Anyone who has read this blog in the past is aware of my opinion of middlemen in health care and how they waste everyone's time and run up costs. Pharmacy Benefit Managers (PBM) remain there right up at the top. The PBM is the company that your doctor calls to get authorization so that an insurance plan will pay for all or part of a specific prescription drug. It has never been more clear to me that their sole function is to be an obstacle to the physician, the pharmacist and the patient. The goal of that obstruction is to increase the likelihood that anyone of those parties will give up at some point and either not fill the prescriptions or accept a different product that is less expensive, less effective, or one that has more side effects. I am sure that the pharmaceutical companies have gamed the system to make it harder for PBMs to deny claims on a scientific basis. They can do this by maximizing the number of FDA approved indications up front. In many cases that results in a product with multiple diverse indications so that the newer medication can be prescribed based on secondary indications. The physician, pharmacist and patient are left to deal with all of the unnecessary bureaucracy in between.
I posted my interaction with a PBM sometime ago and named them in that post. I learned about the power of corporate America as a result of that post. The VP of the company involved called me the next morning and wanted information about the patient involved. One thing led to another but the bottom line was that I pulled that post as a result of that sequence of events. Since my position has not significantly changed since then, the companies involved here will remain nameless. Keep in mind that identical transactions occur tens of thousands of times per day in the United States as PBMs and pharmaceutical companies battle for the healthcare dollar at your expense.
I am still working on the theory about how the VP of a PBM hears about a post on an obscure Internet blog and calls me the next day. The only three theories I have at this point are:
1. NSA grade Internet surveillance system by the managed care cartel.
2. A reader wants to see me silenced because they disagree with my viewpoint or just dislike psychiatrists. They forwarded the link to the company named in my original post.
3. My reputation as a tireless crusader against managed care and all of its associated systems. Well not so much a crusader, but there have been some memorable moments. Like a conference where I was speaking out against managed care - rather vehemently only to have the VP of one of these organizations remark: "Dr. Dawson - don't you work for a managed care organization?"
If I did - they never censored me.
Back to the case at hand. I was called originally by a pharmacist and had no information about the situation. I had to call her back and ask for a fax. I got the fax and it contained the prescription and a number for the PBM. I called and got their endless and indecipherable telephone queue. After typing in the correct identification number 3 times and saying it once (I thought I would forgo the voice recognition system that is set up to not work) I was put on hold and connected with a human. He asked me to "verify" in a line by line manner all of the data already on the faxed form. After wasting those minutes he talked about pulling up the prior authorization points as though he was going to call in another person for that detailed process. After a long pause (I am sure that many of my colleagues lose it at this point) he asked me the indication for the drug. This drug has only one indication and I told him. He said: "It's approved."
That sequence of events, taking a total of about 20 minutes would be enough to piss off any intelligent person, but then he said: "The office can call the pharmacy and tell them the prescription is authorized" I was momentarily confused and said "What office?" He said: "Your office."
That's right. Here we have a sequence of events that starts at the pharmacy with the PBM telling the pharmacist that prior authorization is needed. The pharmacist has to talk to me twice on the phone and send me a fax. And I have to complete this waste of time by calling and acting like an agent of the PBM. Just to be sure that I wasn't being totally lied to I asked the pharmacist if it was true that the physician's office had to call and complete this sequence from hell. Her response was "It's about 80:20 from the doctors' offices."
Call me a dinosaur. Call me a hot head. But this exercise in helping corporate America make more money, while taking valuable time away from me, my employer, my patients, and my family is an abomination and a manipulation. It can exist only in a country where corporate welfare is the rule of the day and conflict of interest is at all levels of government. From the perspective of corporate America prior authorization is a good way to get physicians and pharmacists to work for them for free. From the physician's perspective - it is a complete waste of time.
George Dawson, MD, DFAPA
Supplementary 1: Although the sequence of events listed above may sound incredible it is not. I have dealt with PBM telephone queues where there was no way out. You could not enter the numbers by keypad or say them through voice recognition. There was no way to speak to a human. I had to call the pharmacist back and explain that the prior authorization through the PBM was basically a sham and if the patient wanted the medication they would need to pay for it out of pocket.
It would be a lot more honest if the PBM would just tell people: "We make money by denying your prescriptions and in an ideal world we would prefer to not have to pay for anything."
But I guess that would be bad for public relations.
Monday, April 7, 2014
Thursday, April 3, 2014
More on Geriatric Depression and Overprescribing Antidepressants in Primary Care
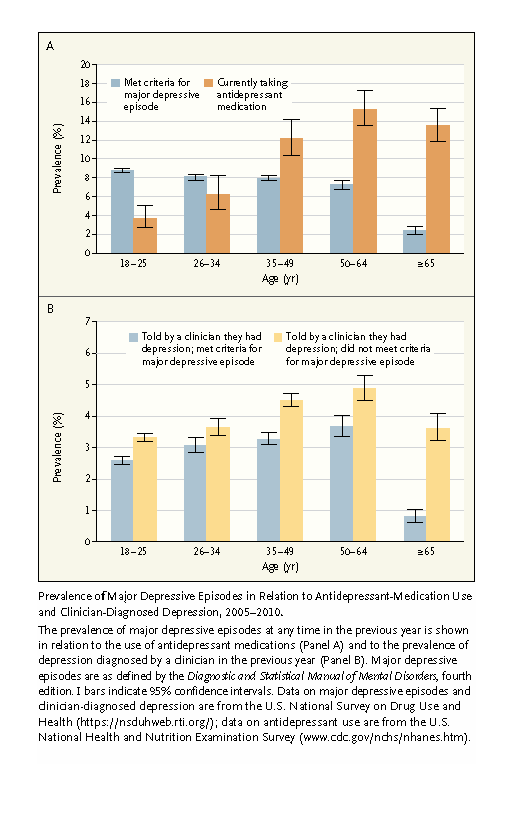
A recent article in the New England Journal of Medicine adds some more epidemiological data to the issue of the treatment of geriatric depression. The centerpiece of the article by Ramin Mojabai, MD is a graphic that is a combination of data from the National Survey on Drug Use and Health or NSDUH and the U.S. National Health and Nutrition Examination Survey or NHANES. His central point is that the majority of people diagnosed with depression in primary care clinics do not meet diagnostic criteria for major depression. The actual numbers for the elderly are 18% of those diagnosed with depression and 33% of those diagnosed with major depression actually have a diagnosis of major depression as assessed by rating scales or structured interviews. The bar graphs in the A panel illustrate that most people over the age of 35 who are taking antidepressants do not meet criteria for major depression. The opposite is true for the 18-34 year olds where antidepressant prescriptions are less than the prevalence of depression. Panel B illustrates that the prevalence of people who were told by their clinician that they had depression and did or did not meet criteria for major depression. In all cases the clinicians involved estimated non-major depression as being more prevalent than major depression. Can we learn anything from these graphs?
 The striking feature in Panel A is the dissociation of the total number of people taking antidepressants from the people with a diagnosis of major depression. I can see that happening for a couple of reasons. I would expect the number of people who are stable on antidepressant therapy to accumulate over time. Most of them would have major depression in stable remission and would no longer meet the criteria. A related issue is the atypical presentations of depression with increasing age. I have seen many cases of depression presenting as pseudodementia, Parkinson's syndrome, and polyarthritis or a similar chronic pain syndrome. In all cases, the symptoms responded to antidepressant medication but they would not meet criteria for major depression and most often the evaluation would resemble an evaluation for a medical problem. There is also the problem of depression in the aging population who have a form of dementia. At the upper end of this age distribution that may involve as many as 5% of the 65 year old population and they are likely overrepresented in primary care settings. Lastly there is the problem of suicide in the elderly. I reviewed a recent paper in the American Journal of Geriatric psychiatry that documented a decreased risk for suicide in elderly men and women who were taking antidepressants and the increased suicide risk in that group. It is likely that many primary care physicians are concerned about that higher level of risk and this may influence prescribing for this group. The other interesting comparison is that using different methodologies the ballpark antidepressant use in the elderly in Denmark approximates the antidepressant use on the US. It is probably a few percentage points lower, but the study in Denmark used a more robust marker of antidepressant use (refilling the actual prescription) rather than survey questions.
The striking feature in Panel A is the dissociation of the total number of people taking antidepressants from the people with a diagnosis of major depression. I can see that happening for a couple of reasons. I would expect the number of people who are stable on antidepressant therapy to accumulate over time. Most of them would have major depression in stable remission and would no longer meet the criteria. A related issue is the atypical presentations of depression with increasing age. I have seen many cases of depression presenting as pseudodementia, Parkinson's syndrome, and polyarthritis or a similar chronic pain syndrome. In all cases, the symptoms responded to antidepressant medication but they would not meet criteria for major depression and most often the evaluation would resemble an evaluation for a medical problem. There is also the problem of depression in the aging population who have a form of dementia. At the upper end of this age distribution that may involve as many as 5% of the 65 year old population and they are likely overrepresented in primary care settings. Lastly there is the problem of suicide in the elderly. I reviewed a recent paper in the American Journal of Geriatric psychiatry that documented a decreased risk for suicide in elderly men and women who were taking antidepressants and the increased suicide risk in that group. It is likely that many primary care physicians are concerned about that higher level of risk and this may influence prescribing for this group. The other interesting comparison is that using different methodologies the ballpark antidepressant use in the elderly in Denmark approximates the antidepressant use on the US. It is probably a few percentage points lower, but the study in Denmark used a more robust marker of antidepressant use (refilling the actual prescription) rather than survey questions.
The author addresses the issue of antidepressants being used for other applications like headaches and chronic pain chronic pain and states from an epidemiological perspective that two thirds of the prescriptions are for "clinician diagnosed mood disorder." The standard used in this study of DSM major depression criteria is too strict to use as a marker for antidepressant use since there are other valid psychiatric indications that primary care physicians are aware of and treat. Panic disorder, generalized anxiety disorder, social anxiety disorder and dysthymia are a few. There are also more fluid states like adjustment disorders that seem to merit treatment based on severity, duration, or in many cases by the fact that there are no other available treatment modalities. These are all possible explanation for the author's observation that the majority of people diagnosed with depression in primary care clinics do not meet criteria for major depression.
Diagnostic complexity is another issue in primary care settings. Patients are often less severely depressed, have significant anxiety, may have an undisclosed problem with drugs or alcohol, and have associated medical comorbidity. In an ideal situation, a diagnosis of depression is not necessarily an easy diagnosis to make. It takes the full cooperation of a patient who is a fairly accurate historian with regard to symptom onset and dates. They are harder to find than the literature suggests. The epidemiological literature often depends on lay interviewers using structured interviews like the DIS or SADS to make longitudinal diagnoses. This approach will not work for a large number of patients and a significant number will not be able to recall events, dates, medications or prior treatments with any degree of accuracy. With that level of uncertainty, antidepressant prescription often comes down to a therapeutic trial so that the patient and physician can directly observe what happens between them as the only available reliable data.
The author notes that the primary intervention for depression in primary care is the prescription of antidepressants. He talks about the ethical concerns about exposing patients especially the elderly to antidepressant drugs if it is not warranted, but he is using the major depression diagnosis here as the standard for treatment. He makes the same observation that I have made here that mass screening for depression is not warranted based on the concern about false positives. That stance is supported by the Canadian Task Force on Preventive Health Care. The U.S. Preventive Services Task Force recommends screening "when staff assisted depression care supports." My position is that screening, especially in medical populations is problematic not only from the false positive perspective but also because the screening checklist is often used as the diagnosis and an indication for starting antidepressant medications. Screening checklists are also political tools that are used to manipulate physicians. The best example I can think of is using serial PHQ-9 scores as a marker of depression treatment in primary care clinics even though it has not been validated for that application. As an extension of that application the PHQ-9 is used as a quality marker in clinics treating depression over time even though there is no valid way to analyze the resulting longitudinal data.
The author makes recommendations to limit the overuse of antidepressants and uses the stepped care approach with an example from the UK National Institute for Clinical Excellence or NICE. These guidelines suggest support and psychoeducation for patient with subsyndromal types of depression. A fuller assessment is triggered by very basic inquiries about mood and loss of interest. Amazingly the PHQ-9 is brought up as an assessment tool at that point. More monitoring and encouragement is suggested as a next step with a two week follow up to see if the symptoms remit spontaneously. Medications are a third step for longstanding depressions or those that do not remit with low level psychosocial interventions. An expert level of intervention is suggested for patient with psychosis, high risk of suicide, or treatment resistance. That seems like a departure for NICE relative to their guideline for the treatment of chronic neuropathic pain. In that case the referral for specialty care was contingent on a specific prescribing consideration (opioids) and the pain specialist was considered the gatekeeper for opioid prescriptions in this situation. Antidepressants are seen as overprescribed drugs but no gatekeeper is necessary. I suppose the argument could be made that there are not enough psychiatrists for the job, but are they really fewer than pain specialists who prescribe opioids for chronic neuropathic pain in the UK?
This model is only a slight variation on the Minnesota HMO model of screening everyone in a primary care clinic with a PHQ-9 and treating them as soon as possible with antidepressants. The driving factor here is cost. With a month of citalopram now costing as little as $4.00 - there is no conceivable low level psychosocial intervention that is more "cost effective". I have also been a proponent of computerized psychotherapy as a useful intervention and it is not likely that the Information Technology piece needed to deliver the psychotherapy would be that inexpensive. Another well known correlate of depression in the elderly is isolation and loneliness. I was not surprised to find that there were no interventions to target those problems since it would probably involve the highest cost. In the article standard research proven psychotherapies were recommended on par with the medical treatment of depression, but the question is - does anyone actually get that level of therapy anymore? My experience in assessing patients who have gone through it is that it is crisis oriented and patients are discharged at the first signs of improvement. That may happen after 2 or 3 sessions.
I doubt that the stepped care approach will do very much to curb antidepressant prescribing. This study suggests that overprescribing is a problem using a strict indication of major depression. There are always problems with how that is sorted out. I have not seen any studies where a team of psychiatrists goes into a primary care clinic and does the typical exhaustive diagnostic assessment that you might see in a psychiatric clinic. It would probably be much more relevant to the question at hand than standardized lay interviews or checklists. There is also a precedent for interventions to curb over prescribing of medications and that is the unsuccessful CDC program to reduce unnecessary antibiotic prescriptions. If clear markers of a lack bacterial infection can be ignored, what are the chances that an abstract diagnostic process will have traction?
And finally the stepped care interventions seem very weak. This is a good place for any number of professional and public service organizations to intervene and directly address the psychosocial aspects of depression in the elderly. Public education on a large scale may be useful. The psychoeducation pieces can be included in relevant periodicals ahead of time rather than as a way to avoid the use of medications. Environmental interventions to decrease isolation and loneliness is another potential solution. From a medical perspective, if the concern is medication risk every clinic where antidepressants are prescribed should have a clear idea of what those risks are and how to assess and prevent them. Patients who are at high risk from antidepressants should be identified and every possible non medication intervention (even the moderately expensive ones) should be exhausted before the prescription of antidepressant medication. Primary care prescribing patterns that potentially impact the patient on antidepressants should also be analyzed and discussed. A focus on risks and side effects can have more impact on the prescription of antidepressants than psychosocial interventions and waiting for the depression to go away.
George Dawson, MD, DFAPA
Supplementary 1: Permission and credit for the graphic:
"From New England Journal of Medicine, Ramin Mojtabai, Diagnosing depression in older adults in primary care. Volume No 370, Page No. 1181, Copyright © (2014) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society."

The author addresses the issue of antidepressants being used for other applications like headaches and chronic pain chronic pain and states from an epidemiological perspective that two thirds of the prescriptions are for "clinician diagnosed mood disorder." The standard used in this study of DSM major depression criteria is too strict to use as a marker for antidepressant use since there are other valid psychiatric indications that primary care physicians are aware of and treat. Panic disorder, generalized anxiety disorder, social anxiety disorder and dysthymia are a few. There are also more fluid states like adjustment disorders that seem to merit treatment based on severity, duration, or in many cases by the fact that there are no other available treatment modalities. These are all possible explanation for the author's observation that the majority of people diagnosed with depression in primary care clinics do not meet criteria for major depression.
Diagnostic complexity is another issue in primary care settings. Patients are often less severely depressed, have significant anxiety, may have an undisclosed problem with drugs or alcohol, and have associated medical comorbidity. In an ideal situation, a diagnosis of depression is not necessarily an easy diagnosis to make. It takes the full cooperation of a patient who is a fairly accurate historian with regard to symptom onset and dates. They are harder to find than the literature suggests. The epidemiological literature often depends on lay interviewers using structured interviews like the DIS or SADS to make longitudinal diagnoses. This approach will not work for a large number of patients and a significant number will not be able to recall events, dates, medications or prior treatments with any degree of accuracy. With that level of uncertainty, antidepressant prescription often comes down to a therapeutic trial so that the patient and physician can directly observe what happens between them as the only available reliable data.
The author notes that the primary intervention for depression in primary care is the prescription of antidepressants. He talks about the ethical concerns about exposing patients especially the elderly to antidepressant drugs if it is not warranted, but he is using the major depression diagnosis here as the standard for treatment. He makes the same observation that I have made here that mass screening for depression is not warranted based on the concern about false positives. That stance is supported by the Canadian Task Force on Preventive Health Care. The U.S. Preventive Services Task Force recommends screening "when staff assisted depression care supports." My position is that screening, especially in medical populations is problematic not only from the false positive perspective but also because the screening checklist is often used as the diagnosis and an indication for starting antidepressant medications. Screening checklists are also political tools that are used to manipulate physicians. The best example I can think of is using serial PHQ-9 scores as a marker of depression treatment in primary care clinics even though it has not been validated for that application. As an extension of that application the PHQ-9 is used as a quality marker in clinics treating depression over time even though there is no valid way to analyze the resulting longitudinal data.
The author makes recommendations to limit the overuse of antidepressants and uses the stepped care approach with an example from the UK National Institute for Clinical Excellence or NICE. These guidelines suggest support and psychoeducation for patient with subsyndromal types of depression. A fuller assessment is triggered by very basic inquiries about mood and loss of interest. Amazingly the PHQ-9 is brought up as an assessment tool at that point. More monitoring and encouragement is suggested as a next step with a two week follow up to see if the symptoms remit spontaneously. Medications are a third step for longstanding depressions or those that do not remit with low level psychosocial interventions. An expert level of intervention is suggested for patient with psychosis, high risk of suicide, or treatment resistance. That seems like a departure for NICE relative to their guideline for the treatment of chronic neuropathic pain. In that case the referral for specialty care was contingent on a specific prescribing consideration (opioids) and the pain specialist was considered the gatekeeper for opioid prescriptions in this situation. Antidepressants are seen as overprescribed drugs but no gatekeeper is necessary. I suppose the argument could be made that there are not enough psychiatrists for the job, but are they really fewer than pain specialists who prescribe opioids for chronic neuropathic pain in the UK?
This model is only a slight variation on the Minnesota HMO model of screening everyone in a primary care clinic with a PHQ-9 and treating them as soon as possible with antidepressants. The driving factor here is cost. With a month of citalopram now costing as little as $4.00 - there is no conceivable low level psychosocial intervention that is more "cost effective". I have also been a proponent of computerized psychotherapy as a useful intervention and it is not likely that the Information Technology piece needed to deliver the psychotherapy would be that inexpensive. Another well known correlate of depression in the elderly is isolation and loneliness. I was not surprised to find that there were no interventions to target those problems since it would probably involve the highest cost. In the article standard research proven psychotherapies were recommended on par with the medical treatment of depression, but the question is - does anyone actually get that level of therapy anymore? My experience in assessing patients who have gone through it is that it is crisis oriented and patients are discharged at the first signs of improvement. That may happen after 2 or 3 sessions.
I doubt that the stepped care approach will do very much to curb antidepressant prescribing. This study suggests that overprescribing is a problem using a strict indication of major depression. There are always problems with how that is sorted out. I have not seen any studies where a team of psychiatrists goes into a primary care clinic and does the typical exhaustive diagnostic assessment that you might see in a psychiatric clinic. It would probably be much more relevant to the question at hand than standardized lay interviews or checklists. There is also a precedent for interventions to curb over prescribing of medications and that is the unsuccessful CDC program to reduce unnecessary antibiotic prescriptions. If clear markers of a lack bacterial infection can be ignored, what are the chances that an abstract diagnostic process will have traction?
And finally the stepped care interventions seem very weak. This is a good place for any number of professional and public service organizations to intervene and directly address the psychosocial aspects of depression in the elderly. Public education on a large scale may be useful. The psychoeducation pieces can be included in relevant periodicals ahead of time rather than as a way to avoid the use of medications. Environmental interventions to decrease isolation and loneliness is another potential solution. From a medical perspective, if the concern is medication risk every clinic where antidepressants are prescribed should have a clear idea of what those risks are and how to assess and prevent them. Patients who are at high risk from antidepressants should be identified and every possible non medication intervention (even the moderately expensive ones) should be exhausted before the prescription of antidepressant medication. Primary care prescribing patterns that potentially impact the patient on antidepressants should also be analyzed and discussed. A focus on risks and side effects can have more impact on the prescription of antidepressants than psychosocial interventions and waiting for the depression to go away.
George Dawson, MD, DFAPA
Supplementary 1: Permission and credit for the graphic:
"From New England Journal of Medicine, Ramin Mojtabai, Diagnosing depression in older adults in primary care. Volume No 370, Page No. 1181, Copyright © (2014) Massachusetts Medical Society. Reprinted with permission from Massachusetts Medical Society."
Sunday, March 30, 2014
A Lemon Law for Medications?
I always hear about expensive medications and what a racket that is for Big Pharma. A recent exacerbation of asthma was an eye opener for me. I have had to discard a lot of medications prescribed for me in the past because they either were not indicated (like an antibiotic for cellulitis when I really had gout) or medications that I thought were too risky (they shall remain nameless).
I posted some of my experiences with medications taken for asthma. Over a two month period I took oral prednisone in addition to corticosteroid inhalers and beta agonist bronchodilators. All of the medication was only moderately effective over a two month period and this necessitated switching between different preparations. It also involved discarding some after only one or two doses due to intolerable side effects. That trial and error came an a high cost. Like most employees these days I have a high deductible health insurance plan. That deductible is $3,000. The final tab between the dates January 20, 2014 and February 25, 2014 was $3,000 out-of-pocket. So I guess the good news is that I met my deductible for this year.
The drug costs are instructive. Some of the inhalers retail for $500 apiece. The out-of-pocket costs for a high deductible insurance plan varies from $50.65 to $251.03. The total out-of-pocket drug cost for one month of treatment for asthma was $1,284.92. The most important part was that about half of that cost was for medications that could not be tolerated or were ineffective and had to be discontinued ($565.72). This is a form of cost shifting that nobody ever talks about. I have over $500 worth of medication sitting on the shelf and ready to be discarded because it was ineffective or could not be tolerated. When I think about how many times I have prescribed a medication for a patient only to have the PBM fax me to say that they would only fill 90 days worth of the medication, I wonder about how many tens of thousands of these prescriptions are sitting out there unused.
