Like most physicians in the United States, I got a letter from US Surgeon General Vivek H. Murthy, MD last week. The focus of the letter was recruiting the assistance of physicians in solving what he describes as "an urgent health care crisis facing America: the opioid epidemic." As an addiction psychiatrist about one out of every three new patients that I see is addicted to opioids. I have been lecturing on this topic for 6 years now, so I have more than a passing interest in what the SG has to say. I have to say that Dr. Murthy wrote an excellent letter. I was particularly impressed with his second paragraph describing how the was a combination of good intentions to treat pain and aggressive marketing by pharmaceutical companies and the single most important sentence in the letter:
"Many of us were taught-incorrectly-that opioids are not addictive when prescribed for legitimate pain."
Since I was already out practicing for about a decade at the time, I was spared that initiative. I never assumed that opioids were not addictive, only that some people were more predisposed to addiction than others and that some had such strong adverse effects that they were very unlikely to become addicted. But in routine psychiatric practice, even before the epidemic it was common to see patients who demanded increasing amounts of addictive drugs or who were hospitalized for adverse effects. I had treated numerous people who appeared to have dementia, but were longstanding users of opioids, benzodiazepines, and even older sedative hypnotics.
Dr. Murthy goes on to detail the costs in terms of 2 million people with prescription opioid disorder, increasing heroin use, and increasing numbers of cases of HIV and hepatitis C. He acknowledges that treating pain with opioids and finding the correct balance between analgesia and addiction will not be easy. He encourages physicians to take the pledge to turn the tide on the opioid epidemic at www.TurnTheTideRx.org and reading the enclosed pocket card to the CDC Opioid Prescribing Guideline. He also encourages physicians to approach addiction as a chronic illness rather than a moral failing. That will probably result in some blowback from the addiction is not a disease crowd. I hope that it is clear from my previous postings that in popular surveys, most people consider addiction to be a disease. At the scientific level, I think it makes the most sense. A lot of the confusion in this area comes from a lack of appreciation about how substance use disorders are stratified. Volkow came up with a good definition in a New England Journal of Medicine paper earlier this year (1) - separating substance use disorders in general from addiction and defining addiction as severe DSM-5 substance use disorders. (the DSM-5 refrains from using the term addiction).
The enclosed card entitled "Prescribing Opioids For Chronic Pain" touches on a few of the high points. My section by section critique follows (the entire card is below in the supplementary section for review). Section 1 focuses on pain ratings using the old 0 to 10 scale where 10 is the "worst pain you can imagine". The unstated problem with that approach is that it is not quantitative and cannot be taken in isolation. There are people for example where this rating is completely unreliable. Section 2 is a consideration of non-opioid therapies. It lists the usual medication prescribed for chronic pain. The problem here is that acute pain is often an entry point for addiction. There are many people getting opioids like oxycodone and hydrocodone for what used to be considered trivial injuries, like an uncomplicated ankle sprain. The other acute pain entry point for addiction is post operative pain. There have been studies that show a significant number of patients are still taking opioids a year after their surgical procedure. It is common for me to interview very young patients who were given opioids for trivial injuries or surgery who became addicted to these drugs. Physicians need to be very clear on appropriate pain treatments and not offer choices. For example, I was told by a friend that he was in a situation where patients were offered acetaminophen, ibuprofen, oxycodone, or oxymorphone. This is exactly the wrong way to approach the treatment of pain. In a culture where many people consider themselves to be drug savvy - the overwhelming choice will always be the most euphoria producing opioid.
Section 3 is a discussion of the treatment plan. Treatment contracts can be useful here, because most patients need more than a discussion. They need a document that they can refer to. It also gives the physician clear anchor points that can be used when discussing a taper or need to discontinue the medication. Section 4 involves the complicated assessment of harm and misuse. For most physicians this means the capability to expand their diagnostic capacity from the primary condition and the associated pain disorder to being able to make the diagnosis of addiction. In some cases there are clear markers (toxicology screens), but in many cases, the patient has developed an addiction as a direct result of the physician's prescription and the line between therapeutic use and addiction is less clear.
