 |
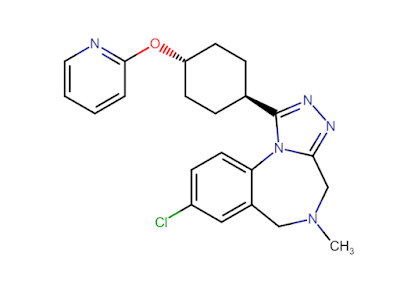
| Balovaptan (RG7314) |
Autism is a difficult to treat disorder, especially in the case where it is associated with aggression. As the patient ages, physical redirection and behavioral approaches can not be effective. In that case, the patient's living situation can be placed at risk. As an inpatient psychiatrist, I would frequently see patients admitted to my inpatient unit who had been living at home until their parents could not longer provide the necessary care. The expectation was that the inpatient stay would help with that transition. Care of the older person with autism and aggression is further complicated by a nearly complete lack of public resources in terms of stable living environments with staff present to assist with behavioral problems.
The only medications that have been FDA approved to treat autism are risperidone - the first approved atypical antipsychotic medication in the USA and aripiprazole. Antipsychotics can exert an anti-aggression effect in the case where aggression is part of schizophrenia and bipolar disorder. It is also used as an off label indication for treating aggressive symptoms in personality disorders and autism. One of the main studies in autism was done by McCracken, et al (1) and published in 2002. That study showed a significant improvement in irritability, aggression, and self injury in the treatment group relative to the control group. In the study irritability as measured by that subscale on the Aberrant Behavior Checklist was significantly improved in 69% of the treated group and that improvement was maintained at 6 months. The mean daily dose of risperidone was 1.8±0.7 mg to a group with a mean age of 8.8±2.7 years. By comparison, the lowest effective dose in adults is 6 mg with typical range of 2-5 mg for most conditions.
The limitations of atypical antipsychotic therapy are well known and they were observed in this group of children over the course of the course of the 8 week study. They included increased appetite, a weight gain of 2.7±2.9 kg, and drowsiness. Of the neurological symptoms anticipated with this class of drug including akathisia, tremor, dyskinesia, rigidity, and difficulty swallowing - only the tremor was more frequently observed in the risperidone treated group relative to placebo. The rate of withdrawal from the study was 5 times higher in the placebo treated group. The authors concluded that within the limits of their study design that risperidone was safe and effective for the treatment of tantrums, aggression, and self injury. The
FDA package insert for risperidone was modified to include the indication:
Treatment of irritability associated with autistic disorder in children and
adolescents aged 5-16 years. FDA approval for risperidone was in 2006 followed by FDA approval for aripiprazole in 2009. The wording in the
package insert is slightly different under the indications section for aripiprazole:
Irritability Associated with Autistic Disorder. Although I don't have any actual data, clinical use in adults suggests that aripiprazole would be the most prescribed agent for autism because it is generally seen as having a more favorable side effect profile.
The putative effects of psychiatric medications are generally extrapolated from know receptor affinities and atypical antipsychotics are generally dopamine receptor (D2) and serotonin receptor (5HT2) antagonists. Aripiprazole is described as a partial
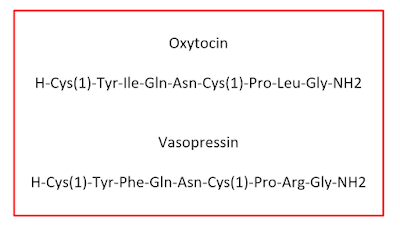
agonist activity at D2 and 5-HT1A receptors and an antagonist at 5-HT2A receptors. Because of the limitations of this class of medications other molecular targets have been sought. Vasopressin and oxytocin and their receptor systems have become targets of interest by some research groups.
The best paper and the only paper (4) I was able to locate that was a comprehensive look at the research supporting this approach as well as the discovery path and synthesis of the ultimate chemical compounds is reference 4 below. It happens to be authored by chemists from Roche, the company that has been awarded FDA breakthrough status for it newly approved autism drug - Balovaptan (RG7314). Interestingly none of the 41 structures listed in the article matches the final structure given above. The paper is a testament to modern medicinal chemistry - not so much on the synthesis end but how compounds are screened for activity at specific receptors. All of the preliminary animal data point to the vasopressin G protein coupled receptor V1a. A V1a antagonist was thought to have possible anxiolytic, antidepressant and pro-social properties. Because of the similarity to oxytocin and potential candidate drug needed to not block V2 receptors mediating antidiuretic effects in the kidney and not counteract the prosocial effects of oxytocin.
The authors screened 700,000 compounds at a concentration of 10 μM and had a hit rate of 1.48% looking for an "orally available, CNS penetrant and selective V1a antagonist". They identified 8 compounds with suitable DMPK (drug metabolism and pharmacokinetics) parameters that might be suitable for human studies. From there they used a chemogenomics approach based on the assumption that proteins with similar binding sites similar ligands. They developed a list of human class A GPCRs (G-protein-coupled receptors). They used this approach to look at the 35 amino acids that form the transmembrane pocket for 298 GPCR receptor sequences.
At this time I cannot locate an FDA approved package insert for Balovaptan, more detailed information on its medicinal chemistry, or the details about the trial entitled the VANILLA ( Vasopressin ANtagonist to Improve sociaL communication in Autism ) a phase II trial of Balovaptan. I have located the author of a paper on the VANILLA trial that may have been associated with the drug getting approval and have requested that article. I did locate the FDA podcast (7) that briefly discusses how Balvaptan may be a breakthrough drug for autism spectrum disorder because it might address the core social deficits of the disorder. The podcast suggests that the company will not be filing for approval of the drug until 2020.
The only experimental data that I could find was a proof of mechanism study that basically looked at some purported measures of vasopression V1a antagonism (3,4). The authors used a compound (RG7713) that is not the Balovaptan (RG7314) designation in a randomized, double blind, placebo controlled, two period crossover study of 19 subjects with high functioning autism. The subjects had a mean age of 23 and a full scale IQ or 100. A single 20 mg dose infusion over two hours was administered. The subjects were tested on paradigms that looked at eye-tracking, affective speech recognition, reading the mind in the eyes (thought or mood) test, olfactory identification and scripted interactions to look at interpersonal skills. They were also rated on global functioning and anxiety.
The only significant result was a change in eye tracking with the compound of interest. The global rating of improved function was slightly improved. There were four adverse effects from RG7713 but not placebo. There were no serious adverse effects or early terminations.
Based on the currently available information, the proof of concept paper for a similar vasopressin V1a antagonist provides modest proof at best. As any clinician knows, in order to diagnose autism it requires not just a knowledge of the criteria, but clinical experience in observing autism. There is a high degree of subjectivity. In the popular media that has resulted in applying what appear to be diagnostic criteria to a number of very high functioning celebrities and concluding that they are on the autism spectrum. Reading through the objective measures used in this paper is concerning and makes me question the validity of several of the tests. I suppose the proof of concept at the pilot study level is justified by the eye tracking test since this is the single test with the most research in the disorder and it represents a clear clinically observed finding. What I will be looking for in future papers or the VANILLA study paper if I can get it is a more robust demonstration of objective findings. I think one of the best ways to do that is to use a stratified sample of subjects according to severity of the disorder.
It is always disappointing when the press leads with a story like this and there is a data vacuum. Let's hope they release some studies of Balovaptan and the package insert information, but that might not happen for a couple of years.
George Dawson, MD, DFAPA
References:
1: McCracken JT, McGough J, Shah B, Cronin P, Hong D, Aman MG, Arnold LE, Lindsay R, Nash P, Hollway J, McDougle CJ, Posey D, Swiezy N, Kohn A, Scahill L, Martin A, Koenig K, Volkmar F, Carroll D, Lancor A, Tierney E, Ghuman J, Gonzalez NM, Grados M, Vitiello B, Ritz L, Davies M, Robinson J, McMahon D; Research Units on Pediatric Psychopharmacology Autism Network. Risperidone in children with autism and serious behavioral problems. N Engl J Med. 2002 Aug 1;347(5):314-21. PubMed PMID: 12151468. DOI: 10.1056/NEJMoa013171
2: Umbricht D, Del Valle Rubido M, Hollander E, McCracken JT, Shic F, Scahill L, Noeldeke J, Boak L, Khwaja O, Squassante L, Grundschober C, Kletzl H, Fontoura P. A Single Dose, Randomized, Controlled Proof-Of-Mechanism Study of a Novel Vasopressin 1a Receptor Antagonist (RG7713) in High-Functioning Adults with Autism Spectrum Disorder. Neuropsychopharmacology. 2017 Aug;42(9):1924. doi: 10.1038/npp.2017.92. PubMed PMID: 28701745; PubMed Central PMCID: PMC5520791.
3: Umbricht D, Del Valle Rubido M, Hollander E, McCracken JT, Shic F, Scahill L, Noeldeke J, Boak L, Khwaja O, Squassante L, Grundschober C, Kletzl H, Fontoura P. A Single Dose, Randomized, Controlled Proof-Of-Mechanism Study of a Novel Vasopressin 1a Receptor Antagonist (RG7713) in High-Functioning Adults with Autism Spectrum Disorder. Neuropsychopharmacology. 2017 Aug;42(9):1914-1923. doi: 10.1038/npp.2016.232. Epub 2016 Oct 6. Erratum in: Neuropsychopharmacology. 2017 Aug;42(9):1924. PubMed PMID: 27711048; PubMed Central PMCID: PMC5520775.
4: Ratni H, Rogers-Evans M, Bissantz C, Grundschober C, Moreau JL, Schuler F, Fischer H, Alvarez Sanchez R, Schnider P. Discovery of highly selective brain-penetrant vasopressin 1a antagonists for the potential treatment of autism via a chemogenomic and scaffold hopping approach. J Med Chem. 2015 Mar 12;58(5):2275-89. doi: 10.1021/jm501745f. Epub 2015 Feb 18. PubMed PMID: 25654260.
5: Albers HE. Species, sex and individual differences in thevasotocin/vasopressin system: relationship to neurochemical signaling in the
social behavior neural network. Front Neuroendocrinol. 2015 Jan;36:49-71. doi:
10.1016/j.yfrne.2014.07.001. Epub 2014 Aug 4. Review. PubMed PMID: 25102443.
6: Francis SM, Sagar A, Levin-Decanini T, Liu W, Carter CS, Jacob S. Oxytocin andvasopressin systems in genetic syndromes and neurodevelopmental disorders. Brain
Res. 2014 Sep 11;1580:199-218. doi: 10.1016/j.brainres.2014.01.021. Epub 2014 Jan
22. Review. PubMed PMID: 24462936; PubMed Central PMCID: PMC4305432.
7:
FDA Podcast: 074 – Roche’s balovaptan for autism; Lutathera for GEP-NETs; SyMRI NEURO for myelin quantitation on MRI; FDA approves human exoskeleton