatments so that they are more readily
available. Some treatments are more cost-effective than others. It is not clear
from the statement how the AMA hopes to remove these barriers particularly
since they have not been effective in removing them for the past 30 years of
utilization management or prior authorization. They may be counting on
political leverage in this case but I don’t see it happening. Regulators and
politicians could easily make this an exception to the current utilization
management and prior authorization statutes that they have on the books but it
should be apparent from that statement that they are the problem in the first
place.
2. Mental
health - the document cites the well-known correlation between mental illness
and substance use. The document also cites the Mental Health Parity
Addiction and Equity Act (MHPAEA) as meaningful but the only way this law
gets enforced is if civil action is brought against healthcare companies. These
healthcare companies are protected by legislation and they basically do
whatever they want. The AMA Task Force suggests that healthcare company should
be “held accountable” but that hasn’t happened in the 10 years since the MHPAEA
has been passed. The document suggests
that a number of addiction specialists should be in the networks of these
healthcare providers, but for 20 years politicians have been rationing mental
health services to the point that county jails are currently our largest
psychiatric institutions. The mental health suggestion in this document seems
like another wish.
3.Comprehensive pain care and
rehabilitation access - I would really like to see the numbers on this one. If
anything there has been a tremendous proliferation of freestanding or chains of
pain clinics over the past 20 years. That proliferation correlates directly
with increasing opioid prescriptions. As far as I can tell there has been no
movement at all in terms of determining what constitutes a quality pain clinic
versus something else. This may have to do with the politics that wrung the
word “quality” out of the healthcare system 30 years ago. There is also an
access problem. In other words there has always been “non-opioid alternatives”
like physical therapy but healthcare systems ration their utilization. This might be another area where education is
important and convincing people that a course of physical therapy even if their healthcare company makes them pay for it is potentially more beneficial than
taking opioids and getting deconditioned for a period of time.
4. Maternal and child health - there is no doubt
that punishment-based paradigms can intrude on the parental relationships with
children and result in destabilization of families. This usually occurs on a
county by county basis and there are no statewide standards and no specific
treatment facilities. The problem is compounded by the fact that most states
consider social services to be as expendable as mental health services and it
takes more than a suggestion to reverse that 20-year trend. Recently, the child protection issue as a result of substance use has become so bad that additional tax legislation is needed just to cover this problem.
5. Civil and
criminal justice reforms - the most significant reform suggested in this
section is that MAT is continued when a person is incarcerated and after they
are released. This is a tall order considering how difficult it is for anyone
to access MAT in an outpatient setting. Jails and prisons have the absolute
worst record. The evidence for that is people who are acutely taken off of
methadone, buprenorphine, or other psychiatric medications at the time of
incarceration. That can lead to weeks of opioid withdrawal symptoms and intense
physical symptoms. Despite many county
jails considering themselves to be psychiatric hospitals very few of these
places are equipped to assess and treat psychiatric disorders or do medication
assisted treatment of substance use disorders.
That is the AMA
WishList and all of its deficiencies. I have not seen a realistic assessment of
the problem and how to reverse it in spite of the fact that there are two
documented opioid epidemics in the medical literature and suggestions about how
they were resolved. I never heard anyone referencing them. Medication assisted
treatment was one component but there are other significant factors that no one
seems to be talking about at this time.
Working in a
residential treatment facility provides me with unique perspective on the
problem. The continuum of care ranging from residential treatment to intensive
outpatient treatment to date treatment to self-help groups like Alcoholics
Anonymous and Narcotics Anonymous depends on a number of factors to make it
work. First and foremost is a competent staff in the facility with reasonable
boundaries and a supportive environment. Most medical facilities do not have
this because of significant bias against people with substance use disorders.
There are some treatment facilities that have similar biases and they should
not be allowed to admit people until that problem is resolved. The measures
recommended by the AMA Task Force are medically weighted and that means that
treatment facilities need to have medical staff. If the facility needs
histories and physicals done medical staff need to provide that function as
well as comprehensive detoxification, treating associated medical problems, and
providing psychiatric care and MAT. There is no point in having residential or
outpatient treatment programs in a network if they cannot provide that level of
care. People who need MAT should not be treated in facilities where they cannot
get medical assessment and treatment.