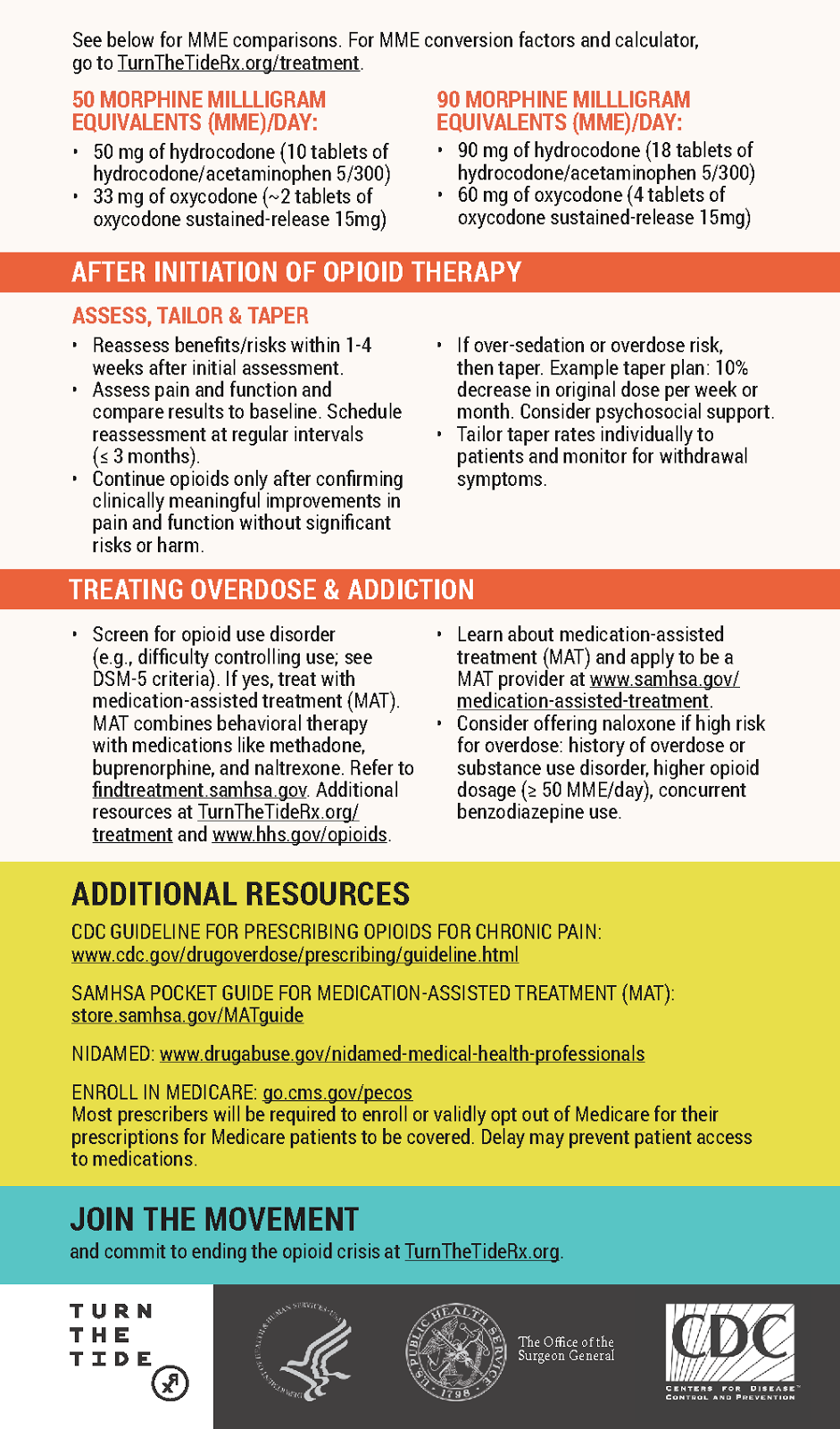
The card also provides clear examples of milligram morphine equivalents (MMEs). This is a term used frequently in the research literature. When comparing patients on different opioids it is useful to convert whatever opioid they are taking to MMEs. Mortality and morbidity with opioid prescriptions are generally associated with daily doses greater than 90-100 MME range. The card points out that this is about 90 mg of hydrocodone or 18 tablets of hydrocodone/acetaminophen 5/300 or 60 mg of oxycodone or 4 tablets of oxycodone sustained release 15 mg. In patients with addictions it is common to see chronic use of 120-240 mg oxycodone per day.
The card provides advice on starting low and going slow with the dose escalation as well as a suggested taper of 10% per week. It suggests limited supplies, much more limited for acute pain. It cautions against prescribing opioids and benzodiazepines concurrently - a practice that remains all too common. A sentence about how that happens might be useful. Chronic pain is typically associated with anxiety, depression, and insomnia. Patients typically are focused on symptomatic relief in all three areas. That can result not only in benzodiazepine prescriptions but also the prescription of cross tolerant sleep medication like zolpidem or eszopiclone. Another worse case scenario is the patient using extra opioids for treating these associated symptoms and that is very problematic. Educating patients about all of these contingencies easily exceeds the time that most primary care physicians have to spend with people. That may be another reason to have ample documentation available to assist physicians. There also needs to be a complete discussion of side effects and adverse effects from opioids.
The card transitions into treating an opioid use disorder with medication-assisted treatment like methadone, buprenorphine, or naltrexone. At this point, I think that the expertise of most primary care physicians has been exceeded and they are looking for referrals to treat the addiction. I think that the context of care needs to change. It is very difficult to be in a primary care setting focused on pain as the disorder one week and then transition to addiction care the next. Most patients will be unable to make that transition in the same clinic. The idea of offering naloxone for those with high overdose potential on the same card is also confusing. I could see how it might result in patients being treated for pain and getting prescribed opioids also getting naloxone. I think that naloxone is more appropriately used with a defined addiction and plan to address the addiction. The best approach to prevent oversedation and cognitive side effects is close monitoring and gradual dose increases.
All things considered this was a good first effort by the Surgeon General. I would like to see him become active in changing the cultural attitudes in the US about opioids. There is a myth that opioids are the magic bullet for pain relief and that is not true especially for chronic pain where the effects are modest and not typically better than non-opioids. There is a large segment of the American culture that also values getting high and opioids are always discussed from that perspective. Americans hoard opioid medications and give them away and trade them with other people for various reasons. When a medication becomes an urban legend like opioids have - it is like the old travelling medicine shows. Opioids are good for whatever ails you and they make you feel good as a useful side effect.
Countering all of those cultural biases about opioids is a big job - but I am reminded of Surgeon General Koop and his approach to altering American biases about tobacco smoke.
George Dawson, MD, DFAPA
References:
1: Volkow ND, Koob GF, McLellan AT. Neurobiologic Advances from the Brain Disease Model of Addiction. N Engl J Med. 2016 Jan 28;374(4):363-71. doi: 10.1056/NEJMra1511480. Review. PubMed PMID: 26816013. (full text).
Supplementary:
TurnTheTideRx Pocket Card as graphics below. You can also download the actual card as a pdf at this link: