The Mayo Clinic puts on very good conferences in Psychiatry. Two of the last three that I have attended had a strong biological and genetic emphasis. I was interested when I saw a reference in my Facebook feed to a study of potential biological markers of Bipolar I Disorder. It was even better that the article was published in the open access journal Translational Psychiatry. In the current article the authors looks at the results from the analysis of serum protein levels in controls and adults seeking treatment for depression and bipolar disorder. The sera of their subjects and controls was analyzed by Myriad RBM in a quantitative immunoassay designed to search for biomarkers through large numbers of proteins. The actual product and the proteins analyzed are described on the company's web page. All of the six proteins identified as possibly being discriminating as listed in the above graphic including growth differentiation factor 15 (GDF-15), hemopexin (HPX), hepsin (HPN), matrix metalloproteinase-7 (MMP-7), retinol-binding protein 4 (RBP-4), and transthyretin (TTR) can be located on this page and additional information is provided about the specific proteins
The authors emphasize in several places that this is a pilot or exploratory study but also point out that sufficient power to detect odds ratios for pairwise comparisons between mood disorders versus controls, bipolar disorder versus controls, and bipolar I versus controls. They looked at 272 proteins from 288 samples (141 controls, 52 Unipolar depression, 49 Bipolar II, and 46 Bipolar I). It was a one time cross sectional sample and no longitudinal sampling was done. Rigorous patient selection was used to reduce the risk of substance abuse disorders and inflammatory conditions. In a table describing patient characteristics, the cases had significantly greater BMI, greater lifetime illicit drug use, greater BMI, greater percentage of smokers, and fewer years of education. Existing symptoms were rated with the following scales IDS-C (depression), PHQ-9 (depression), GAD-7 (anxiety), YMRS (mania), and AUDIT (alcohol use). The cases were also being actively treated with antipsychotics, AED mood stabilizers, lithium, antidepressants, sedative/hypnotics, and thyroxine supplement.
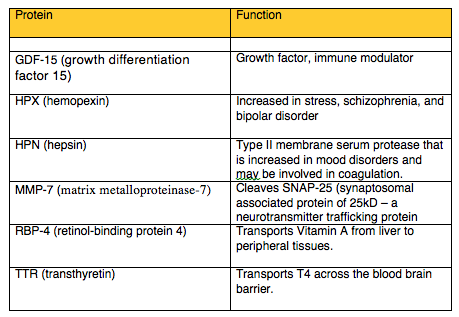
The graphic from the article labelled figure 2 above shows the differences in protein concentrations for the six proteins that were significantly different after Bonferroni correction by diagnosis. As can be seen from the figure all six proteins were at the highest levels in Bipolar I disorder. ROC curves and the ROC-AUC was used to determine which proteins were better predictors of Bipolar I Disorder. The text contains theoretical and speculative discussions of these particular proteins, what they have been associated with so far, and what importance that has for the issue of why their concentrations may vary in bipolar disorder.
There are a number of relevant considerations when looking at this type of proteomic analysis. The most obvious is the assumption that the underlying dynamics of the biological substrate can be measured in meaningful ways by knowing the protein signature of those systems. Although most of us are used to looking at cartoon depictions of neuron and synapses but the reality is much more complex. Recent work in Science shows that there are 62 proteins associated with synaptic bouton (2) and vesicle trafficking and that the copy number of these proteins varies greatly. The authors of that paper speculate that the production and number of those proteins may vary because some physical locations within the neuron may allow for an enrichment effect. One of the implicit assumptions in the Frye, et al paper is that psychiatric disorders may have a unique configuration in terms of synaptic architecture and that it will be reflected in the proteins responsible for that architecture. A further assumption is these CNS protein changes are all going to be reflected in the periphery and detectable in blood samples.
Although it is premature to draw many conclusions about the data in this study, the implications may be far reaching. It will be an interesting day in psychiatry if and when proteins will be used as biomarkers. It will be an interesting day even if variants can be found and reliably detected. Until then students of neuroscience and psychiatry will be able to appreciate that information flow in these systems is significant and we are just on the cusp of being able to understand it. We are just at the stage of moving from cartoon versions of neurons - to the real thing.
George Dawson, MD, DFAPA
References:
1: Frye MA, Nassan M, Jenkins GD, Kung S, Veldic M, Palmer BA, Feeder SE, Tye SJ, Choi DS, Biernacka JM. Feasibility of investigating differential proteomic expression in depression: implications for biomarker development in mood disorders. Transl Psychiatry. 2015 Dec 8;5:e689. doi: 10.1038/tp.2015.185. PubMed PMID: 26645624.
2: Wilhelm BG, Mandad S, Truckenbrodt S, Kröhnert K, Schäfer C, Rammner B, Koo SJ, Claßen GA, Krauss M, Haucke V, Urlaub H, Rizzoli SO. Composition of isolated synaptic boutons reveals the amounts of vesicle trafficking proteins. Science. 2014 May 30;344(6187):1023-8. doi: 10.1126/science.1252884. PubMed PMID: 24876496.
Attribution:
The figure at the top of this post is from the above reference 1 and is used per the conditions of a Creative Commons Attribution 4.0 International License.
Attribution:
The figure at the top of this post is from the above reference 1 and is used per the conditions of a Creative Commons Attribution 4.0 International License.