That basic fact
seems to be missing from the AMA Task Force guidelines, state regulations, and
any discussion at the federal level about what kind of treatment is needed for
people with active opioid use disorders.
The AMA could
be of more service referring people to appropriately staffed treatment programs
and advising the public on the source of all of these obstacles of care. As I
have been writing here for years now those obstacles are a product of pro-business
government policy at both the state and federal level and how those rationing
businesses are able to operate. Until that basic flaw is corrected - I do not
anticipate any increase in access to treatment (at least effective treatment),
increased access to appropriate social services, or sudden revision of county
jails to suddenly make them functional psychiatric units.
There are some changes that would make an immediate difference in the opioid epidemic instead of the continued evidence-based platitudes. If there are any policy makers or politicians out here that are serious about making some changes - here they are:
1: Hold physicians harmless for providing MAT:
The suggestion that more physicians should be providing MAT for opioid use disorder has gone from a suggestion to more of a demand. Just this weekend there have been debates about why Emergency Department Physicians aren't providing MAT for every person with OUD that they see. My first thought when I saw that was: "Are they serious?" People are not presenting to EDs with casual use. They are not people coming into clinic intentionally in withdrawal to start buprenorphine induction. They are generally people with very serious use problems who end up in EDs because of a different problem. Many of them are polysubstance users with multiple drugs on board and in many cases drugs that are typically flagged as having potentially serious interactions with buprenorphine. Add to that the dearth of buprenorphine prescribers that will accept referrals from an ED and it makes perfect sense that Emergency Medicine physicians do not want to send people out with buprenorphine.
The physicians are not the problem, the practice environment is. The solutions seem obvious to me. The first is to indemnify the physicians for providing care that is harm reduction to patients with high risk. This already happens in state statutes that cover Good Samaritan provisions, mandatory reporting of child and adult protection concerns, and civil commitment and guardianship proceedings that hold the petitioners harmless for good faith activity. MAT is a very similar endeavor. But I would not just stop at a vague statutory requirement. I would tie it in with abbreviated training for MAT. When I took that training, at least half of the patient case examples were high risk with limited resources, psychiatric comorbidity, and they were using high levels of multiple substances. The answer in each of these scenarios was to prescribe buprenorphine as a way to assist the patient with the OUD aspect of the problem.
2: Open up addiction clinics:
The idea that primary care physicians are all going to start seeing large volumes of these patients will not materialize as long as there is a problem with cross coverage. I have seen it happen many times. A well intended physician starts prescribing buprenorphine and even in a mutli-specialty clinic has nobody else to assist and is on-call 24/7 for years until they burn out. There has to be a structure in place where there are clinics that can handle large volumes of patients including the referrals from all of the local EDs and correctional facilities and provide adequate cross coverage for the physicians prescribing buprenorphine.
3: Decrease the training requirement:
Unlike others - I don't think it can be eliminated for the reason I cited above. The physicians and other prescribers need to know the high risk scenarios that they can treat. I think it could probably be done in two hours with a case book of treatment scenarios. The case can be made for collaborative care/mentoring arrangements with experienced physicians, but the funding of those scenarios should be seriously considered.
4: Provide temporary housing programs to take people directly from the ED and crisis appointments:
As a former acute care psychiatrist - I know the uneasy feeling of providing brief opioid detox services and discharging patients with OUD to the street with medications that have street value. There is no surer path to immediate relapse. If we are really serious about helping people get established on MAT, they need a stable environment where it can happen.
5: States need to license substance use programs only if they provide medical services and MAT:
If we are all serious about the effects of MAT in OUD it is time to start acting like it. There is no longer an excuse or reason for not offering MAT to all patients in residential, extended care, or outpatient treatment programs. There are no religious or ideological grounds that justify not offering these services and the license of all treatment facilities should depend on it.
These are my ideas about stopping the opioid epidemic that stop all of the platitudes in their tracks. There is a rational way to proceed that does not depend on physicians sacrificing to keep the irrational system afloat. The rational way will cost money, but it will also save money but not in the way politicians usually talk about healthcare savings. It will save money and resources by saving lives, not investing in inadequate treatment, and finally putting a dent in the large circulating pool of opioid and polysubstance users that are circulating between emergency departments, inpatient units, drug treatment programs without MAT, detox units, shelters, and jails.
The political aspects of medical cannabis are
undeniable. The legalization of cannabis for recreational purposes had no
traction with American politicians or voters until it was promoted as a miracle
drug. With that widespread promotion medical
cannabis is now legal in 33 states and recreational cannabis is legal in ten. The legalization arguments also suggested
that the US was behind other countries of the world when there are only two
countries – Canada and Uruguay – where it is completely legal for medical or
recreational sale and purchase. In the
world, 22 of 195 countries have legalized medical cannabis with widely varying
restrictions on its use. The Netherlands is often cited as an example of
recreational cannabis use, but most Americans don’t realize that it is illegal
for recreational use and tolerated for use and sale only in specially licensed
coffee shops. The promotion of cannabis
as a solution to the opioid overuse and chronic pain problems can be seen as an
extension of the political arguments for legalization that outpace any science
to back them up.
There was probably no greater hype about the purported
benefits of medical cannabis than early data suggesting that it might decrease
the rate of opioid overdoses (1). The sequence of events was supposed to be
opioid users tapering off of opioids or using lower equivalent amounts because of
medical cannabis use. The original study
covered the time period from 1999-2010 and suggested that states with medical
cannabis laws had a lower mean opioid overdose mortality and that the annual
rates of overdose progressively decreased over time. The authors conclusion was: “Medical cannabis laws are associated with
significantly lower state-level opioid overdose mortality rates.”
Despite the usual caveats suggested by the authors
in the original study the results of that study were heavily hyped by all
cannabis promoters as was the discussion of many Internet forums. The lay press, public, and politicians saw it
as another reason to promote medical cannabis and recreational cannabis by association.
A study came out today in PNAS (2), that is an
extension of the original data and it no longer comes to the same
conclusion. In this new study the
authors replicated the opioid mortality estimates from the original study but
when the data was extended from 2010 to 2017 – the improved opioid overdose mortality rates not
only did not stay constant but they reversed themselves to that they were now
on the average from -21% to +23%. They
provide an even more valuable analysis of this effect as spurious rather than a
true positive or negative effect based on the low penetration of medical
cannabis in the population at large (2.5%). The
authors focus on the problem of ecological fallacy – that is conclusions about
individuals are drawn from aggregate data across the entire population.They point out that the states with the medical cannabis laws have a number of characteristics separating them from other states. A recent good example of this
fallacy was the New England Journal of Medicine (3,4) report that per capita
chocolate consumption correlated with the number of Nobel Laureates in a particular country.
This is a valuable lesson in scientific
analysis. The political approach to the problem is all that most of the public
sees. That approach is to grab any information that seems to agree with your
viewpoint and run with it. Big Cannabis
and cannabis promoters have been doing this for almost 20 years now. The process
of science on the other hand is slower and more deliberate. It is not a question of a right answer but a
dialogue that hopefully produces the right pathway. The authors of this study
have added a lot to the dialogue about cannabis but also statistics and how statistical
descriptions may not be what they seem to be.
George Dawson, MD, DFAPA
References: 1: Bachhuber MA, Saloner B, Cunningham CO, Barry CL. Medical Cannabis Laws and Opioid Analgesic Overdose Mortality in the United States, 1999-2010. JAMA Intern Med. 2014;174(10):1668–1673. doi:10.1001/jamainternmed.2014.4005 (full text) 2: Shover CL, Davis CS, Gordon SC, Humphreys K. Association between medical cannabis laws and opioid overdose mortality has reversed over time. First published June 10, 2019 https://doi.org/10.1073/pnas.1903434116 (full text) 3: Messerli FH. Chocolate consumption, cognitive function, and Nobel laureates. NEngl J Med. 2012 Oct 18;367(16):1562-4. doi: 10.1056/NEJMon1211064. Epub 2012 Oct
10. PubMed PMID: 23050509.
4: Pierre Maurage, Alexandre Heeren, Mauro Pesenti, Does Chocolate Consumption Really Boost Nobel Award Chances? The Peril of Over-Interpreting Correlations in Health Studies, The Journal of Nutrition, Volume 143, Issue 6, June 2013, Pages 931–933, https://doi.org/10.3945/jn.113.174813
Attribution: Above figure is from the original article (reference 2): "This open access article is distributed under Creative Commons Attribution-Non Commercial No Derivatives License 4.0 (CC BY-NC-ND).y" See this link for full conditions of this license.
Venlafaxine is a commonly prescribed second-generation
antidepressant. It is well-known to psychiatrists because it is a second line
medication if SSRIs fail and for many psychiatrists it is another first-line
antidepressant. In some head-to-head comparisons with SSRIs venlafaxine has a
more favorable side effect profile. It does have the risk of discontinuation
symptoms and typical antidepressant side effects. I have noticed that the dose
escalation with venlafaxine seems to be out of proportion with SSRIs, bupropion,
and third-generation antidepressants.
Consider the following venlafaxine related scenarios:
1. A colleague comes into my office late in the day and
asks me: “Have you ever heard of venlafaxine causing sedation at higher doses?”
The patient in question was just increased from 187.5 mg to 225 mg - the
suggested max dose according to the FDA approved package insert.
2. I am asked to consult on patient who had extensive
pharmacogenomic testing in a different facility where she was told that she may
need to take 350 to 450 mg of venlafaxine per day based on that genetic
profile. She wants to make sure that she gets an adequate dose of the
antidepressant and is currently on 225 mg.
I reviewed the limitations of that approach with the patient and
potential side effects and I let her know that the commonest side effect I see
in people taking high-dose venlafaxine is excessive sedation or low energy in
the daytime. As we start to follow the recommended dose increase she discloses
that she has had sedation even at the 225 mg level. We decreased the dose to
150 mg and that side effect is gone. Her
depression is also gone.
3. I see a significant number of patients taking more than
300 mg per day of venlafaxine from the same geographic location in the United
States. They all tell me that the target dose in that location is 350 mg per
day and they are all experiencing numerous side effects. Many had dose
escalations into that range in a week or two - much faster than any increase I
have done.
What is wrong with this picture? Why are there a significant
number of people taking more than the recommended dose of venlafaxine in some
cases much more and appearing to have side effects? The roots of this prescribing behavior can be traced back to
old-school psychopharmacology. Proponents of that approach suggests that there
may always be a group of outliers that need to take higher-than-expected doses
of medications - typically antidepressants but there has also been a history of
excessive dosing of antipsychotic medications. People were generally more
cautious with more toxic medications like tricyclic antidepressants, monoamine
oxidase inhibitors, lithium, and various addictive compounds. They also seem to
be more cautious with SSRI type medications at least initially. It took over a
decade for me to see a dose of sertraline in excess of the maximum recommended
dose. While it is true that there are always outliers in terms of dose-response what is the best way to approach that problem.
I have attended medical education
courses where the lecturer suggested titrating the medication to the point of
toxicity and then reducing it back down to the next lowest dose. That
particular lecture was focused on treating anxiety disorders with SSRIs. I don’t
think that is the best approach. The best approach to me is one where the
patient recovers from anxiety or depression and the process does not experience
a single side effect. I know that can be done because I have been doing it for
decades.
That also brings me to what I think is a good research article that looks at optimal dosage ranges. It is a very large
meta-analysis of fixed dose randomized clinical trials that utilize the
specific antidepressants - citalopram, escitalopram, fluoxetine, paroxetine,
sertraline, venlafaxine, and mirtazapine.
The trials were identified by searching the literature and looking for
unpublished studies specifically by searching national drug licensing agencies
and requests directly to pharmaceutical manufacturers. Outcomes were noted at
eight weeks of treatment and defined as a 50% reduction on an observer rated
scale for depression. Dose equivalence
among medications was determined from previous studies and the recommendations
of the manufacturer. The article is written by researchers that I consider to be world experts in meta-analyses and the analysis of large data sets in psychiatry.
77 studies were identified from a total of 24,524 published
references and 4030 unpublished records.
27 were published, 21 or unpublished, and 29 were both published and
unpublished. The study showed too hard when treatment groups across all of the
medications of interest between the years 1986 and 2013.
The authors calculated dose response, dropouts due to adverse effects, and dropouts for any reason. Relative risks (RRs) were calculated for
specific doses. The dose outcome relationships for venlafaxine are included in
the figures below from the original article.
The Response figure shows the significant increase of up to about 150 mg
and then a much more modest increase beyond that. The Dropout figure shows a
similar increase up to the 150 mg range. The Dropout for any reason was less
remarkable. The authors calculated that the 75-150 mg dose of venlafaxine was equivalent to 20
to 40 mg of fluoxetine (click to enlarge graphic)
The authors conclude that optimal acceptability of SSRIs
and venlafaxine and and mirtazapine occurs within the lower end of the licensed
dose range. They reconcile this with serotonin transporter (SERT) studies that
show that 80% SERT occupancy occurs at the minimum doses of SSRIs or
venlafaxine with further dose increases showing small increase in SERT
occupancy.
In the case of venlafaxine they suggest that noradrenalin
reuptake transporter (NET) may require higher doses of venlafaxine in the 225
mg to 375 mg per day range. Given the lack of efficacy of atomoxetine, a logical
question might be whether NET blockade adds much to the antidepressant effect.
The authors review other dose-efficacy studies of
antidepressants and point out that they are variable. The variability ranges
from optimal doses of fluoxetine in the 21-40 mg per day range to doses at the
recommended lower end of the range being superior. Response to doses in the
higher range were variable in some studies. One study found a significant
greater response for high-dose antidepressants but the dose of 40-50 mg
fluoxetine equivalents showed the greatest efficacy.
The authors considered strengths and limitations their
study. They thought that their state-of-the-art meta-analysis was a strength as
well as the size of the data set. They also examined dose dependency for both
efficacy and tolerability and acceptability. The limitations they
discussed included patient selection and dosing not reflecting clinical practice. They
also discussed the calculation of dose equivalency among antidepressants and
how that might be problematic.
Another obvious strength of this study is the calculation
of relative risks for response across SSRIs, venlafaxine, and mirtazapine. The
figures are modest but favor antidepressants across all dosage ranges with the
exception of mirtazapine at the 60 mg dose.
The authors don’t seem to mention it but it would seem that the optimal
dosage ranges could be predicted from the regulatory information since that is
based on dose ranging studies and tolerability studies. In that regard, the
conclusion about dose ranges don’t seem to be that surprising but they may be
needed given what is happening clinically.
Getting back to the issue with venlafaxine I see people
respond to dosing within the lower and of the range from 37.5 to 75 mg in many
cases. That same response rate continues up to the 150 mg dose and then starts
to diminish between two or 25 and 375 mg. Over that same range there is a
significant increase in dropout rates due to adverse effects.
How clinicians approach this new information will be
interesting. There will still be people like me and the conservative camp
looking for the first signs of side effects and toxicity and deciding at that
point whether to stop dose escalation. I explicitly tell people that the goal
is not to experience any side effects and that I doubt that people “get used to”
side effects. There are clearly clinicians out there who are
doing exactly the opposite and that is increasing the dose of venlafaxine and
advising people to either tolerate the side effects or expect that they will go
away.
The balance between therapeutic effect and side effects is
a central issue in all branches of medicine. In many cases, the severity of
adverse effects like an allergic reaction determines the decision. In the case
of the medication like venlafaxine making that decision can be complex. Some of
the side effects like sedation and lethargy at high doses can mimic symptoms of
depression. At this point in time neither pharmacogenomics or most plasma level determinations guarantees either tolerability or
efficacy. Detailed analysis of the
situation by an expert with a bias toward preventing side effects is required as the first step in any dose increase.
George Dawson, MD, DFAPA
References:
1: Furukawa TA, Cipriani A, Cowen PJ, Leucht S, Egger M, Salanti G. Optimal dose of selective serotonin reuptake inhibitors, venlafaxine, and mirtazapine in major depression: a systematic review and dose-response meta-analysis. Published:June 06, 2019DOI: https://doi.org/10.1016/S2215-0366(19)30217-2.
After a protracted discussion on the previous post, I thought I would go down to the University of Minnesota Biomed library today and look at the drug ads in psychiatric journals at about the time Prozac came out in 1987. I was interested in the trends before and after so I picked the years 1985 to 1995. I also picked the journals the American Journal of Psychiatry, Archives of General Psychiatry (currently JAMA Psychiatry), and the Journal of Clinical Psychiatry. I was going to include JAMA and the New England Journal of Medicine. They had about the same number of ads but none of them in that year contained ads for psychiatric medications.
This kind of search is labor intensive these days. There was a time on the early days of the Internet when entire journals with all of the ads were scanned in. As a subscriber I could have run that search from home. These days, all of the ads are gone and the references are saved as text files only. In order to see historical ads - the hard copy of the original journal needs to be examined. Even then there are some problems. I encountered some bound volumes where the ads were physically removed. There were two to three bound volumes per year and additional copies of the NEJM and JAMA - I may have looked at 75 bound volumesover 4 hours.
In many ways it was a walk down memory lane. Clozaril and Haldol Decanoate ads were especially heavy in the early 1990s. There were ads for medications that I prescribed all of the time like Navane and Pamelor and ads for drugs that I seldom prescribed like Stelazine, Serzone and Luvox. There were ads for new drugs that I would prescribe once like Paxil. It was a reminder that despite all of the advertising - a lot of drugs end up never being prescribed by physicians. My reason for being there was to look for the origins of the term "chemical imbalance" in this advertising.
I decided to embark on this project because of all of the inaccuracy about the term, especially the tendency to blame psychiatrists for it. In my previous post, I attempted to point out that it is a fairly straightforward process to conclude that the human brain does not run on chemical imbalances - just based on the average scientific knowledge of physicians. On the advertising side, I was there for the first National Depression Screening Day in 1990 and that was the first time I heard the term. The event has been criticized as a venue for allowing a pharmaceutical company to showcase their product. I participated in the event for 3 years and the advertising involved was much more subtle than is found today at NAMI walks for example. But the question is whether the advertising meme "chemical imbalance" was introduced at that time. Any event that happened 30 years ago is very hard to track. As the Public Affairs Rep for my District Branch of the APA, I had a lot of files about it that I subsequently trashed. I am guessing there were also some files on disk drives that would have been helpful. This is a reconstruction without that data.
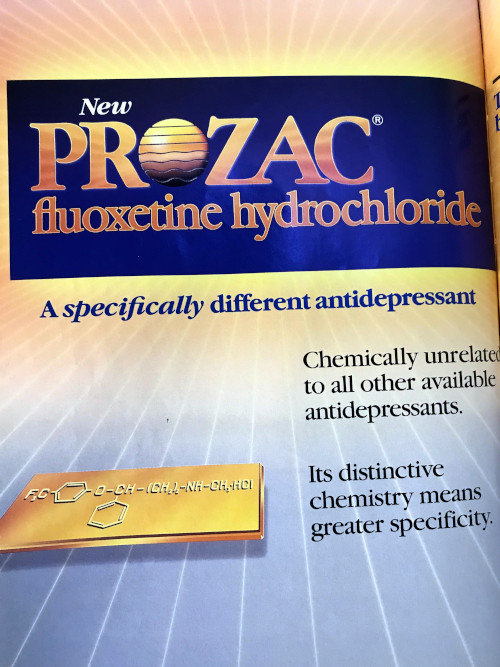
I successfully located the first Prozac ad in AJP from 1988. The graphics are all iPhone photos so there is some distortion. Chemistry is emphasized on page one as in the chemical structure, chemically unrelated to other antidepressants, distinctive chemistry, and the first highly specific and highly potent blocker of serotonin reuptake.
Why is this important? At the time most of the antidepressants being used were tricyclic antidepressants. They could not claim any specificity and in subsequent ads manufacturers start to compare possible side effects based on transporter monoamine protein and receptor affinities. The Prozac molecule was being hyped as being chemically unique and with a better side effect profile. As Prozac started to sell more it became a blockbuster drug for Eli Lilly and at that point the manufacturers of other new antidepressants noted and the competition heated up. There were some direct references to Prozac in the ads from competitors.