What about really expensive medications? Some of those are about the equivalent in cost to a new car or several new cars. To give two examples of medications I recently learned about consider Olysio (simeprevir) and Sovaldi (sofosbuvir) new drugs for hepatitis C. Sofosbuvir costs $954.90 for a 400 mg tablet or a full course of therapy for $35,000 - $70,000. Simeprevir is $753.37 for a single 150 mg capsule. I have already read the cost-benefit analyses of theses medications and like most analyses of very expensive medications they seem justified. What happens when you take a very expensive agent like this and it is ineffective or you can't tolerate the side effects? Medicine may be the only area in American life where the customer underwrites the product cost no matter what. What other product works like that? Lemon laws protect car purchases. If you buy a new house, as part of that agreement you either sign an arbitration agreement or you are free to sue if something happens to that house. Most big ticket item retailers have return policies. With medications you are often left with an unused bottle staring at you from the medicine chest and reminding you of what it costs. It probably takes on a lot more importance now that the average employer plan leads to very high out-of-pocket costs.
I don't mean to imply that any of these products are ineffective. My thoughts on what the FDA does in terms of drug approval are recorded here in this blog. This all has to do with biological variability and balancing Type I versus Type II error. Some of the medications I could not tolerate work exceedingly well for other people. Some of the medications I take are toxic to others. There are no medications that work well with minimal side effects across the entire population.
Is there a solution to this problem? I think there is a very straightforward one. Give the pharmacist the option of supplying a smaller portion of the prescription for the patient to test. For example, a week of pills or an inhaler with a week of inhalations. That would have saved me nearly $400 in unnecessary costs. The environmental costs are also unknown. There has only been recent interest in what happens to discarded pharmaceuticals when they enter our waste disposal systems and waterways. That cost is currently unknown but needs to be considered. This post also highlights the difference between biological products like prescriptions and non biological products like cars. If a car is a lemon, that is independent of the biology of the owner. Whether a prescription drug is a lemon or not is solely determined by biology.
As the cost of health care is shifted back to the consumer, the financing needs to be like any other expensive consumer good. That would include some safeguard of value for the money.
George Dawson, MD, DFAPA
I posted some of my experiences with medications taken for asthma. Over a two month period I took oral prednisone in addition to corticosteroid inhalers and beta agonist bronchodilators. All of the medication was only moderately effective over a two month period and this necessitated switching between different preparations. It also involved discarding some after only one or two doses due to intolerable side effects. That trial and error came an a high cost. Like most employees these days I have a high deductible health insurance plan. That deductible is $3,000. The final tab between the dates January 20, 2014 and February 25, 2014 was $3,000 out-of-pocket. So I guess the good news is that I met my deductible for this year.
The drug costs are instructive. Some of the inhalers retail for $500 apiece. The out-of-pocket costs for a high deductible insurance plan varies from $50.65 to $251.03. The total out-of-pocket drug cost for one month of treatment for asthma was $1,284.92. The most important part was that about half of that cost was for medications that could not be tolerated or were ineffective and had to be discontinued ($565.72). This is a form of cost shifting that nobody ever talks about. I have over $500 worth of medication sitting on the shelf and ready to be discarded because it was ineffective or could not be tolerated. When I think about how many times I have prescribed a medication for a patient only to have the PBM fax me to say that they would only fill 90 days worth of the medication, I wonder about how many tens of thousands of these prescriptions are sitting out there unused.
What about really expensive medications? Some of those are about the equivalent in cost to a new car or several new cars. To give two examples of medications I recently learned about consider Olysio (simeprevir) and Sovaldi (sofosbuvir) new drugs for hepatitis C. Sofosbuvir costs $954.90 for a 400 mg tablet or a full course of therapy for $35,000 - $70,000. Simeprevir is $753.37 for a single 150 mg capsule. I have already read the cost-benefit analyses of theses medications and like most analyses of very expensive medications they seem justified. What happens when you take a very expensive agent like this and it is ineffective or you can't tolerate the side effects? Medicine may be the only area in American life where the customer underwrites the product cost no matter what. What other product works like that? Lemon laws protect car purchases. If you buy a new house, as part of that agreement you either sign an arbitration agreement or you are free to sue if something happens to that house. Most big ticket item retailers have return policies. With medications you are often left with an unused bottle staring at you from the medicine chest and reminding you of what it costs. It probably takes on a lot more importance now that the average employer plan leads to very high out-of-pocket costs.
I don't mean to imply that any of these products are ineffective. My thoughts on what the FDA does in terms of drug approval are recorded here in this blog. This all has to do with biological variability and balancing Type I versus Type II error. Some of the medications I could not tolerate work exceedingly well for other people. Some of the medications I take are toxic to others. There are no medications that work well with minimal side effects across the entire population.
Is there a solution to this problem? I think there is a very straightforward one. Give the pharmacist the option of supplying a smaller portion of the prescription for the patient to test. For example, a week of pills or an inhaler with a week of inhalations. That would have saved me nearly $400 in unnecessary costs. The environmental costs are also unknown. There has only been recent interest in what happens to discarded pharmaceuticals when they enter our waste disposal systems and waterways. That cost is currently unknown but needs to be considered. This post also highlights the difference between biological products like prescriptions and non biological products like cars. If a car is a lemon, that is independent of the biology of the owner. Whether a prescription drug is a lemon or not is solely determined by biology.
As the cost of health care is shifted back to the consumer, the financing needs to be like any other expensive consumer good. That would include some safeguard of value for the money.
George Dawson, MD, DFAPA
Thursday, March 27, 2014
Dr. Fischbach and the Pittsburgh Post-Gazette on the State of Psychiatry
I received a link to this excellent post by Marnin E. Fischbach commenting on two articles in the Pittsburgh Post Gazette on the shortage of psychiatrists, why people have difficulty finding a psychiatrist, and his broad overview of the importance of psychiatry. From other sources I have learned that Dr. Fischbach has over 40 years experience as a psychiatrist. It is good to find another psychiatrist who has confidence in their colleagues. Even though most of my colleagues would agree, that is often not the public opinion stated by many psychiatrists. Conflict of interest issues do not apply since it appears that Dr. Fischbach is not selling a book or trying to come across like somebody who can correct the deficiencies in his colleagues.
His subtitle is critical:
"If more people knew what psychiatrists really do, there would be more of them and better health care for everyone".
His subtitle is critical:
"If more people knew what psychiatrists really do, there would be more of them and better health care for everyone".
In his elaboration he discusses inaccurate portrayals in the media, the lack of "whiz bang technology" like some other specialties and how the general stigma of mental illness also attaches itself to psychiatrists. His discussion of the value of psychiatrists has 5 significant points. Those points include being "willing and able" to deal with the mental forces that affect the human condition, having the broadest understanding of all of the factors that affect those forces, diagnosing and treating borderland conditions because our work requires close attention and listening, being first and foremost physicians, and providing treatment that results in patients getting better. None of these points should come as any surprise. It is only in the context of media bias against psychiatry that they do.
At the end of his essay he states: "I have much faith in our psychiatric profession and great respect for its practitioners." That is a good note to end on. The other theme in the essay was addressing the compensation of psychiatrists. That was critical because it speaks to the shortage of psychiatrists and the two previous articles. It also explains why psychiatrists refuse to accept insurance, but his article does not explain the underlying reason. Most people do not understand that as far as most insurers go, psychiatry is "carved out" from all other medical specialities. In terms of managed care organizations that means services that are either not covered or that are covered by a much different payment mechanism that other medical services. It was actually part of the federal reimbursement scheme until new rules allowed the submission of standard medical billing codes. It makes sense that if managed care companies expect you to accept minimal or in some cases trivial reimbursement that you would refuse to contract with them and accept patients who subscribe to that plan. It is clear cut rationing of psychiatric services by insurance companies and the government.
The other area in Dr. Fischbach's essay that is impacted by similar rationing mechanisms is the collaborative care model. As I have pointed out, this is an extension of rationing by both the managed care cartel and the government that will only result in psychiatry being further marginalized.
Psychiatry is a vital and effective medical specialty. The biases against psychiatry that he mentions and the biases noted in the original article are significant and in my opinion are a larger factor in reducing the number of psychiatrists than the compensation issue. That is why those biases are addressed right here on this blog.
I congratulate Dr. Fischbach on pointing out and elaborating these biases in his essay and and share his positive regard for our colleagues. I encourage a read of his well written essay and a look at the links to the two articles that he is responding to. Never forget that access to psychiatrists is restricted by both the government and the managed care cartel and one of the reasons they can do that is the longstanding stigma against mental illness.
George Dawson, MD, DFAPA
Monday, March 24, 2014
The Problem With Making Medical Information More Like Financial Information
I have been an interested reader of financial information for the the past 40 years. My uncle was an avid stock market investor when I was a kid and he got me interested in reading the Value Line investment survey. I still read it and base some of my decisions on it. Over the years I have had some degree of success in investing, but it hasn't all been good. One of my greatest successes was a defensive maneuver that resulted in me not losing anything during the stock market crash of 2008. I have been a subscriber at one time or another to most of the significant investment magazines and newspapers in the United States.
It has been interesting to observe what has happened to what has come to be known as the financial services industry over my investing career because it has implications for the increasing business control over medicine. I have already alluded to many on these implications on this blog including treating knowledge workers like production workers and creating an unhealthy work environment that results in a lack of empathy for the patients being treated. But there are even larger implications. Financial services industry friendly legislation has probably been the single largest contributor to the idea that the privacy of individuals is relative to the advantages gained by establishing credit reporting. Credit reporting agencies were born out of the idea that data could be collected under a Social Security Number and released to any financial institution without the consent of the person behind that SSN. That single idea violated a previous promise by Congress that SSNs would not be used as any type of national identifier and was single handedly responsible for creating a multi-billion dollar industry that basically buys and sells credit information and the identity theft industry - both the criminal side and the services to protect people from the criminals. It is much harder to be an identity thief in a world that does not have credit information centralized on a SSN.
The driving force behind businesses everywhere is to create leverage that results in people needing to buy a product or service and make it so they can't get it anywhere else. We hear a lot about competition and its importance in capitalism, but there is plenty of evidence that capitalism is not only lacking but that measures are often in place to severely restrict it. It results in an industry that is set up to optimize gain from consumers while keeping them all at risk. As an example, one of the "low risk" strategies for investing with some of these companies is to investment in index funds. As retirement nears, the recommendation can be to put funds into an annuity or with an advisor who can determine withdrawal rates, reallocation, and future investment decisions. In many cases the retiree is charged up to 1% for that service on top of whatever service charges and transaction fees are associated with the funds that are invested in. There is always the disclaimer that there is no guarantee of income from the account and this is compounded by the fact that interest on cash and money market funds is at an all time low. Very few investors can fund their retirement by interest on so-called safe investments and in the last decade we have witnessed the first losses on money market funds. All things considered, regulation at all levels seems like it is clearly set up to favor the financial services industry. They have a license to warn you that you can lose money even though you may be paying them to protect it - and that's OK. In some extreme examples, investment banks have recommended purchases to customer that they were actively betting against.
I don't know how many people can see the trend, but it is pretty obvious to me. As medical information gets more like financial information - it moves farther away from any reality basis and it becomes a vehicle for manipulation. The whole point of collecting data from a medical and scientific standpoint is to look at underlying meaning specifically implications for health care. The best example is lab data. If I look at a patient's CBC with differential count and chemistry profile, I have about 40 data points, any one of which could have significant health implications for the care of that individual. If I look at various quality markers and screening scores that are being collected for business purposes that data varies from questionable to clearly invalid and yet physicians are being held "accountable" for what is essentially business quality data. In other words, data that has no scientific basis and can be manipulated for a specific result. The usual intent is to maximize business profits and make it seem like the business is much more critical to the provision of health care than the health professionals it hires. As absurd as that last sentence looks, it is without a doubt one of the goals of most health care businesses.
Business information collected and manipulated for the sake of furthering business interests in the health care industry is no more valid than what happens in the financial services industry. Both types of information have evolved to place the consumer at risk all of the time and give them no clear reason for a making a decision in their own interest. And in both cases, consumers have no choice but to participate. We have a government mandated retirement industry that provides a windfall to financial services. We now have a government mandated health care industry that is set to provide a windfall the large health care and pharmaceutical companies. In both cases it is underwritten by the American consumer who is placed at financial risk all of the time in an economy of stagnant wages and significant unemployment.
George Dawson, MD, DFAPA
It has been interesting to observe what has happened to what has come to be known as the financial services industry over my investing career because it has implications for the increasing business control over medicine. I have already alluded to many on these implications on this blog including treating knowledge workers like production workers and creating an unhealthy work environment that results in a lack of empathy for the patients being treated. But there are even larger implications. Financial services industry friendly legislation has probably been the single largest contributor to the idea that the privacy of individuals is relative to the advantages gained by establishing credit reporting. Credit reporting agencies were born out of the idea that data could be collected under a Social Security Number and released to any financial institution without the consent of the person behind that SSN. That single idea violated a previous promise by Congress that SSNs would not be used as any type of national identifier and was single handedly responsible for creating a multi-billion dollar industry that basically buys and sells credit information and the identity theft industry - both the criminal side and the services to protect people from the criminals. It is much harder to be an identity thief in a world that does not have credit information centralized on a SSN.
The driving force behind businesses everywhere is to create leverage that results in people needing to buy a product or service and make it so they can't get it anywhere else. We hear a lot about competition and its importance in capitalism, but there is plenty of evidence that capitalism is not only lacking but that measures are often in place to severely restrict it. It results in an industry that is set up to optimize gain from consumers while keeping them all at risk. As an example, one of the "low risk" strategies for investing with some of these companies is to investment in index funds. As retirement nears, the recommendation can be to put funds into an annuity or with an advisor who can determine withdrawal rates, reallocation, and future investment decisions. In many cases the retiree is charged up to 1% for that service on top of whatever service charges and transaction fees are associated with the funds that are invested in. There is always the disclaimer that there is no guarantee of income from the account and this is compounded by the fact that interest on cash and money market funds is at an all time low. Very few investors can fund their retirement by interest on so-called safe investments and in the last decade we have witnessed the first losses on money market funds. All things considered, regulation at all levels seems like it is clearly set up to favor the financial services industry. They have a license to warn you that you can lose money even though you may be paying them to protect it - and that's OK. In some extreme examples, investment banks have recommended purchases to customer that they were actively betting against.
I don't know how many people can see the trend, but it is pretty obvious to me. As medical information gets more like financial information - it moves farther away from any reality basis and it becomes a vehicle for manipulation. The whole point of collecting data from a medical and scientific standpoint is to look at underlying meaning specifically implications for health care. The best example is lab data. If I look at a patient's CBC with differential count and chemistry profile, I have about 40 data points, any one of which could have significant health implications for the care of that individual. If I look at various quality markers and screening scores that are being collected for business purposes that data varies from questionable to clearly invalid and yet physicians are being held "accountable" for what is essentially business quality data. In other words, data that has no scientific basis and can be manipulated for a specific result. The usual intent is to maximize business profits and make it seem like the business is much more critical to the provision of health care than the health professionals it hires. As absurd as that last sentence looks, it is without a doubt one of the goals of most health care businesses.
Business information collected and manipulated for the sake of furthering business interests in the health care industry is no more valid than what happens in the financial services industry. Both types of information have evolved to place the consumer at risk all of the time and give them no clear reason for a making a decision in their own interest. And in both cases, consumers have no choice but to participate. We have a government mandated retirement industry that provides a windfall to financial services. We now have a government mandated health care industry that is set to provide a windfall the large health care and pharmaceutical companies. In both cases it is underwritten by the American consumer who is placed at financial risk all of the time in an economy of stagnant wages and significant unemployment.
George Dawson, MD, DFAPA
Friday, March 21, 2014
Compassion Fatigue? Or Sometimes You Eat The Shark And Sometimes The Shark Eats You
I passed a pamphlet for a conference on Compassion Fatigue today and thought to myself: "Why haven't I ever encountered the term compassion in medical school or at any point in my medical or professional training?" If you look it up in a real dictionary there seems to be multiple meanings ranging from: "A feeling of wanting to help someone who is sick, hungry, in trouble, etc." to "a feeling of deep sympathy and sorrow for another who is stricken by misfortune, accompanied by a strong desire to alleviate suffering." None of these definitions seems to capture what happens in medicine and how physicians are trained. It seems like an undisciplined emotional reaction to human suffering. That may seem a bit calloused to someone outside the field but would you want your surgeon operating on you in the throes of an emotional reaction? Would you want your internist or psychiatrist recommending medication for you during an emotional episode? On the other hand, depending on what part of the definition I focus on, I have already pointed out that in my opinion the overprescribing of medications is motivated at some level by "a strong desire to alleviate suffering." More evidence that compassion may not be the best basis for medical decisions.
I can still recall the first patient that I was responsible for. The very first patient I evaluated on Internal Medicine as a third year medical student. He was not much older than me, but at that point he had a much harder life. As he explained his symptoms to me and we did the examination, I found myself getting more and more anxious. I realized that he had a very serious illness that he was not going to recover from. I pulled all of the test results and x-rays together so I could present it in our team meeting in the morning. I could barely get the information out to my chief resident and attending. I was overcome with emotion. My voice cracked. I was tearing up. My head was spinning. I was focused on how unfair life was. He was a young guy, just like me with the usual hopes, dreams, and relationships that we all have and through no fault of his own, he had developed a terminal illness. I certainly wanted to help him, but there was nothing that could be done. That happens so frequently in medicine, using the most emotional definition of compassion would render most physicians nonfunctional. It tends to alter your focus. The focus has to be on what is happening right here and right now and not the unfairness of the process. The focus needs to be on the technical details or you can't provide competent care and tell people what they need to know. As I have gotten older, I have an image for the process of unpredictable disease and death. It reminds me of the war movie where the fleet is sunk and everyone is bobbing in the Pacific Ocean wearing life preservers. Suddenly the sharks appear and people start to die on a random basis. Whoever the sharks decide to kill. A random horrific process. That is my image.
It may explain the reaction of one of my attendings when I was a resident on a busy inpatient psychiatric unit. I was reading the description of one of our consultants to him and the consultant used the adjective "unfortunate" to describe all of the medical problems the patient had sustained. My attending glared at me and said: "Why is he unfortunate?" It seemed like an obvious descriptor to me. Anyone with all of these severe medical problems could be described as unfortunate, but I could not respond to him at the time. It seems to me if the sharks get you or there is a near miss, unfortunate in the bad luck sense may be a good description. He may have been thinking of another definition. But I think he was most likely giving me the message that it is best to not even recognize the random walk through life and the fact that the shark can eat you at any time. Without that element of denial, how can you function? How can you function as a physician?
After you have talked with thousands of people about their traumas and adversities, you realize that most people suffer. Personal biases make some people want to alleviate the suffering of some more than others. Nobody wants to see children suffer. There are some people who attract the ill wishes of others. They are generally unlikable or they have perpetrated some kind of shocking crime. There seems to be a likeability bias with compassion and that also makes it less useful for physicians. Physicians are obliged to perform competent medical care irrespective of how well the person is liked. There are often errors on the side of people who are very likeable. Sometimes physicians and medical staff get very attached to person based on their personality, physical characteristics, or demeanor. You may want to help that likeable person more, but that doesn't translate into whether you can or not.
If you are trained to render assistance, save lives when you can and alleviate suffering where does the compassion that you had before medical school go? Without invoking defense mechanisms it gets converted to other things that are adaptive in the profession. Empathy and technical skill are good examples. Empathy is probably a more accurate emotional appreciation of what is occurring in a person you are trying to help. It is focused on that person and their emotional state and if reflected back to that person they would agree with the observations. A better measure of burnout for physicians especially psychiatrists would be empathy fatigue rather than compassion fatigue. Seeing people as collections of symptoms and having no appreciation for the emotional side of their experience would be one example. Seeing patients as an endless stream of problems that you need to fix rather than unique individuals would be another. As the days get longer there are also the comparisons physicians make about how much time they spend taking care of others compared to how much time they spend with their families. As the family time gets shorter it may be harder to empathize with increasing numbers of patients.
Whether it is compassion fatigue or burnout, these seminars all seem to teach the same things. It is fashionable to refer to the skills as "tools". Mindfulness techniques, cognitive behavioral therapy. relaxation techniques, meditation, diet, sleep, and exercise are all parts of the "toolkit." Nobody ever seems to address the severely deteriorated work environment as a cause and ongoing factor. Productivity demands on physicians in terms of the number of patients seen, the amount of documentation that needs to be done and the other aspects of being a good corporate citizen are a recipe for burnout and that is probably the most common job scenario for physicians these days. Professional organizations seem to ignore that fact that if physicians are going to function the way they should and treat the whole person, a work environment without adequate time to talk with patients in one of the fast paths to burnout.
No amount of "tools" can reverse that.
George Dawson, MD, DFAPA
Supplementary 1: In talking with people over the years and trying to help them stay on the job, the most significant problem is unreasonable employers. People work in jobs where the job directly impacts their health. The best example is alternating shifts and never being able to establish a regular sleep routine. Hospitals are some of the worst offenders. They have adopted policies that allow them to tell nursing staff that they need to work "mandatory doubles" when there are shortages. The policies that have hospitalists working 7 days on and 7 days off are no better. I have interviewed hospitalists about their cognitive efficiency on day 6 and 7 and have been told that it generally plummets. They are taking twice as long to do the documentation and it is difficult to think. I was in a similar position one year when I was running a 20 bed inpatient service with assistance of a physician's assistant. I had to see everyone, everyday and managed both the medical and psychiatric diagnoses. When I decided to stop doing that, I was replaced by two full time psychiatrists and an internal medicine specialist to take care of all of the medical problems. Eventually those two psychiatrists felt it was too much work and a third psychiatrist was added to cover 4 of the 20 patients. The adverse effect of a business model on employee health that operates on personnel expenses cut to the bone can not be overemphasized. Hospitals and clinics will happily work medical staff to the point that it adversely impacts their health and lifestyle, adversely impacts their cognitive abilities at work, leads to burnout, and leaves them in a state where empathy is a thing of the past.
The only reason I quit running a 20 bed inpatient unit by myself was a colleague of mine who told me he did it for years - right up to the point he had his first heart attack.
I can still recall the first patient that I was responsible for. The very first patient I evaluated on Internal Medicine as a third year medical student. He was not much older than me, but at that point he had a much harder life. As he explained his symptoms to me and we did the examination, I found myself getting more and more anxious. I realized that he had a very serious illness that he was not going to recover from. I pulled all of the test results and x-rays together so I could present it in our team meeting in the morning. I could barely get the information out to my chief resident and attending. I was overcome with emotion. My voice cracked. I was tearing up. My head was spinning. I was focused on how unfair life was. He was a young guy, just like me with the usual hopes, dreams, and relationships that we all have and through no fault of his own, he had developed a terminal illness. I certainly wanted to help him, but there was nothing that could be done. That happens so frequently in medicine, using the most emotional definition of compassion would render most physicians nonfunctional. It tends to alter your focus. The focus has to be on what is happening right here and right now and not the unfairness of the process. The focus needs to be on the technical details or you can't provide competent care and tell people what they need to know. As I have gotten older, I have an image for the process of unpredictable disease and death. It reminds me of the war movie where the fleet is sunk and everyone is bobbing in the Pacific Ocean wearing life preservers. Suddenly the sharks appear and people start to die on a random basis. Whoever the sharks decide to kill. A random horrific process. That is my image.
It may explain the reaction of one of my attendings when I was a resident on a busy inpatient psychiatric unit. I was reading the description of one of our consultants to him and the consultant used the adjective "unfortunate" to describe all of the medical problems the patient had sustained. My attending glared at me and said: "Why is he unfortunate?" It seemed like an obvious descriptor to me. Anyone with all of these severe medical problems could be described as unfortunate, but I could not respond to him at the time. It seems to me if the sharks get you or there is a near miss, unfortunate in the bad luck sense may be a good description. He may have been thinking of another definition. But I think he was most likely giving me the message that it is best to not even recognize the random walk through life and the fact that the shark can eat you at any time. Without that element of denial, how can you function? How can you function as a physician?
After you have talked with thousands of people about their traumas and adversities, you realize that most people suffer. Personal biases make some people want to alleviate the suffering of some more than others. Nobody wants to see children suffer. There are some people who attract the ill wishes of others. They are generally unlikable or they have perpetrated some kind of shocking crime. There seems to be a likeability bias with compassion and that also makes it less useful for physicians. Physicians are obliged to perform competent medical care irrespective of how well the person is liked. There are often errors on the side of people who are very likeable. Sometimes physicians and medical staff get very attached to person based on their personality, physical characteristics, or demeanor. You may want to help that likeable person more, but that doesn't translate into whether you can or not.
If you are trained to render assistance, save lives when you can and alleviate suffering where does the compassion that you had before medical school go? Without invoking defense mechanisms it gets converted to other things that are adaptive in the profession. Empathy and technical skill are good examples. Empathy is probably a more accurate emotional appreciation of what is occurring in a person you are trying to help. It is focused on that person and their emotional state and if reflected back to that person they would agree with the observations. A better measure of burnout for physicians especially psychiatrists would be empathy fatigue rather than compassion fatigue. Seeing people as collections of symptoms and having no appreciation for the emotional side of their experience would be one example. Seeing patients as an endless stream of problems that you need to fix rather than unique individuals would be another. As the days get longer there are also the comparisons physicians make about how much time they spend taking care of others compared to how much time they spend with their families. As the family time gets shorter it may be harder to empathize with increasing numbers of patients.
Whether it is compassion fatigue or burnout, these seminars all seem to teach the same things. It is fashionable to refer to the skills as "tools". Mindfulness techniques, cognitive behavioral therapy. relaxation techniques, meditation, diet, sleep, and exercise are all parts of the "toolkit." Nobody ever seems to address the severely deteriorated work environment as a cause and ongoing factor. Productivity demands on physicians in terms of the number of patients seen, the amount of documentation that needs to be done and the other aspects of being a good corporate citizen are a recipe for burnout and that is probably the most common job scenario for physicians these days. Professional organizations seem to ignore that fact that if physicians are going to function the way they should and treat the whole person, a work environment without adequate time to talk with patients in one of the fast paths to burnout.
No amount of "tools" can reverse that.
George Dawson, MD, DFAPA
Supplementary 1: In talking with people over the years and trying to help them stay on the job, the most significant problem is unreasonable employers. People work in jobs where the job directly impacts their health. The best example is alternating shifts and never being able to establish a regular sleep routine. Hospitals are some of the worst offenders. They have adopted policies that allow them to tell nursing staff that they need to work "mandatory doubles" when there are shortages. The policies that have hospitalists working 7 days on and 7 days off are no better. I have interviewed hospitalists about their cognitive efficiency on day 6 and 7 and have been told that it generally plummets. They are taking twice as long to do the documentation and it is difficult to think. I was in a similar position one year when I was running a 20 bed inpatient service with assistance of a physician's assistant. I had to see everyone, everyday and managed both the medical and psychiatric diagnoses. When I decided to stop doing that, I was replaced by two full time psychiatrists and an internal medicine specialist to take care of all of the medical problems. Eventually those two psychiatrists felt it was too much work and a third psychiatrist was added to cover 4 of the 20 patients. The adverse effect of a business model on employee health that operates on personnel expenses cut to the bone can not be overemphasized. Hospitals and clinics will happily work medical staff to the point that it adversely impacts their health and lifestyle, adversely impacts their cognitive abilities at work, leads to burnout, and leaves them in a state where empathy is a thing of the past.
The only reason I quit running a 20 bed inpatient unit by myself was a colleague of mine who told me he did it for years - right up to the point he had his first heart attack.
Thursday, March 20, 2014
Public Sector Mental Health Continues to Be Squeezed Out Of Business
There was a story that shocked many in the local press earlier this week. A local mental health center serving about 3,000 people in five counties shut its doors, leaving nobody to fill that void. Although this appears to be scandalous news, it is really the logical progression of events that has been accurately described in E. Fuller Torrey's book. It is the logical result of federal and state governments selectively rationing mental health benefits and closing down both inpatient bed and outpatient treatment capacity.
People always ask me: "Well - what should an ideal community mental health center look like?" That is easy for me to answer because I was trained in community psychiatry, my first job out of residency was as the medical director of a community mental health center (CMHC) , and most of my career has been focused on helping patients who are largely in the public sector or certainly funded by those resources (Medicare/Medical Assistance). I know exactly what an ideal CMHC needs to run and provide services to a broad range of people who do not have access to metropolitan style mental health services. The vignettes provided in this article will also be addressed in the following points.
1. The backbone of any CMHC should be services that focus on people with disabling mental illnesses and helping them live independently. In the state where my original CMHC was located, statutes defined these conditions as schizophrenia, bipolar disorder, schizoaffective disorder, major depression, and borderline personality disorder. Adequate resources to treat those conditions generally means nursing and case management services that can meet with people in their homes and in the community. In the teams that I worked with over 20 years ago we also had a vocational rehabilitation component and we worked with a number of physicians and specialists to address medical problems. In any treatment setting where a CMHC is responsible for treating all public patients over a county wide catchment area, there is of necessity a legal component. That is typically focused on involuntary treatment like civil commitment, court ordered medications, guardianships, conservatorships and protective placement. Depending on the size of the county it can also involve competency assessments for ability to proceed to a court hearing based on concerns about mental illness.
2. A community trained psychiatrist with medical skills. The psychiatrist involved should enjoy working with people with people who have severe mental illnesses and medical comorbidity. The legal component of services means that this person also needs to be comfortable doing the necessary exams and court testimony. Medical and neurological illnesses need to be recognized and treated. In CMHC settings the psychiatrist generally has much more information available about the health of his or her patients and they know how to interview people to get it. When I was a medical director I also provided consultation to nursing homes, hospital consultations, and I would also travel to patient homes with case managers to provide consultation in that setting. A lot depends on geography and distances to the other facilities needing consultation.
3. Psychotherapists are critical to the functioning of a CMHC. It has been interesting to watch the government and managed care companies ration psychotherapy services as much as they ration access to psychiatrists. Correct me if I am wrong but as far as I know there are no HMOs or MCOs offering standard research based psychotherapies for psychiatric diagnoses. At the max, usually 2 or 3 "crisis counseling" sessions. In some cases a generic dialectical behavior therapy (DBT) group where many people with personality disorders end up because more specific therapy is unavailable. CMHCs could be leaders in the implementation of computer based therapies, and the argument against that would be the lack of information technology departments. The argument in support of this would be the fact that all counties across the state could share the same resource. With today's tech, it would be easily scalable to support anyone who needed it. It would be inexpensive, effective and a good way to not dilute the psychotherapy resources of the clinic. The other major change int he past two decades has been the focus on psychotherapy for people with severe mental illnesses. That should be a critical part of any CMHC function.
4. Addiction treatment - many communities have more resources available outside of the CMHC for assessment and treatment or referral of addictions. The CMHC resources need to be more focused on the issue of co-occurring disorders and probably chronic pain and co-occurring disorders. This would be another opportunity for networking all of the CMHCs in a state to assure a standard of assessment, share treatment resources, consult on specific cases and assure that there is no deterioration in prescriber standards with regard to potentially addictive medications.
5. Crisis intervention services - 24/7 availability is necessary to provide acute evaluations but more importantly to resolve crises in patients who are well known to treatment teams. Ity reduces the likelihood of unnecessary hospitalizations when there are staff person available who know the person in crisis very well. It is much more efficient and patient centered than sending a person to an emergency department and asking them to start over there with professionals who do not know them.
In the CMHC I worked in we had a catchment area of about 100,000 people spread over a large rural county. We had a little over 100 patients in our community support programs for the severely disabled. We we staffed by 1 psychiatrist, 2 psychologists, 4 social workers, 1 occupational therapist, 4 psychotherapists, 1 RN, and 2 LPNs.
The progression noted in this article is very clear and it has been replicated thousands of times across the US. Shut down the large hospitals and tell people that treatment will be available in the communities near their homes. Then shut down community treatment. You will notice that officials make it seem like this is some kind of mystery.
“We’re so tight in [psychiatric] beds that any change in the delivery system impacts the whole system,” said Assistant Human Services Commissioner David Hartford. “The agencies need to reorganize to get people the care they need.”
People always ask me: "Well - what should an ideal community mental health center look like?" That is easy for me to answer because I was trained in community psychiatry, my first job out of residency was as the medical director of a community mental health center (CMHC) , and most of my career has been focused on helping patients who are largely in the public sector or certainly funded by those resources (Medicare/Medical Assistance). I know exactly what an ideal CMHC needs to run and provide services to a broad range of people who do not have access to metropolitan style mental health services. The vignettes provided in this article will also be addressed in the following points.
1. The backbone of any CMHC should be services that focus on people with disabling mental illnesses and helping them live independently. In the state where my original CMHC was located, statutes defined these conditions as schizophrenia, bipolar disorder, schizoaffective disorder, major depression, and borderline personality disorder. Adequate resources to treat those conditions generally means nursing and case management services that can meet with people in their homes and in the community. In the teams that I worked with over 20 years ago we also had a vocational rehabilitation component and we worked with a number of physicians and specialists to address medical problems. In any treatment setting where a CMHC is responsible for treating all public patients over a county wide catchment area, there is of necessity a legal component. That is typically focused on involuntary treatment like civil commitment, court ordered medications, guardianships, conservatorships and protective placement. Depending on the size of the county it can also involve competency assessments for ability to proceed to a court hearing based on concerns about mental illness.
2. A community trained psychiatrist with medical skills. The psychiatrist involved should enjoy working with people with people who have severe mental illnesses and medical comorbidity. The legal component of services means that this person also needs to be comfortable doing the necessary exams and court testimony. Medical and neurological illnesses need to be recognized and treated. In CMHC settings the psychiatrist generally has much more information available about the health of his or her patients and they know how to interview people to get it. When I was a medical director I also provided consultation to nursing homes, hospital consultations, and I would also travel to patient homes with case managers to provide consultation in that setting. A lot depends on geography and distances to the other facilities needing consultation.
3. Psychotherapists are critical to the functioning of a CMHC. It has been interesting to watch the government and managed care companies ration psychotherapy services as much as they ration access to psychiatrists. Correct me if I am wrong but as far as I know there are no HMOs or MCOs offering standard research based psychotherapies for psychiatric diagnoses. At the max, usually 2 or 3 "crisis counseling" sessions. In some cases a generic dialectical behavior therapy (DBT) group where many people with personality disorders end up because more specific therapy is unavailable. CMHCs could be leaders in the implementation of computer based therapies, and the argument against that would be the lack of information technology departments. The argument in support of this would be the fact that all counties across the state could share the same resource. With today's tech, it would be easily scalable to support anyone who needed it. It would be inexpensive, effective and a good way to not dilute the psychotherapy resources of the clinic. The other major change int he past two decades has been the focus on psychotherapy for people with severe mental illnesses. That should be a critical part of any CMHC function.
4. Addiction treatment - many communities have more resources available outside of the CMHC for assessment and treatment or referral of addictions. The CMHC resources need to be more focused on the issue of co-occurring disorders and probably chronic pain and co-occurring disorders. This would be another opportunity for networking all of the CMHCs in a state to assure a standard of assessment, share treatment resources, consult on specific cases and assure that there is no deterioration in prescriber standards with regard to potentially addictive medications.
5. Crisis intervention services - 24/7 availability is necessary to provide acute evaluations but more importantly to resolve crises in patients who are well known to treatment teams. Ity reduces the likelihood of unnecessary hospitalizations when there are staff person available who know the person in crisis very well. It is much more efficient and patient centered than sending a person to an emergency department and asking them to start over there with professionals who do not know them.
In the CMHC I worked in we had a catchment area of about 100,000 people spread over a large rural county. We had a little over 100 patients in our community support programs for the severely disabled. We we staffed by 1 psychiatrist, 2 psychologists, 4 social workers, 1 occupational therapist, 4 psychotherapists, 1 RN, and 2 LPNs.
The progression noted in this article is very clear and it has been replicated thousands of times across the US. Shut down the large hospitals and tell people that treatment will be available in the communities near their homes. Then shut down community treatment. You will notice that officials make it seem like this is some kind of mystery.
“We’re so tight in [psychiatric] beds that any change in the delivery system impacts the whole system,” said Assistant Human Services Commissioner David Hartford. “The agencies need to reorganize to get people the care they need.”
Sorry Commissioner but in case you didn't notice we are not talking about beds anymore. All of the people involved here were living at home in their own beds. Agency "reorganization" is not an option. There are no agencies anymore and one that was providing a valuable service was just shut down. The problem here is very clear, cost shifting by managed care and defunding by the state. Corporate welfare in the form of a carve-out for psychiatric services. Keep in mind that when the comprehensive and humanistic approach to community treatment is lost, the only alternative is going in to a large managed care clinic where the appointments are scheduled every 15-20 minutes, the focus is on a prescription, and the only thing the doctor knows about what is going on is exchanged in that visit and recorded in the electronic health record. That is frequently a symptom checklist.
I guess there is always the psychiatric hospital of last resort - the county jail. At least until the Sheriff's department goes broke.
George Dawson, MD, DFAPA
Christopher Snowbeck. Crisis mental health provider closes; 5 counties scrambling. TwinCities.com St. Paul Pioneer Press. March 18, 2014.
Chris Serres. Minn. mental health center shuts down, stranding thousands. Minneapolis StarTribune. March 17, 2014.
Supplementary 1: I e-mailed the author of the first article Mr. Serres to inquire about the recently released state report that he refers to in the article and got no response. As far as I can tell it may be the "Health Services in State Correctional Facilities Report" available at this site. The concerning highlights include the fact that there are units that provide intensive nursing and mental health services. About 33% (67,456) of all of the health services encounters with staff are for mental health purposes. That translates to 28% of the offenders receiving mental health services. At some point in their stay 32% are diagnosed with a "serious and persistent mental illness" as defined by state statute. The report provides an interesting overview of how mental health services are provided in Minnesota prisons and the special problems involved in treating mentally ill offenders.
Supplementary 2: According to Minnesota Statutes 2013, 245.462, subd. 20(c)(4)(i), states that a person has serious and persistent mental illness if he or she is an adult and “has a diagnosis of schizophrenia, bipolar disorder, major depression, schizoaffective disorder, or borderline personality disorder.”
George Dawson, MD, DFAPA
Christopher Snowbeck. Crisis mental health provider closes; 5 counties scrambling. TwinCities.com St. Paul Pioneer Press. March 18, 2014.
Chris Serres. Minn. mental health center shuts down, stranding thousands. Minneapolis StarTribune. March 17, 2014.
Supplementary 1: I e-mailed the author of the first article Mr. Serres to inquire about the recently released state report that he refers to in the article and got no response. As far as I can tell it may be the "Health Services in State Correctional Facilities Report" available at this site. The concerning highlights include the fact that there are units that provide intensive nursing and mental health services. About 33% (67,456) of all of the health services encounters with staff are for mental health purposes. That translates to 28% of the offenders receiving mental health services. At some point in their stay 32% are diagnosed with a "serious and persistent mental illness" as defined by state statute. The report provides an interesting overview of how mental health services are provided in Minnesota prisons and the special problems involved in treating mentally ill offenders.
Supplementary 2: According to Minnesota Statutes 2013, 245.462, subd. 20(c)(4)(i), states that a person has serious and persistent mental illness if he or she is an adult and “has a diagnosis of schizophrenia, bipolar disorder, major depression, schizoaffective disorder, or borderline personality disorder.”
Subscribe to:
Posts (Atom)