The best example is this Wellbutrin ad from AJP in 1991. Prozac is directly mentioned in the ad and reasons are given for choosing Wellbutrin over Prozac. Being non-serotonergic is one of them and this is more of a counter to Prozac advertising as being a unique first highly selective serotonergic drug. It gives little or no weight gain as a reason, but at the time I was seeing obese patients who were taking 80 mg of Prozac because their primary care physicians told them they could lose weight taking it. Of the other bullet points it seems that lack of sexual dysfunction would be the most relevant. The marketing decision in this case was a conscious decision to go after the purported serotonergic effects of Prozac rather discuss the hypothetical mechanism of Wellbutrin. The side effect of Wellbutrin that most physicians are concerned about - seizures - is in the smaller print below the bullet points.
Effexor came up with similar ads. In the late 1980s and early 1990s, synaptosome technology was invented to look at binding affinities of central nervous system medications to specific receptor sites. The quantitative aspects of these studies were generally globalized in the psychiatric literature to qualitative ballpark effects. For example a plus or minus grading system could be used ranging from no effect at a receptor (-) to a robust effect (++++). Effexor advertising used this to compare side effect profiles among the competitive antidepressants at the time.
This ad emphasizes that Effexor is "a structurally novel antidepressant and is chemically unrelated to any other available antidepressant." It shows the table with comparisons to tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) and what might be predicted based on the in vitro synaptosome data with the qualifier that the clinical significance of that data is unknown. Clinically most people are able to tolerate all three classes of medication but some will not. The differences can't be predicted on the basis of the receptor binding studies because of receptor heterogeneity and differences in drug metabolism. For example, I still prescribe TCAs. It is nortriptyline and it is the only one I have ever prescribed. At the doses I prescribe and per the table in the ad - it is as well tolerated as SSRIs and SNRIs (Effexor). The ad appeared in the AJP in April of 1994. On that basis the argument could be made that it is an appeal to the technical expertise of psychiatrists and it should contain this information. That also points to a weakness in my informal advertising study and that is a lack of ads from the non-technical consumer literature from the same period. (see supplementary on a proposal).
I have 30 additional ads from the journals but the themes are roughly the same. An emphasis on medicinal chemistry and the suggestions that some chemistry is better than others. Interestingly, in my previous post the whole point was that this is the kind of argument that would not fly based on what the average physician knows about chemistry and molecular biology. Psychiatrists should know a lot more because the evidence for and against these theories had been reviewed in the psychiatric literature 20 years before these ads came out (1974-2002) (1). And they are engaged in clinical practice and need to be skeptical of newly introduced products and claims.
What I did find so far is unequivocal evidence that the chemical imbalance meme was used to directly market antidepressants to the public. The Zoloft ad embedded at the top of this page from 2001 is the first example. The second example is this Paxil ad from the same year.
That is what I have so far. See the Supplementary below to find out what you can do to complete the story. I don't have a problem with people telling me that their doctor told them that they have a chemical imbalance and their antidepressant is supposed to treat that. I don't have a problem with people saying that their psychiatrist told them that. I do have a problem with people saying that all or even most psychiatrists say this and that psychiatrists are behind this meme.
There is an exaggerated focus on the mechanism of action of medications used for psychiatric indications. I have never heard anyone say their doctor told them about the mechanism of action of antibiotics or even their blood pressure medications. In the case of antibiotics it is clear that people demand them and they don't care what the risks or mechanisms are. This advertising campaign may have something to do with the conversion of folk psychologists to folk psychopharmacologists. A friend of mine also brought up an important aspect of this campaign that is also addressed by these manufacturers and that is legitimacy. For decades people with depression and anxiety were viewed as weak people with a questionable problem. My friend told me that these ads confirmed that she had a serious problem that needed a serious solution and that it was finally acceptable to talk about it. Say whatever you want about Big Pharma advertising but it apparently carried the message that current "Let's Talk About Mental Health" programs do - but over 15 years ago.
The attribution of an advertising meme to psychiatry and psychiatrists despite the fact it has never appeared in 30 years of psychopharmacology texts is not a trivial fact. The advertising videos posted here were viewed by tens of millions of people. I hope to get more information and still have some people to contact. With any luck I will be able to fill in the additional data between the release date of Prozac in 1987 and the ads posted here from 2001.
Please send me anything you might have from those dates.
George Dawson, MD, DFAPA
References:
1. Nathan KI, Schatzberg AF. Mood disorders. in Review of Psychiatry, vol 13. American Psychiatric Press, Washington DC(1994): p.171-184 Supplementary 1:
From the information I posted above it is clear that chemical imbalance was an advertising meme introduced during the height of competition of blockbuster antidepressant drugs. The common Wall Street definition of a blockbuster pharmaceutical is a product that generates sales of a billion dollars a year. There are two important pieces of data that would be useful to complete the story.
The first is earlier ads with the term chemical imbalance. So far, I have two from 2001, but I am certain it appeared before that. I don't have time to search all of the popular literature. If you subscribe to a magazine that has pharmaceutical advertising and keep all of the old volumes - take a look at the editions from about 1987 to 1995. If you see the term chemical imbalance please send me the image with the name and date of the periodical. Let me know if you want credit for finding the image and I will give you full credit.
If you are a current or former pharmaceutical rep or marketing person and have access to any documents or videos with the chemical imbalance phrase please send it to me with the date it was being used. If you have recollections of how it was implemented and when I can also use that information but I am most interested in clear documentation like the videos I have posted. I have no interest in vilifying the pharmaceutical industry and understand the need for marketing and advertising. I am just interested in the origins of this term and how it was implemented.
If you are an APA member and you were involved in the original National Depression Screening Day in 1990 - you may also have some information about this. Please send it to me.
Thanks!
Supplementary 2:
All of the name brand drugs/medications mentioned in this post are currently generics or are no longer manufactured. I have no affiliation with the original manufacturers or the generic drug industry.
Supplementary 3:
There are various Internet sites that attribute the term chemical imbalance to Pfizer or Lilly but they do not appear to be reliable - many appear to be antipsychiatry sites. I would like to hear from people who were there at the time and can provide the necessary proof. In those days (1986-1996) it would have been an internal memo or presentation. Send me a copy if you have it.
Supplementary 4:
I had the opportunity to discuss this issue with a corporate attorney - especially the issue of available emails and memoranda dating back to 1987. He told me that corporations hold this data only as long as the law states they needs to. For example, if the law states the data must be held for 4 years it will be held exactly that long and then everything will be shredded. If this information exists it will probably be in private hands.
Supplementary 5:
I got the expected low level feedback from a Twitter poster who thought he was making some point about this link on the Royal College of Psychiatrists web site suggesting that at least one of the causes of schizoaffective disorder was "a chemical imbalance". I guess he really thought he had made me look foolish especially with the proclamation "You aren't psychiatry - they are."
In fact, I can't tell who wrote this and whether or not it is a psychiatrist. I don't know what the RCP official position is. I was happy to see that they are much more flexible than the anti-psychiatry Twitter posters I encounter. There was a feedback form that I completed and advised them to lose the "chemical imbalance" and that replacing it with "unknown etiology" was preferable. What I would like to see is an exposition of the latest theories and a suggestion that the critics actually read psychiatric literature. They would be less likely to perseverate the same criticism they have used for year after year. This poster also seemed to ignore the fact that the RCP public information was posted in 2015 - that's 14 years after the television ad posted at the top of this page. Royal College of Psychiatrists - the ball is in your court.
Supplementary 6: (added on 1/11/2020): I just learned today from an advertising expert in antidepressants that there was also a Zoloft ad from 2004 that used the term:
"While the cause is unknown, Zoloft can help. It works to correct a chemical imbalance in the brain that may be related to these symptoms."
Reference:
Cristina Hanganu-Bresch. Treat Her with Prozac: Four Decades of Direct-to-Physician Antidepressant Advertising in Drugs Media: New Perspectives on Communication, Consumption, and Consciousness (Hardback) (1st Edition) by Robert C. Macdougall (Editor), Drugs &. Media-Pasta Dura, 340 Pages, Published 2011 ISBN-10: 1-4411-1988-4 / 1441119884 ISBN-13: 978-1-4411-1988-9 / 9781441119889: