I was buoyed to see this line as the title of a financial blog today: "Coming Corporate Control of Medicine Will Throw Patients Under the Bus". You don't usually see that level of insight into what is going on in medicine from financial people who have usually bought the "cost effectiveness" dogma, even at a time where middlemen are siphoning off hundreds of billions of dollars from the direct provision of health care and producing an inferior product. I will say it for the thousandth time - what other industry can make money by selling you a rationed product and denying your access to that product? Can you imagine what the automobile or cell phone market would look like with that guiding principle?
The article is focused on two critical issues-physician management by people with no medical experience and the message from the top. The first part of the article discusses the situation of a pediatrician who had successfully managed a clinic but found herself being managed by a non-physician who told her that she either had to see very complex patients in a shorter period of time or not see them at all. The second part of the article focuses on a blog post where a CEO/physician for a managed care company flat out encourages physicians to get rid of difficult patients to improve their managed care style performance measures.
The blogger in this case is Yves Smith. I have been reading her blog for years. She wrote the book Econned and takes a generally skeptical view of that way that financial markets are regulated and run. I have seen her do commentary on some financial television but infrequently. I would tend to see her commentary as legitimate criticism and welcome in the area of physician and health care management. As a blogger she is highly successful. This post alone has about 40 pages of commentary.
In this article she has some additional comments about what physicians face in the assembly line of today's managed care environment:
"As an aside, it's hard to stress enough that this sort of demoralizing micromanagement an unwillingness to listen and learn from workers is a weird shortcoming of management American style. And it has been weirdly airbrushed out of the media."
I can't agree more with the second comment in particular. The American public gets a glimpse of how their health care management occurs only when Michael Moore makes a movie about it or they are confronted face to face with an impossible situation. That happens all of the time in psychiatry with restrictions on treatment to the point that it seems like treatment has never occurred. To get that accomplished takes both micromanagement of physicians and a general management style that greatly emphasizes profit margin over patients. At the public relations level, physician opinion especially physician dissent is not tolerated. The personal experience of the physicians in these systems is considered the property of the organization. Any public disclosure of the severe shortcomings can be ruthlessly suppressed either by firing or a series of political maneuvers designed to force resignation at some point.
There is a divergence of medical and corporate culture at the level of disclosure of errors or wrongdoing. For most of my professional life I have been in monthly conferences - some type of mortality-morbidity conferences where real or potential errors were discussed on a department wide basis. I don't think that happens in the corporate world. I think that errors in the corporate world are acknowledged if they are widely known and there is an emphasis on public relations and maintaining an almost unrealistic positive light on the company. That has been most evident in the past decade with an abundance of managed care public relations. Wherever I turn it seems like I come across a hospital or clinic that is proclaiming themselves as the "best" - usually in the country. That kind of advertising by physicians was widely viewed as unethical by state medical boards. These ratings are usually based on a few process parameters that can be actively "managed". Contrary to what health care management tells you the quality of any hospital or clinic depends on the quality of the physicians working there and the level of autonomy they have in their medical decision making.
You can have the best surgeons, internists, or psychiatrists in the world and if they are managed to see as many patients as possible and provide the care that will provide the best profit margin for the company - their medical and surgical care will not be appreciably different from a mediocre staff.
I wrote a piece several years ago about an informed approach to managing knowledge workers that originated with management guru Peter Drucker. The details can be found in the original piece in this newsletter (page 3) and a earlier posts on this blog. Everywhere I look in health care we are at the opposite pole from Drucker. Managers are generally far too authoritarian in dealing with physicians especially in cases where (like the Yves Smith blog post) - the mangers know far less than the physicians. This managerial style is also disruptive. Many health care managers think that they can implement any idea they wake up with that morning if they accompany it with enough "Change is good" or "Cost effective" rhetoric. All of this micromanagement and mismanagement illustrates that Dilbert has changed professions. He is currently wearing a white lab coat.
The other bad news of course is that corporate control of medicine is not coming - it has been here for years. In the case of psychiatry it has been here for 30 years. Anyone who wants to see how corporate control of medicine changes things only has to look at the state of current psychiatric services or their "shortage" for a lesson.
George Dawson, MD, DFAPA
Saturday, May 18, 2013
Saturday, May 11, 2013
The Model of Psychiatric Care for the Future
The Psychiatric News came out with an article yesterday that is critically important for all psychiatrists to read. It reveals the American Psychiatric Association (APA) thinking about the future role of psychiatrists and the model of care that they are promoting. The diagram in this article titled "Integrated Care Relies on Team Approach, Consultant Role for Psychiatrists" is a critical read because it shows what is basically a managed care paradigm for marginalizing psychiatrists. There is is a "BHP/Care Manager" between the psychiatrist and the patient. This is a popular managed care approach to having "care/case managers" making discharge decisions for psychiatrists providing inpatient care. For anyone with professional expertise and direct responsibility to patients it is unacceptable.
The main reason that psychiatry has been marginalized is that all of the knowledge in the membership about what we do and the value we add is ignored in the face of special interest research. The research that forms the "evidence base" for our marginalization in the Psych News article is a good example. There is a long history of similar studies have been published to sell the managed care industry. I can come up with a pharmacoepidemiology study from 20 years ago that show that putting everyone in a primary care clinic on fluoxetine saves money on as many parameters as this article claims for integrated care. Instead of confronting that and saying: "You know psychiatrists do a lot more than that" - the APA seems to accept it and think that integrated care is some big deal. From the diagram it is clear to me that integrated care is just the latest head of the managed care hydra.
The other aspect of the article is the omnipresent "cost savings" rhetoric. Professional organizations have bought this hook line and sinker and seem obliged to include that nonsense in policy about the future of their speciality. The difference of course is that in the last two decades, Cardiology has built out a trillion dollar infrastructure being "cost effective" and we are now treating people in jails who should be in psychiatric hospitals, we have few functional detox facilities and have minimal resources to help disabled patients in the community.
What we need here is a reality based characterization of what psychiatrists do and on average it is a lot more than sitting in a primary care clinic and advising primary care docs about what to do if they can't get their depression ratings (PHQ-9 scores) headed in the right direction. Its is just a matter of time before everybody who thinks they can make a psychiatric diagnosis by reading the DSM will think they can treat depression by reading an algorithm and psychiatry slips off the next managed care diagram. Nobody will realize they just eliminated not just a psychiatrist but the person in the clinic who knew the most Neurology as well.
If we are going to promote any image of ourselves and an image that current trainees can be excited about, it should be a larger than life psychiatric multispeciality clinic and a group of psychiatrists who can cover the gamut of care. That is consistent with the psychiatrist of the future that Thomas Insel, MD has talked about, and it takes a page from some of our specialist colleagues like Radiologists and Anesthesiologists.
They realized a long time ago that you are not going to get a fair deal bartering away your expertise for the sake of doing business.
George Dawson, MD. DFAPA
Mark Moran. Report on Health Care Reform Focuses on Psychiatrists' Role. Psychiatric News May 3, 2013.
Sunday, May 5, 2013
Using A Civil War Law to Intimidate Physicians
I thought I would post this latest iteration of how managed care organizations (MCOs) and their proxies in the pharmacy benefit manager (PBM) industry are intimidating physicians into not prescribing a specific medication for you. At some point these companies started to attach a reference to the False Claims Act, along with the usual forms they expect doctors to fill out so that you can get your prescription filled. Intimidating physicians has always been a tactic to try to slow doctors down or stop them in their tracks. Delaying and stopping doctors from writing prescriptions is money in the pocket of any PBM or MCO. Intimidating physicians is also useful because it has a demonstrated effect on their behavior. It causes them to undercode or bill for less service than they actually provided and it dates back to the 1990s when the FBI was used change the billing behavior of an entire generation of teaching physicians under the threat of large scale paybacks for "fraud" or RICO actions and the threat of imprisonment. I have never seen an estimate of the total amount of money "saved" (as in removed from physicians) and time wasted based on these political ideas, but it would not surprise me if it was hundreds of billions of dollars. I know it forced me not to teach residents for over a decade. I could see no point in needing to generate a daily note that was identical to my residents' notes and they logically found it offensive.
So we have the issue of "prior authorization". You used to get a prescription from your doctor, take it to the pharmacy, and get it filled. In the 1990s HMOs and MCOs decided they knew more than doctors and they would adopt some sweeping measures to "reform" prescribing practices. In some of the areas it made sense at the level of clinic or hospital based Pharmacy and Therapeutics (P&T) Committees. Certain drugs are so specialized (eg. chemotherapy agents) that only certain physicians should prescribe them. There has been a two decades long problem with antibiotic over prescribing and there are typically ongoing initiatives to deal with that problem. I have not been on a P&T Committee for over three years, but I can't imagine there is nothing currently being done to curb opioid painkiller overprescribing. There are definite reasons for intervening with prescribers on a scientific basis. But at some point prior authorization became much more than that and some of the assumptions (like all SSRIs are alike) are not valid. To make matters worse, the pharmacy arm of managed care companies (the PBMs) were now asking for prior authorizations on generic drugs. Or they were asking for repeat authorizations if the prescriber changed or the patient was hospitalized and the prescription stayed the same. These same PBMS found that the same rules did not apply to themselves. They could frequently make deals with hospital that would involve the bundling of one medication with the same medication form the same company and they could make money off that. PBMs had become a multibillion dollar business.
The hassle of filling out forms and making many phone calls in order to assure that a prescription is completed is more than an annoyance. It removes billions of dollars of resources from the provision of medical care. One study estimated that the cost for American physicians to deal with insurance companies was $82,975 per physician or about four times higher than their Canadian counterparts. That amounts to $27.6 billion nationwide. That is a lot of medical care and the time jumping through hoops is never reimbursed by MCOs or PBMs. An estimate of the losses to the treatment side for billing practices alone is about $7 billion.
The political aspects of this intrusion of business into medical practice is instructive. Physicians are notoriously inept when it comes to politics and there is no clearer example than drug prior authorization. What other business in the United States has to provide that level of free work in addition to the primary work in order to be reimbursed. Do other professionals like lawyers need to waste this amount of time? I sat through a meeting at one point where the debate was whether we could influence the length of a drug prior authorization form and get it down to two pages instead of five. The consensus at the time was that there were probably federal rules that would not allow the form to be "streamlined" to two pages!
So now we have the streamlined form with a 14 page federal statute affixed to it. Reading through the statute and figuring out what it means takes an attorney. But every doctor who sees this knows what it means. Don't rock the boat. Don't question this government backed, big business policy that is guaranteed to waste your time and put more money into the pocket of the insurance industry. And by the way, there is no guarantee that your patient will get the medication that you think they need, even if you jump through all of these hoops.
That is the state of health care in America today and it may be why you are standing in a pharmacy waiting to get your prescription filled. It also may be why your doctor looks exhausted.
George Dawson, MD, DFAPA
Morra D, Nicholson S, Levinson W, Gans DN, Hammons T, Casalino LP. US physician practices versus Canadians: spending nearly four times as much money interacting with payers. Health Aff (Millwood). 2011 Aug;30(8):1443-50. doi: 10.1377/hlthaff.2010.0893. Epub 2011 Aug 3. PubMed PMID: 21813866.
So we have the issue of "prior authorization". You used to get a prescription from your doctor, take it to the pharmacy, and get it filled. In the 1990s HMOs and MCOs decided they knew more than doctors and they would adopt some sweeping measures to "reform" prescribing practices. In some of the areas it made sense at the level of clinic or hospital based Pharmacy and Therapeutics (P&T) Committees. Certain drugs are so specialized (eg. chemotherapy agents) that only certain physicians should prescribe them. There has been a two decades long problem with antibiotic over prescribing and there are typically ongoing initiatives to deal with that problem. I have not been on a P&T Committee for over three years, but I can't imagine there is nothing currently being done to curb opioid painkiller overprescribing. There are definite reasons for intervening with prescribers on a scientific basis. But at some point prior authorization became much more than that and some of the assumptions (like all SSRIs are alike) are not valid. To make matters worse, the pharmacy arm of managed care companies (the PBMs) were now asking for prior authorizations on generic drugs. Or they were asking for repeat authorizations if the prescriber changed or the patient was hospitalized and the prescription stayed the same. These same PBMS found that the same rules did not apply to themselves. They could frequently make deals with hospital that would involve the bundling of one medication with the same medication form the same company and they could make money off that. PBMs had become a multibillion dollar business.
The hassle of filling out forms and making many phone calls in order to assure that a prescription is completed is more than an annoyance. It removes billions of dollars of resources from the provision of medical care. One study estimated that the cost for American physicians to deal with insurance companies was $82,975 per physician or about four times higher than their Canadian counterparts. That amounts to $27.6 billion nationwide. That is a lot of medical care and the time jumping through hoops is never reimbursed by MCOs or PBMs. An estimate of the losses to the treatment side for billing practices alone is about $7 billion.
The political aspects of this intrusion of business into medical practice is instructive. Physicians are notoriously inept when it comes to politics and there is no clearer example than drug prior authorization. What other business in the United States has to provide that level of free work in addition to the primary work in order to be reimbursed. Do other professionals like lawyers need to waste this amount of time? I sat through a meeting at one point where the debate was whether we could influence the length of a drug prior authorization form and get it down to two pages instead of five. The consensus at the time was that there were probably federal rules that would not allow the form to be "streamlined" to two pages!
So now we have the streamlined form with a 14 page federal statute affixed to it. Reading through the statute and figuring out what it means takes an attorney. But every doctor who sees this knows what it means. Don't rock the boat. Don't question this government backed, big business policy that is guaranteed to waste your time and put more money into the pocket of the insurance industry. And by the way, there is no guarantee that your patient will get the medication that you think they need, even if you jump through all of these hoops.
That is the state of health care in America today and it may be why you are standing in a pharmacy waiting to get your prescription filled. It also may be why your doctor looks exhausted.
George Dawson, MD, DFAPA
Morra D, Nicholson S, Levinson W, Gans DN, Hammons T, Casalino LP. US physician practices versus Canadians: spending nearly four times as much money interacting with payers. Health Aff (Millwood). 2011 Aug;30(8):1443-50. doi: 10.1377/hlthaff.2010.0893. Epub 2011 Aug 3. PubMed PMID: 21813866.
Even more DSM bashing - is it a fever pitch yet?
Just when you think you have seen it all, you run into an article like this one in The Atlantic. A psychotherapist with a long antipsychiatry monologue. It is written in interview format with psychotherapist Gary Greenberg as the discussant. I thought it was interesting because the title describes this diatribe as the "real problems" with psychiatry. Of course what he writes about has nothing to do with the real problems that specifically are the rationing and decimation of psychiatric services by managed care companies and the government. The entire article can be discredited on a point by point basis but I will focus on a few broad brush strokes.
The author here spins a tale that the entire impetus for a diagnostic manual and a biomedical orientation for psychiatry is strictly political in nature and it has to do with wanting to establish credibility with the rest of medicine. That is quite a revision of history. Psychiatry pretty much exists now because psychiatrists would take care of the problems that nobody else wanted to. I have immediate credibility when another physician is seeing a person with a mental illness, they don't know what to do about it, and I do. It is less clear today, but psychiatry professional organizations were asylum focused and the goal was to treat people in asylums initially and then figure out a way to get them back home. Part of the psychiatric nosology was based on the people who would get out of asylums at some point and those who did not. The credibility of psychiatry has nothing to do with a diagnostic manual. It has to do with the fact that psychiatrists have a history of treating people with serious problems and helping them get well. There is no discussion of how the numbers of people institutionalized in the 1950s and 1960s fell to the levels of current European levels as a result of psychiatric intervention that included the use of new medications but also a community psychiatry movement that was socially based. (see Harcourt Figure II.2)
The author uses the idea of "chemical imbalance" rhetorically here as further proof that psychiatrists are using a false premise for political purposes. He presumes to tell his readers that during the time he is giving the interview there is some psychiatrist out there using the term chemical imbalance to convince a patient to take antidepressants. Since I have never used that term and generally discourage it when patients bring it up, I wonder if he is right. Any psychiatrist trained in the past three decades knows the situation is much more complex than that. Eric Kandel describes the situation very well in his 1979 classic article on "Psychotherapy and the Single Synapse". Any antipsychiatrist using "chemical imbalance" against psychiatry in a rhetorical manner suggests that there is no biomedical basis for mental disorders. There should be nobody out here who believes that is true and in fact this article acknowledges that.
The basic position here is to deny that anything psychiatric exists. Psychiatrists don't know what they are doing. Psychiatrists are driven by the conflict of interest that nets them "hundreds of millions of dollars". He doesn't mention how much money he makes as an outspoken critic of psychiatry. He tries to outflank his rhetoric by suggesting any psychiatrists who disagrees with him and suggests that it is typical antipsychiatry jargon is "diagnosing him". He doesn't mention the fact that antipsychiatry movements are studied and classified by philosophers.
I think the most revealing part of this "interview" is that it appears to be orchestrated to enhance the author's rhetoric. The evidence for that is the question about "drapetomania" and implying that has something to do with coming up with DSM diagnoses and the decision to drop homosexuality as a diagnostic category. That is more than a stretch that is a clear distortion and of course the question is where the interviewer comes up with a question about "drapetomania". I wonder how that happened?
This column is an excellent ad for the author's antipsychiatry work. Apart from that it contains contains the standard "chemical imbalance" and psychiatric disorders are not "real illnesses". To that he adds the conflicting positions of saying there appear to be biological correlates of mental disorders but they would never correlate with an existing diagnosis and the idea of a chemical imbalance metaphor is nonsense. He uses colorful language to boost his rhetoric: "They'll (those wacky psychiatrists - my clarification) bob and weave, talk about the "living document," and unleash their line of bullshit."
His conclusory paragraph and the idea to "take the thing (DSM) away from them" has been a common refrain from the DSM critics. In fact as I have repeatedly pointed out, there is nothing to stop any other organization from coming up with a competing document. In fact, sitting on my shelf right now (next to DSM-IV) is a reference called the Psychodynamic Diagnostic Manual. It is listed as a collaborative effort of six different organizations of mental health professionals. It was published 12 years after the last edition of the DSM - it is newer. I have texts written by several of the collaborators of this volume. When I talk with psychiatrists from the east coast, they frequently ask me about whether or not I am familiar with the volume. My point here is that if the author's contentions about the reality basis of DSM diagnoses are correct, it should be very easy to come up with a different system. I encourage anyone or group of people to develop their own diagnostic system and compete with the DSM.
So the last minute attacks on psychiatry with the release of the DSM seem to be at a fever pitch. The myth of the psychiatric bogeyman is alive and well. Add The Atlantic to the list of uncritical critics of psychiatry.
George Dawson, MD, DFAPA
1. Hope Reese. The Real Problems with Psychiatry. The Atlantic. May 2, 2013.
2. Bernard E. Harcourt. From the asylum to the prison: rethinking the incarceration revolution. The Law School, University of Chicago, 2007.
3. Psychodynamic Diagnostic Manual (PDM). A collaborative effort of the American Psychoanalytic Association, International Psychoanalytic Association, Division of Psychoanalysis (38) of the American Psychological Association, American Academy of Psychoanalysis and Dynamic Psychiatry, National Membership Committee on Psychoanalysis in Clinical Social Work. Published by the Alliance of Psychoanalytic Organizations. Silver Spring, MD (2006).
4. Kandel ER. Psychotherapy and the single synapse. The impact of psychiatric thought on neurobiologic research. N Engl J Med. 1979 Nov 8;301(19):1028-37. PubMed PMID: 40128.
The author here spins a tale that the entire impetus for a diagnostic manual and a biomedical orientation for psychiatry is strictly political in nature and it has to do with wanting to establish credibility with the rest of medicine. That is quite a revision of history. Psychiatry pretty much exists now because psychiatrists would take care of the problems that nobody else wanted to. I have immediate credibility when another physician is seeing a person with a mental illness, they don't know what to do about it, and I do. It is less clear today, but psychiatry professional organizations were asylum focused and the goal was to treat people in asylums initially and then figure out a way to get them back home. Part of the psychiatric nosology was based on the people who would get out of asylums at some point and those who did not. The credibility of psychiatry has nothing to do with a diagnostic manual. It has to do with the fact that psychiatrists have a history of treating people with serious problems and helping them get well. There is no discussion of how the numbers of people institutionalized in the 1950s and 1960s fell to the levels of current European levels as a result of psychiatric intervention that included the use of new medications but also a community psychiatry movement that was socially based. (see Harcourt Figure II.2)
The author uses the idea of "chemical imbalance" rhetorically here as further proof that psychiatrists are using a false premise for political purposes. He presumes to tell his readers that during the time he is giving the interview there is some psychiatrist out there using the term chemical imbalance to convince a patient to take antidepressants. Since I have never used that term and generally discourage it when patients bring it up, I wonder if he is right. Any psychiatrist trained in the past three decades knows the situation is much more complex than that. Eric Kandel describes the situation very well in his 1979 classic article on "Psychotherapy and the Single Synapse". Any antipsychiatrist using "chemical imbalance" against psychiatry in a rhetorical manner suggests that there is no biomedical basis for mental disorders. There should be nobody out here who believes that is true and in fact this article acknowledges that.
The basic position here is to deny that anything psychiatric exists. Psychiatrists don't know what they are doing. Psychiatrists are driven by the conflict of interest that nets them "hundreds of millions of dollars". He doesn't mention how much money he makes as an outspoken critic of psychiatry. He tries to outflank his rhetoric by suggesting any psychiatrists who disagrees with him and suggests that it is typical antipsychiatry jargon is "diagnosing him". He doesn't mention the fact that antipsychiatry movements are studied and classified by philosophers.
I think the most revealing part of this "interview" is that it appears to be orchestrated to enhance the author's rhetoric. The evidence for that is the question about "drapetomania" and implying that has something to do with coming up with DSM diagnoses and the decision to drop homosexuality as a diagnostic category. That is more than a stretch that is a clear distortion and of course the question is where the interviewer comes up with a question about "drapetomania". I wonder how that happened?
This column is an excellent ad for the author's antipsychiatry work. Apart from that it contains contains the standard "chemical imbalance" and psychiatric disorders are not "real illnesses". To that he adds the conflicting positions of saying there appear to be biological correlates of mental disorders but they would never correlate with an existing diagnosis and the idea of a chemical imbalance metaphor is nonsense. He uses colorful language to boost his rhetoric: "They'll (those wacky psychiatrists - my clarification) bob and weave, talk about the "living document," and unleash their line of bullshit."
His conclusory paragraph and the idea to "take the thing (DSM) away from them" has been a common refrain from the DSM critics. In fact as I have repeatedly pointed out, there is nothing to stop any other organization from coming up with a competing document. In fact, sitting on my shelf right now (next to DSM-IV) is a reference called the Psychodynamic Diagnostic Manual. It is listed as a collaborative effort of six different organizations of mental health professionals. It was published 12 years after the last edition of the DSM - it is newer. I have texts written by several of the collaborators of this volume. When I talk with psychiatrists from the east coast, they frequently ask me about whether or not I am familiar with the volume. My point here is that if the author's contentions about the reality basis of DSM diagnoses are correct, it should be very easy to come up with a different system. I encourage anyone or group of people to develop their own diagnostic system and compete with the DSM.
So the last minute attacks on psychiatry with the release of the DSM seem to be at a fever pitch. The myth of the psychiatric bogeyman is alive and well. Add The Atlantic to the list of uncritical critics of psychiatry.
George Dawson, MD, DFAPA
1. Hope Reese. The Real Problems with Psychiatry. The Atlantic. May 2, 2013.
2. Bernard E. Harcourt. From the asylum to the prison: rethinking the incarceration revolution. The Law School, University of Chicago, 2007.
3. Psychodynamic Diagnostic Manual (PDM). A collaborative effort of the American Psychoanalytic Association, International Psychoanalytic Association, Division of Psychoanalysis (38) of the American Psychological Association, American Academy of Psychoanalysis and Dynamic Psychiatry, National Membership Committee on Psychoanalysis in Clinical Social Work. Published by the Alliance of Psychoanalytic Organizations. Silver Spring, MD (2006).
4. Kandel ER. Psychotherapy and the single synapse. The impact of psychiatric thought on neurobiologic research. N Engl J Med. 1979 Nov 8;301(19):1028-37. PubMed PMID: 40128.
Friday, May 3, 2013
Greyhound Therapy - suddenly wrong?
Without any disrespect to the famous long haul bus company, I wanted to comment on this story posted from the APA's Facebook feed. It is a story about a man, James Brown who was discharged unchanged from a psychiatric hospital in the state of Nevada and sent to California via bus with minimal resources. That was the discharge plan. Watch the actual clip to see what happened and watch the concerned discussion by the public official in this case. Diane Sawyer, et al were outraged. How could this possibly happen? How often does this happen? There was a happy ending to this story but how often does it go horribly wrong?
When I looked at this clip I was amazed for a couple of reasons. First off, it was on the APA's Facebook feed with a comment by the Medical Director. Without going into all of the details that I have posted so far on this blog, I will say that it is about time and leave it at that. The fact that nothing has been said to this point is also reflected in my second point and that is - this has been going on for over 20 years! Every place in this country with a major psychiatric hospital has been the recipient or point of origin for discharges by bus to another state. It is so common that I used to refer to it as Greyhound Therapy with my coworkers and everybody knew exactly what I was talking about.
At first blush putting somebody with a severe mental illness on a bus and sending them to another state - sometimes across a number of states seems inhumane. In some cases, the person himself may insist but if we are talking about the instance where the person is mentally ill and cannot care for themselves - I agree completely. It is inhumane and not really ethical from the standpoint of a physician. So how does it occur?
It basically occurs by taking a business approach to psychiatry. Rationing and cost center management coalesce into the perfect mechanism to get people out of psychiatric hospitals when they are at their most vulnerable. I have posted many times the concept of getting people out of the hospital before the hospital loses money on a DRG payment. That is generally within 3 - 5 days. That period of time is well below any acceptable time period necessary for the evaluation or treatment of severe psychiatric problems. Everyone agrees that hospital treatment like outpatient treatment means treating people with medications and in hospitals the medications are generally added faster and at much larger doses than in outpatient settings. Five days does not allow for any changes if there are side effects or inadequate treatment response or comorbid medical complications that may crop up. So doctors don't want to use this approach. Who does?
The main drivers are managed care companies and the government agencies that promote these tactics. So the psychiatrist doesn't want to discharge the patient in 5 days - get a managed care reviewer to say that the hospital stay is no longer "medically necessary" and will not be paid for. If the attending psychiatrist doesn't like that decision - he or she can appeal it to another reviewer within the same company. How do you think that will turn out? Of course you can always appeal to the state - right? The state has managed care rights embedded in their statutes. The appeal goes through a commission that is often staffed by insurance industry insiders and they are not there to advocate for patients or their physicians. In the case of psychiatrists who are unfortunate enough to work for managed care companies, they may find their discharge decisions commandeered by case managers and a medical director whose only jobs are to get people out of the hospital as soon as possible. Disagree with them and you might hear that the medical director will come down and take over discharging the patient. Or you might find yourself fighting a never ending series of political battles for not being a "team player." The discharge team may decide to do an end run around you entirely and that could involve putting somebody on a bus.
What about the psychiatrists working in these settings? Why don't they ever speak up? It should be obvious from the preceding paragraph that it could result in getting fired or forced out in one way or another. Every organization these days has policies that stifle disclosure from physicians working in those companies. All of the communication needs to go though an administrator who has the company's best interest at heart. The interest of the patient, the physician, and the physician-patient relationship is not a priority. Making money is the priority or in the case of health care, being "cost-effective".
We have a perfectly corrupted system of hospital care for people with severe mental illnesses. Businesses and governments can essentially do what they want. Many of these settings are so miserable that good psychiatrists avoid them. Patients churn in and out often with no changes or changes that are so abrupt that they are immediately rehospitalized.
There is a solution that can have immediate impact and potentially lead to reform. I applaud James Brown in this case for disclosing what happened to him and elegantly stating what he was deprived of. On the other hand, nobody should have to forfeit their confidentiality and talk about what continues to be a stigmatizing illness just because business friendly systems predictably fail to provide quality medical care and marginalize medical decisions. A whistleblower statute that protects any psychiatrist who reports that their patient was discharged against their recommendations and given a bus ticket is a quick solution. It should also apply when a managed care company is insisting that an unstable patient be discharged when they remain at high risk or have not been evaluated or treated. The ABC story here suggests that these discharged patients may be "dangerous to themselves or others". In fact, the majority of these cases are very vulnerable people who need help and protection. That help and protection is not coming from a government set up to protect the managed care industry and those forces that ration care for the mentally ill.
George Dawson, MD, DFAPA
ABC News. Man with Psychosis Recalls Nevada 'Patient Dumping'.
When I looked at this clip I was amazed for a couple of reasons. First off, it was on the APA's Facebook feed with a comment by the Medical Director. Without going into all of the details that I have posted so far on this blog, I will say that it is about time and leave it at that. The fact that nothing has been said to this point is also reflected in my second point and that is - this has been going on for over 20 years! Every place in this country with a major psychiatric hospital has been the recipient or point of origin for discharges by bus to another state. It is so common that I used to refer to it as Greyhound Therapy with my coworkers and everybody knew exactly what I was talking about.
At first blush putting somebody with a severe mental illness on a bus and sending them to another state - sometimes across a number of states seems inhumane. In some cases, the person himself may insist but if we are talking about the instance where the person is mentally ill and cannot care for themselves - I agree completely. It is inhumane and not really ethical from the standpoint of a physician. So how does it occur?
It basically occurs by taking a business approach to psychiatry. Rationing and cost center management coalesce into the perfect mechanism to get people out of psychiatric hospitals when they are at their most vulnerable. I have posted many times the concept of getting people out of the hospital before the hospital loses money on a DRG payment. That is generally within 3 - 5 days. That period of time is well below any acceptable time period necessary for the evaluation or treatment of severe psychiatric problems. Everyone agrees that hospital treatment like outpatient treatment means treating people with medications and in hospitals the medications are generally added faster and at much larger doses than in outpatient settings. Five days does not allow for any changes if there are side effects or inadequate treatment response or comorbid medical complications that may crop up. So doctors don't want to use this approach. Who does?
The main drivers are managed care companies and the government agencies that promote these tactics. So the psychiatrist doesn't want to discharge the patient in 5 days - get a managed care reviewer to say that the hospital stay is no longer "medically necessary" and will not be paid for. If the attending psychiatrist doesn't like that decision - he or she can appeal it to another reviewer within the same company. How do you think that will turn out? Of course you can always appeal to the state - right? The state has managed care rights embedded in their statutes. The appeal goes through a commission that is often staffed by insurance industry insiders and they are not there to advocate for patients or their physicians. In the case of psychiatrists who are unfortunate enough to work for managed care companies, they may find their discharge decisions commandeered by case managers and a medical director whose only jobs are to get people out of the hospital as soon as possible. Disagree with them and you might hear that the medical director will come down and take over discharging the patient. Or you might find yourself fighting a never ending series of political battles for not being a "team player." The discharge team may decide to do an end run around you entirely and that could involve putting somebody on a bus.
What about the psychiatrists working in these settings? Why don't they ever speak up? It should be obvious from the preceding paragraph that it could result in getting fired or forced out in one way or another. Every organization these days has policies that stifle disclosure from physicians working in those companies. All of the communication needs to go though an administrator who has the company's best interest at heart. The interest of the patient, the physician, and the physician-patient relationship is not a priority. Making money is the priority or in the case of health care, being "cost-effective".
We have a perfectly corrupted system of hospital care for people with severe mental illnesses. Businesses and governments can essentially do what they want. Many of these settings are so miserable that good psychiatrists avoid them. Patients churn in and out often with no changes or changes that are so abrupt that they are immediately rehospitalized.
There is a solution that can have immediate impact and potentially lead to reform. I applaud James Brown in this case for disclosing what happened to him and elegantly stating what he was deprived of. On the other hand, nobody should have to forfeit their confidentiality and talk about what continues to be a stigmatizing illness just because business friendly systems predictably fail to provide quality medical care and marginalize medical decisions. A whistleblower statute that protects any psychiatrist who reports that their patient was discharged against their recommendations and given a bus ticket is a quick solution. It should also apply when a managed care company is insisting that an unstable patient be discharged when they remain at high risk or have not been evaluated or treated. The ABC story here suggests that these discharged patients may be "dangerous to themselves or others". In fact, the majority of these cases are very vulnerable people who need help and protection. That help and protection is not coming from a government set up to protect the managed care industry and those forces that ration care for the mentally ill.
George Dawson, MD, DFAPA
ABC News. Man with Psychosis Recalls Nevada 'Patient Dumping'.
Wednesday, May 1, 2013
Nature Takes A Shot at DSM5 – Spectrums Only Get You So Far
"The Catholic Church changes its pope more often than the APA publishes a new DSM." (reference 1)
I was disappointed to see another shot at the DSM, this time
on my Nature Facebook feed. I suppose with the impending release it is a
chance to jump on the publicity bandwagon.
I will jump over numerous errors in the first paragraph (David Kupfer – modern
day heretic?!) and get to the main argument.
The author in this case makes it seem like seeing psychopathological
traits on a spectrum
is somehow earth shaking news and yet another reason to trash a modest
diagnostic manual designed by psychiatrists to be used as a part of psychiatric
diagnostic process.
In evaluating this article the first question is the whole
notion of continuums. The idea has
been there for a long time and this is nothing new. Just looking at some DSM-IV major category
criteria like major depression, dysthymia, and mania and just counting symptoms
using combinatorics you get the following possibilities:
Major depression - 20 C 5 = 15,504
Manic episode - 15 C 3 = 455
Dysthymia - 2 C 10 = 45
Mixed - 20 C 5 + 15 C 3 = 15,959
That means if you are following the DSM classification and
looking just at the suggested diagnostic combinations you will be seeing
something like 16,004 combinations of mood symptoms just based on a categorical
classification. Superimposed reality can
expand that number by several factors right up to the point that you have a
patient who cannot be categorically diagnosed. If you add all Axis II
conditions with mood sx - there is another large expansion in the number of
combinations. The sheer number of combinations possible should suggest at
some point that the discrete categories give way to a frequency
distribution. The only problem of course
(and this is lost or ignored by all managed care and political systems) the
clinician is treating an individual patient with certain problems and not
addressing the entire spectrum of possibilities. The other reality is that if you put a point anywhere on the spectrum including the Nature blog's mental retardation-autism-schizophrenia-schizoaffective disorder-bipolar and unipolar disorder spectrum - you essentially have a categorical diagnosis.
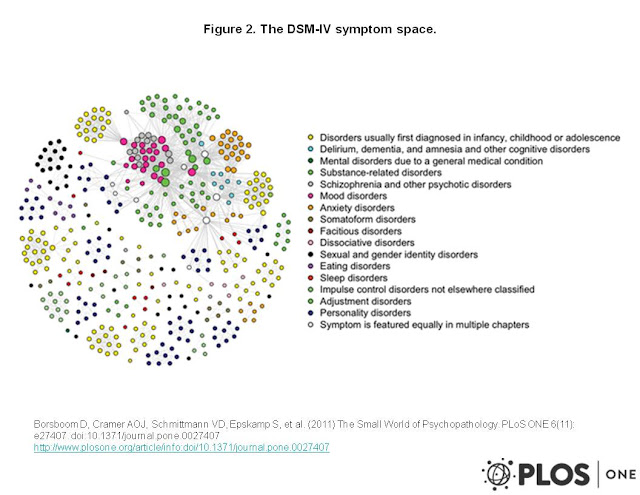
In a recent article, Borsboom,
et al use a graphing approach to show the relationship between the 522
criteria (simplified to 439 symptoms) of 201 distinct disorders in the
DSM-IV. The authors demonstrate that
these symptoms are highly clustered relative to a random graph and go on to
suggest that their network model currently account for the variance in genetics,
neuroscience, and etiology in the study of mental disorders. Their figure below is reproduced in accordance with the Creative Commons 3.0 license. (click to enlarge).

For the example given
by the author’s example – schizophrenia with obsessive traits, we still need to
make that characterization in order to proceed with treatment. The diagnostic categories “schizophrenia”
and “obsessive compulsive disorder” and “obsessive compulsive personality
disorder” are still operative. What does
saying that there is a “continuum” or “spectrum disorder” add? In initial evaluations psychiatrists are
still all looking for markers of all of the major diagnostic categories and
listing everything that they find. The
treatment plan needs to be a cooperative effort between the psychiatrist and
patient to treat the problems that are affecting function and leading to
impairment. The idea that there will be
a magical genetic and brain imaging test that will result in a “proper clinical
assessment” at this point is a pipe dream rather than a potential product of a
diagnostic manual. The limitations of the spectrum approach are also evident in this article that points out the failed field trials attempting to use a dimensional approach for personality disorders.
George Dawson, MD, DFAPA
1. Adam D. Mental health: On the spectrum. Nature. 2013 Apr
25;496(7446):416-8. doi: 10.1038/496416a. PubMed PMID: 23619674
2. Borsboom D, Cramer AO, Schmittmann VD, Epskamp S, Waldorp
LJ. The small world of psychopathology. PLoS One. 2011;6(11):e27407. doi: 10.1371/journal.pone.0027407.
Epub 2011 Nov 17. PubMed PMID: 22114671
Friday, April 26, 2013
A Grand DSM critique from Health Affairs
There is a large Health Affairs article that just became
available online. It criticizes (what
else) the DSM 5. The article and its
initiatives all seem to flow from the conclusion:
"Inadequate interdisciplinary review and collaboration translate into missed opportunities to increase the accuracy of explanations for mental disorders. They also lead to suboptimal care and outcome disparities for millions of patients at a time when dramatic differences in psychiatric diagnosis and treatment rates by sociodemographic status, ethnicity, and geography have undermined public confidence in psychiatry.” (p 7)
"Inadequate interdisciplinary review and collaboration translate into missed opportunities to increase the accuracy of explanations for mental disorders. They also lead to suboptimal care and outcome disparities for millions of patients at a time when dramatic differences in psychiatric diagnosis and treatment rates by sociodemographic status, ethnicity, and geography have undermined public confidence in psychiatry.” (p 7)
I hope that anyone reading this blog knows what the factors
are in the mismatch between psychiatric diagnoses and care. I hope that anyone reading this blog knows
the biases against psychiatry and how that influences the allegations of
overdiagnosis, diagnostic reliability, overprescriptions and conflict of interest that are typically leveled at psychiatrists and their professional
organization. The most obvious example
and a point that seems to be completely lost on these authors is the rationing
of psychiatric services and the resulting fact that most of the diagnostic
disparities that they are complaining about are not due to psychiatrists or the
DSM. I hope that any reader here has also noted my
running commentary about the real causes of “suboptimal care and outcome disparities”. It is directly related to managed care,
pharmacy benefit managers, and the adoption of these same rationing practices
by local, state, and federal governments charged with the provision of mental
health and substance abuse services.
The authors seem to lack an understanding of some of the
basic social processes that they believe to be impacted by the DSM. They cite the New York Times as a source for
the issue of whether the DSM committee backed down on diagnostic revisions that
would have disqualified “half of those who currently receive benefits for
autism spectrum disorders” and various other changes. As a psychiatrist who is intimately familiar
with the disability process, the determination of disability is a political process
at the level of the Social Security Administration. A diagnosis is an entry point but it does not
assure a disability award or even ongoing disability payments. I have seen patients who were hospitalized for
severe problems who did not get a disability determination in their favor. I have seen people who clearly misrepresented
themselves, did not believe they have a mental disability, and who received
disability determinations that they requested.
As far as I can tell, the system is currently set up to favor people
with mental illnesses who have been hospitalized at least three times in two
years. There are companies who
facilitate applications. It generally
takes a series of two or three appeals that can drag out over a year or
two. If it comes to a hearing, those
hearings are uncontested and they are not adversarial in that the government does
not have an attorney present to oppose the application and the decision is made
by a judge and not a jury. The most significant political event in this process
occurred about 15 years ago when the government decided it would not consider
alcoholism and drug addiction a disability.
Prior to that alcoholism was a leading cause of disability in many
states. With all of those political variables
how can a DSM diagnosis be seen as the rate limiting step in that process?
The authors also conclude “Psychiatric conditions result
from a combination of biological and environmental factors”. The arguments that follow suggest that psychiatrists
are basically clueless about these phenomenon.
I did not see George Engel or the biopsychosocial model of illness
referenced. In Engel's seminal 1977 paper
in Science, he directly addressed the
limitations of the biomedical model and changed the paradigm for the future by
proposing a biopsychosocial model. This paper
is dramatic in its intellectual scope and it addresses practically
all of the issues brought up in the Health Affairs article including several
areas that are not addressed such as the experience of the patient. Engel also addressed the issue of “When is
grief a disease?”, a popular current DSM critique:
“…Hence the physician’s basic professional knowledge and
skills must span the social, psychological, and biological for his decisions
and the actions on the patient’s behalf involve all three. Is the patient suffering normal grief or
melancholia? Are the fatigue and
weakness of the woman who recently lost her husband conversion symptoms, psychophysiological
reactions, manifestations of a somatic disorder, or a combination of
these. The patient soliciting the aid of
a physician must have confidence that the MD degree has indeed rendered that
physician competent to make such differentiations.”
A reference to Engel would seem appropriate but it detracts
from the authors’ contentions that physicians seem to need to have their
biopsychosocial horizons broadened and acknowledging that a physician discussed
this definitively 35 years ago would detract from their argument.
The authors more direct arguments about the role of “social
and institutional influences on diagnosis” can be similarly addressed. Although they don’t acknowledge the DSM, they
discuss post traumatic stress disorder as an example of environmental exposure. They
cite evidence gathered in the psychiatric literature as their proof. In fact, any psychiatric evaluation should
contain a formulation section that considers social, biological, and
consciousness based factors in the overall evaluation of the person seeking
help. This is nothing new and every
competent psychiatrist is trained to do this.
The now abandoned oral Board exam, used to test these skills. The idea that these factors are relevant to
psychiatric diagnosis have been taught to psychiatrists for decades. Do we really need to learn that from a panel of social experts who don't talk with people about that information every day like we do?
The idea that social
context, is a relevant factor has
also been obvious to psychiatrists for a long time. Psychiatrists are routinely asked to evaluate
and treat patients from various socioeconomic and cultural groups and
frequently work with interpreters in the process. There is no basis in fact for their
speculative comment that “Identifying and understanding the causes of
diagnostic disparities can lead to improved diagnostic criteria and their more
accurate application.”
On the issue of institutional
and policy factors the authors also miss the mark. They make the previous mistake about
diagnosis and Social Security disability by suggesting that a specific
diagnosis results in a disability check.
They do not point out how the Social Security process rather than a DSM
diagnosis may be more important in the issue of disabilities for mental health.
Interestingly they are concerned about the “major consequences for payers and
patients" and reference a study looking at the prescription of atypical
antipsychotic medications for children.
They ignore the fact that the actual treatment of mental illnesses are
outside of the purview of the DSM and that overprescription (if this is
actually overprescription) is a widespread problem that extends well beyond the
field of psychiatry. As is the case with
all critics of psychiatry and the DSM, they give a pass to the real causes of
systemic poor treatment and a focus on medications rather than psychosocial
therapies and that is the managed care industry and its supporters at all
levels in the government.
Their final focus on publicity
and marketing is certainly not a problem specific to psychiatry. It is also a process that is not DSM
dependent. Restless leg syndrome or
insomnia do not need to be in the DSM to end up being treated on a large scale
by primary care physicians. All it takes is a pharmaceutical company web site with a checklist. They provide
no insight into why the political process of direct-to-consumer advertising as determined
by lobbyists, politicians, and the associated exchange of money should be part of a DSM oversight process.
The authors proposed Psychiatric
Diagnosis Review Body and its potential benefits are equally speculative. Their idea that there would be “greater
sophistication” in the explanations of mental illness is doubtful, especially
considering the impact that Engel’s biopsychosocial model has had on both the
field and DSM development. Their idea
that the work of a review body would “heighten mental health practitioners’
awareness of population level differences in diagnoses, in some instances
improving their ability to tailor diagnoses to patient’s demographic
characteristics and cultural backgrounds…” is also problematic. First off, the DSM is written for
psychiatrists and a psychiatric diagnosis and formulation is much more than looking
at a list of symptoms that possibly identifies a person as being a statistical
outlier in a group. Any person can pick
up a copy of the DSM and presume to make a "diagnosis" based on these criteria,
but that is not a psychiatric diagnosis.
Secondly, cultural, demographic characteristics, and demographic factors
have already been incorporated into psychiatric evaluations for decades. An even greater question is what broad scale
social data would add to the evaluation of the individual patient given the biases
that are usually present in those studies.
The authors suggest that the incorporation of feedback from
the review body would “increase public confidence in the manual and psychiatry
as a medical profession”. The single
most important factor that would enhance psychiatry’s image would be the
recognition that rhetorical negative arguments against the profession abound
and need to be corrected. That could
start by recognizing what psychiatrists actually do and what a DSM is actually
used for. It would also take a critical
look at why 20 years of rationing of psychiatric services by the managed care
industry and the government is the single largest factor in why these services
have deteriorated and now operate on the premise that getting people on one
medication or another is the best way to treat mental illness. The authors in this case banter about million
and billion dollar amounts that are typically used to suggest the impact of the
DSM or significant conflicts of interest in psychiatry. Nobody is focused on the fact that the
managed care industry makes far more money than that by denying medical
care. Psychiatric services make up a
disproportionately large amount of denied care.
If you are really interested in improving the care of people
with mental illness in this country it would seem logical to attack those who routinely
deny them care and interfere at all levels with the provision of care rather than those providing the care and trying to improve it. That is the most important social problem
affecting the provision of mental health services and access to psychiatry. Social scientists seem to be as disinterested in that fact as the average journalist.
George Dawson, MD, DFAPA
Hansen HB, Donaldson
Z, Link BG, Bearman PS, Hopper K, Bates LM, Cheslack-Postava K, Harper K,
Holmes SM, Lovasi G, Springer KW, Teitler JO.
Independent Review Of Social And
Population Variation In Mental Health Could Improve Diagnosis In DSM Revisions.
Health Aff (Millwood). 2013 Apr 24. [Epub ahead of print] PubMed PMID:
23614899.
Engel G. The need for a new medical model: a challenge for biomedicine. Science 1977; 196:129-136.
Engel G. The need for a new medical model: a challenge for biomedicine. Science 1977; 196:129-136.
George L. Engel, MD. JAMA.2000;283(21):2857.
doi:10.1001/jama.283.21.2857
Thursday, April 18, 2013
Psychiatric care versus gun control - an expected outcome
Just in case you are keeping score the Senate voted down some modest gun control proposals last week. The issue of coming together over mental health care to address one of the dimensions of mass shootings also did not happen. In the political calculus, it makes sense that if legislators did not fear the gun control lobby they had a lot less to fear from a mental health lobby ambivalent about dovetailing improved mental health care with gun control.
The pro gun advocates especially the NRA have always underscored the idea that they support law abiding citizens having access to firearms. Their mantra for years has been that if there are more obstacles to law abiding citizens getting guns then only criminals would have them. Never mind the significant number of accidental deaths every year and the fact that firearm suicide is consistently greater that firearm homicide in this country. That detail is not lost on psychiatrists interviewing patients who have told us that they were impulsively looking for a gun to kill themselves and the only thing that prevented it was a background check and a waiting period. The main provision of the attempted legislation was an extension of background checks. If the pro gun lobby believes that it is protecting the right of law abiding citizens to purchase firearms, there should be no problem at all with universal background checks. That should cut across all venues where firearms are bought and traded. I have not heard a single rational explanation for voting down extended or universal background checks.
Reaction to the failure of this legislation was as swift as the Sunday morning talk shows. Bob Scheiffer interviewed family members of the victims of the Sandy Hook incident on Face the Nation. They were clearly upset about the vote in the Senate as captured in this quote from Neil Heslin father of 6 year old Jesse Heslin one of the victims of this incident:
"....As simple as a background check, putting aside the assault weapon ban or limitation or control, it's just a stepping stone of the background check with the mental health and the school security. I think the most discouraging part of this week was to, after the vote, to see who voted and who didn't vote, support it, and realize it's a political game. It was nothing bipartisan about it, at all. And we aren't going to go away. I know I'm not. We're not going to stop until there are changes that are made."
In the vacuum of no discussion of the vote against the bill or partisan rhetoric, very little was said in the press about the money behind the vote. OpenSecrets.org did an excellent job of showing that like most things in American politics it looks like a significant factor. Their research clearly shows that the pro-gun lobby can outspend the gun control lobby by as much as 15:1 with most of the money going to Republicans. There are a couple of things working against the pro-gun lobby and all of that money - public support for common sense gun measures like background checks is at an all time high. The second factor is difficult to say out loud but in American culture you can depend on it. There will be more incidents and the pro-gun solutions (armed guards in schools, keeping the guns out of the hands of criminals and the mentally ill) are not really solutions. The pro-gun lobby has demonstrated that they do not take that task seriously.
George Dawson, MD, DFAPA
Senate Blocks Drive for Gun Control. NYTimes April 17, 2013.
S. 649 Roll Call Vote
The pro gun advocates especially the NRA have always underscored the idea that they support law abiding citizens having access to firearms. Their mantra for years has been that if there are more obstacles to law abiding citizens getting guns then only criminals would have them. Never mind the significant number of accidental deaths every year and the fact that firearm suicide is consistently greater that firearm homicide in this country. That detail is not lost on psychiatrists interviewing patients who have told us that they were impulsively looking for a gun to kill themselves and the only thing that prevented it was a background check and a waiting period. The main provision of the attempted legislation was an extension of background checks. If the pro gun lobby believes that it is protecting the right of law abiding citizens to purchase firearms, there should be no problem at all with universal background checks. That should cut across all venues where firearms are bought and traded. I have not heard a single rational explanation for voting down extended or universal background checks.
Reaction to the failure of this legislation was as swift as the Sunday morning talk shows. Bob Scheiffer interviewed family members of the victims of the Sandy Hook incident on Face the Nation. They were clearly upset about the vote in the Senate as captured in this quote from Neil Heslin father of 6 year old Jesse Heslin one of the victims of this incident:
"....As simple as a background check, putting aside the assault weapon ban or limitation or control, it's just a stepping stone of the background check with the mental health and the school security. I think the most discouraging part of this week was to, after the vote, to see who voted and who didn't vote, support it, and realize it's a political game. It was nothing bipartisan about it, at all. And we aren't going to go away. I know I'm not. We're not going to stop until there are changes that are made."
In the vacuum of no discussion of the vote against the bill or partisan rhetoric, very little was said in the press about the money behind the vote. OpenSecrets.org did an excellent job of showing that like most things in American politics it looks like a significant factor. Their research clearly shows that the pro-gun lobby can outspend the gun control lobby by as much as 15:1 with most of the money going to Republicans. There are a couple of things working against the pro-gun lobby and all of that money - public support for common sense gun measures like background checks is at an all time high. The second factor is difficult to say out loud but in American culture you can depend on it. There will be more incidents and the pro-gun solutions (armed guards in schools, keeping the guns out of the hands of criminals and the mentally ill) are not really solutions. The pro-gun lobby has demonstrated that they do not take that task seriously.
George Dawson, MD, DFAPA
Senate Blocks Drive for Gun Control. NYTimes April 17, 2013.
S. 649 Roll Call Vote
Monday, April 15, 2013
Penis Size and the Primitive State of Sexual Consciousness
On the Nature blog this week, there was a summary of
an article originally posted in Proceedings
of the National Academy of Sciences (PNAS) on the implications of penis size
preference and evolutionary pressure for large penises. If true that may
explain why humans have the largest penis size of all primates. Someone
has apparently already figured out that male genitalia were the earliest
developed physical traits in the animal kingdom.
In the experiment, researchers showed computer generated life
sized projections of 53 frontal images of men of varying heights, flaccid penis
size, and body type to a group of 105 heterosexual Australian women. The
women looked at the images and rated them for sexual attractiveness.
Since the original article is not accessible, the results on the Nature blog state that that a range of
flaccid penis sizes and male body types were rated the most attractive.
At some point masculine body type (greater shoulder width to hip width) was
more important. There was not a direct correlation with penis
size and attractiveness. The graph of size versus attractiveness was
described as an inverted U-shaped curve with attractiveness falling off at both extremes. There were some remarks on the
importance of this finding not the least of which that studies like this may
make it easier to talk about an “uncomfortable subject”. I doubt that the
press will take such a nuanced approached.
As I read that last line, I thought about penis references in the
popular culture over the course of my lifetime from Woody Allen films to
Seinfeld episodes to morning radio shock jocks. I have gone through the
“sexual revolution” and noticed that very little has changed. If anything
the landscape seems to have shifted to a more male dominated perspective with
the further objectification of women and much easier access to that
content. In some of that content there is a disturbing portrayal of
serial violence (usually homicide) and sadomasochism even in prime time
television. All it takes is showing an MALSV (mature audiences, strong
language, sexual situations, violence) disclaimer at the outset to broadcast a
blend of sexual violence and gratuitous nudity. The focus from business
interests is producing as much of this content as possible combined with the
legitimization of the pornography industry. What is driving all of this?
There are two areas relevant to psychiatry that are the object of
very little research and they are sex addiction and sexual consciousness.
Consciousness in general has not been much of a focus by psychiatry since the
advent of DSM atheoretical
descriptors that in effect limited the focus of study to extremes of human
behavior. The consciousness that I
am referring to is the unique conscious state of individuals. The current diagnostic system does not
presume to diagnose individuals
Sexual addiction and other "behavioral addictions" like
eating and gambling are all the rage right now. The neurobiological
theories of reward, initial impulse control involving positive
positive reinforcement, and subsequent compulsive behavior based on
negative reinforcement are thought to apply in traditional chemical addictions
but can the same models apply to sexual behavior? The problem is that
there are vast uncharted areas connected to the midbrain and basal
forebrain structures that are thought to be substrates for addictive
behavior. Not all of the details of neurotransmission within the system
are known even though we have several cartoon versions. An analysis from reference 3 suggests in a rat model of sucrose
self administration that up to 28 regulatory proteins in various cell
structures may form the basis for the signaling involved. Despite several papers suggesting that
behavioral and chemical addictions may have the same substrates, I have not
seen any compelling evidence that this might be true. If sex can be addicting, what are the risks
of exposure and can we help people with serious problems involving their sexual
behavior?
The state of consciousness in psychiatry these days is at an all
time low. Biological reductionism and a poor understanding of the
importance of modern psychoanalysis in exploring unique conscious states may
be part of the problem. The other part of the problem is a single minded
focus on problems with human behavior that are clearly two standard deviations
from the norm. This basically leaves out the unique conscious state of
the individual and the fact that many people are clearly affected by problems
that can't be reduced to a psychopathological model. Human sexual
behavior and all of the behaviors it is associated with are excellent examples
at both an individual and cultural level. Those authors who have taken
on this task; most notably the late Ethel Person, MD have described a continuum of male
sexual fantasy and behavior from the perspective of psychoanalytic theory and
treatment of associated problems. One
of the more interesting considerations to me is the omission of practically all considerations
of fantasy and daydreaming in the DSM as if these important functions have no explanation
and are not as grounded in prefrontal cortex as the working memory is. Do we know the basic differences in the
sexual consciousness of men and women?
Not from anything that I can find.
These considerations are as important for culture as they are for
psychiatry and psychiatric research. The
current cultural attitude seems to be that we need a mechanical understanding of
sex. It is the mechanical approach that
is presented as sex education in school.
Here are the parts, here is how they work, here is how you get pregnant,
and here is how you get diseases. No
relevant discussion about associated emotions, human attachment, desire, or
love. No appreciation of scientific
differences in the sexes. No discussion
about how the really big organ in the head is orchestrating everything. Figuring out how to address these important
issues is a lot more complicated than voting on the most attractive present day
penis.
George Dawson, MD, DFAPA
1. Nuzzo R. Bigger
not always better for penis size. Nature
News April 8, 2013.
2. Mautz BS, Wong
BBM, Peters RA, Jennions MD. Penis size interacts with body
shape and height to influence male attractiveness. Proc. Natl Acad. Sci. USA http://www.pnas.org/cgi/doi/10.1073/pnas.1219361110 (2013).
3. Van den
Oever MC, Spijker S, Li KW, Jiménez CR, et al. A Proteomics Approach to Identify Long-Term Molecular Changes in Rat
Medial Prefrontal Cortex Resulting from Sucrose Self-Administration. Journal of Proteome Research 2006 5 (1), 147-154
4. Ethel Spector Person, MD. The Sexual Century. Yale University Press, New Haven, 1999.
4. Ethel Spector Person, MD. The Sexual Century. Yale University Press, New Haven, 1999.
Sunday, April 14, 2013
Bipartisan Agreement on Treating Mental Illness - Believe It when You See It
The New York Times has an incredibly naive article on how legislators may be split on gun control but both parties support better care for people with mental illnesses. The article alludes to a bipartisan plan that would "prevent killers .....from slipping through the cracks." The next paragraph says that the plan: "would lead to some of the most significant advancements in years in treating mental illness and address a problem that people on both sides of the issue agree is a root cause of gun rampages."
That would be groundbreaking news if it were true, but let's be realistic. The history of funding treatment for addictions and mental illnesses in this country has been a downhill spiral for at least 30 years and there are no real signs that will changed. Congress has essentially been at the root of the problem. Congress after all is responsible for the disproportionately poor level of funding for the treatment of mental illness. Congress basically invented the managed care and pharmacy benefit manager industry that has increased the rationing of psychiatric services that has led to the current deterioration. Rather than focus of providing quality in the services that federal, state, and local governments typically provide (like community mental health centers, case management, civil commitment, protective services, and crisis intervention) they have adopted the managed care model of rationing services.
The only relative bright spot in mental health legislation was a parity law spearheaded by Senators Wellstone and Domenici. The actual boilerplate is one thing and there was always a question about managed care would react to the parity law and if they could continue their successful rationing techniques. Events in the past week suggest that they are as evidenced by the New York State Psychiatric Association and the Connecticut Psychiatric Society joining in a class action lawsuit against United Health Care and Anthem Health Plans for violations of the Mental Health Parity and Addiction Equity Act (MHPAEA). The interesting aspect of the alleged "violations" is that they are standard rationing tactics that have been used by this industry for decades.
There are surprisingly few details of "improved mental health care" provided in this article. There are many legislative tricks to make it seem like something has happened when it really has not. The mental health issue seems like a safe haven for legislators who don't really want to address the gun issue. I have posted some of the rhetoric on the issue here and some of it is fairly grim. The President's initiative in the article involves over $100 million for screening. There is no good evidence that screening adds much more than getting people on medications as fast as possible - probably too many people.
A related issue with Congressional lawmaking is that they rarely seem to consult anyone with expertise. Many consider themselves to be experts in something even though they have never trained or worked in the field. The people with the most significant access are business lobbyists and in many cases they are writing the laws or at least very satisfied with what is happening. The focus is generally on improving the wealth of the folks with the lobbyists. That is unfortunate because there are numerous ways to improve the provision of psychiatric services for severe mental illness without giving away more money to managed care companies. The idea that "the most significant advancements in years in treating mental illness" will come out of Congress and business lobbyists sets my teeth on edge.
George Dawson, MD, DFAPA
Jeremy W. Peters. In Gun Debate No Rift On Care for the Mentally Ill. New York Times April 12, 2013.
That would be groundbreaking news if it were true, but let's be realistic. The history of funding treatment for addictions and mental illnesses in this country has been a downhill spiral for at least 30 years and there are no real signs that will changed. Congress has essentially been at the root of the problem. Congress after all is responsible for the disproportionately poor level of funding for the treatment of mental illness. Congress basically invented the managed care and pharmacy benefit manager industry that has increased the rationing of psychiatric services that has led to the current deterioration. Rather than focus of providing quality in the services that federal, state, and local governments typically provide (like community mental health centers, case management, civil commitment, protective services, and crisis intervention) they have adopted the managed care model of rationing services.
The only relative bright spot in mental health legislation was a parity law spearheaded by Senators Wellstone and Domenici. The actual boilerplate is one thing and there was always a question about managed care would react to the parity law and if they could continue their successful rationing techniques. Events in the past week suggest that they are as evidenced by the New York State Psychiatric Association and the Connecticut Psychiatric Society joining in a class action lawsuit against United Health Care and Anthem Health Plans for violations of the Mental Health Parity and Addiction Equity Act (MHPAEA). The interesting aspect of the alleged "violations" is that they are standard rationing tactics that have been used by this industry for decades.
There are surprisingly few details of "improved mental health care" provided in this article. There are many legislative tricks to make it seem like something has happened when it really has not. The mental health issue seems like a safe haven for legislators who don't really want to address the gun issue. I have posted some of the rhetoric on the issue here and some of it is fairly grim. The President's initiative in the article involves over $100 million for screening. There is no good evidence that screening adds much more than getting people on medications as fast as possible - probably too many people.
A related issue with Congressional lawmaking is that they rarely seem to consult anyone with expertise. Many consider themselves to be experts in something even though they have never trained or worked in the field. The people with the most significant access are business lobbyists and in many cases they are writing the laws or at least very satisfied with what is happening. The focus is generally on improving the wealth of the folks with the lobbyists. That is unfortunate because there are numerous ways to improve the provision of psychiatric services for severe mental illness without giving away more money to managed care companies. The idea that "the most significant advancements in years in treating mental illness" will come out of Congress and business lobbyists sets my teeth on edge.
George Dawson, MD, DFAPA
Jeremy W. Peters. In Gun Debate No Rift On Care for the Mentally Ill. New York Times April 12, 2013.
Sunday, April 7, 2013
The “Spike” in ADHD diagnoses
There was the usual furor in the press earlier this
week about a CDC Study that suggested that ADHD diagnoses have spiked up to
11%. A previous post on this blog suggests
that the real prevalence of ADHD is closer to 6-8%. The
press predictably implicates overdiagnosis, overprescribing, a Big
Pharma based culture that suggests there is a pill for everything, and of
course the DSM5 – even though it has not yet been released. What is really going on?
Before getting into my theories let me express my profound
disappointment in the Centers for Disease Control (CDC). As far as I can tell they have no actual
research document on this issue, at least they did not sent me that document or
link when I requested it. The closest I
can come is the web page that suggests that it may contain the data. You can find for example – the full text of
the survey that was used for this data.
If you are interested in that actual data that lists several data files
that require specialty software. So we
apparently have a “scoop” by the New York Times based on getting and analyzing
the data files and other interested people (like me) do not have access to the
original data. That is really not acceptable for a government funded agency.
If I am wrong here – please send me the link or the raw data, but I am
very clear that the CDC did not respond to my direct request for clarification and
they always have in the past.
Rather than debate the limitations of the study which is not
possible because there apparently is no published version of the study, the
easiest thing to do is accept that the increase is diagnoses as estimated
by surveys is in fact true and go from there.
When I think about drugs that are truly overprescribed by comparison,
the first class that comes to mind is antibiotics. This trend is so well known that the CDC has
run a campaign about it since 1995.
There is some consensus that progress has been made but a recent
commentary describes the overall effort as a failure with antibiotic
overuse as high as 50-100% in some areas and suggests a comprehensive
strategy. The table below highlights a
few problems especially with regard to treating infections caused by viruses
with antibiotics in the past two years.
Problem
|
Findings
|
Reference
|
Acute sinusitis
3 million outpatient visits/yr in US
|
Antibiotics prescribed in 83% of visits
50% of patient diagnosed received a macrolide or quinolone and only
20% received amoxicillin – the recommended drug
|
Fairlie T, Shapiro DJ, Hersh AL, Hicks LA. National Trends in Visit
Rates and Antibiotic Prescribing for Adults With Acute Sinusitis.Arch
Intern Med. 2012;172(19):1513-1514.
|
Acute Strep Pharyngitis
|
56% received an antibiotic and only 19.5% had a confirmed diagnosis
|
Nakhoul GN,
Hickner J. Management of Adults with Acute Streptococcal
Pharyngitis:
Minimal Value for Backup Strep Testing and Overuse of Antibiotics. J Gen
Intern Med. 2012 Oct 6.
|
Febrile Respiratory Illness (AFI)
|
The context (number of cases recently seen and pandemic status) affected
whether or not physicians prescribe antibiotics for AFI.
|
Courtney
Hebert, Jennifer Beaumont, Gene Schwartz, Ari Robicsek; The Influence of
Context on Antimicrobial Prescribing for Febrile Respiratory IllnessA Cohort
Study. Annals of Internal Medicine. 2012 Aug;157(3):160-169.
|
Unnecessary fluroquinolone use in hospitalized patients
|
39% of fluroquinolone use was unnecessary as defined as excessive duration
of therapy or use for non bacterial infection.
|
Werner NL,
Hecker MT, Sethi AK, Donskey CJ. Unnecessary use of fluoroquinolone
antibiotics
in hospitalized patients. BMC Infect Dis. 2011 Jul 5;11:187. doi:
10.1186/1471-2334-11-187.
|
A direct comparison of antibiotic over prescription and the
possible over prescription of stimulants is instructive from several perspectives.
It may not be obvious but a clinician faced
with whether or not a patient has a bacterial infection or whether they have
ADHD has similar problems. In both
cases, the therapy may precede the diagnosis.
By that I mean it is often impossible on purely clinical grounds to
determine whether an infection is caused by bacteria or the patient's behavioral
or cognitive complaints are cause by ADHD. If at the end of an assessment the physician
comes to the conclusion of bacterial infection or ADHD a medication is
prescribed. Nobody makes a probability
statement and there is often the element of an “empirical trial” – if the
patient improves the treatment and the diagnosis were correct. Since
any misdiagnosed viral infections will usually improve and most people given
stimulants will experience cognitive enhancement whether they have ADHD or not –
the empirical trial is a highly flawed approach but one of many biases in an
area of diagnostic uncertainty.
Another issue is the expectations of the patient. Pediatricians often face irate parents if
they don’t prescribe antibiotics for certain infections that are likely to be
viral. Internists and family physicians
face the same problem explaining why acute bronchitis generally does not
require antibiotic therapy. Patients
often have stories about multiple antibiotic failures to treat their bronchitis
when it is likely that the process was viral and happened to resolve on its own after the most recent
antibiotic trial. Many patients taking stimulants for no clear reason have similar reactions when their use of stimulants is questioned.
There is the issue of complications of both therapies. I do think that the potential harm of antibiotic overprescribing far exceeds the harm of stimulant overprescribing and that is the basis for the CDC having an initiative in this area for nearly 20 years. On the basis of acute complications and medical side effects stimulant medications are some of the safest around. On the other hand, I have also treated stimulant abusers who were routinely taking several times the recommended dose for years or who went on to use cocaine or other stimulants regularly and had the expected complications from addiction.
An important area of divergence between these classes of prescription
drugs is the potential for addiction with stimulant medications and the new
cultural movement that has been described as “cognitive enhancement”. Both of these factors add the dimension that
patients can misrepresent themselves to physicians with the intent of getting a stimulant prescription. That does not happen with antibiotics, but the scope of the problem in
terms of which drug is overprescribed more seems decidedly in favor of antibiotics
at this time. That does not bode well
for the potential for even higher rates of stimulant overutilization in the
future and in fact it seems obvious to me that there is no reason why it would
not rise to at least the same level of antibiotics.
The reaction to these parallel problems in the press is
instructive. Rather than seeing the
possible over prescription of medications as a problem inherent in the practice
of medicine (like antibitotics) – a common reaction in the press is that this is a problem with over diagnosis
and leaps to suggesting that the unreleased DSM5 will lead to even more
diagnoses. They quote several experts
who respond strictly on the issue of whether the numbers are “real” or
not. The Director of the CDC – Thomas R.
Frieden, MD makes an accurate comparison of the problem to both antibiotics and
pain medications but concludes: “The
right medications for A.D.H.D., given to the right people, can make a huge
difference. Unfortunately, misuse appears to be growing at an alarming rate.” Clear diagnostic criteria for bacterial
infections has not been the solution nearly 20 years of antibiotic over prescribing. From what we know about trends in overprescribing, I would expect stimulant prescriptions to continue to increase irrespective of the release of the DSM5. It will prove to be an easy scapegoat for a poorly understood problem.
The unfortunate focus of the New York Times article is the
familiar: “Are drugs good or bad?” The
appropriate focus for physicians is focusing on the process and how individual
and group practices can be modified to reduce overprescribing. In most cases that would involve four additional
steps – a discussion of cognitive enhancement and why it is not a good idea,
screening for an addiction diagnosis, making sure that there is a clear level
of functional impairment, and urine toxicology. The effects of an assembly line approach to managing physicians and inadequate time for complex diagnostic thinking cannot be minimized. A central collaborative model used by the University of Wisconsin for the diagnosis and treatment of dementia could be adapted to a network of clinics to treat ADHD. This could provide the best solution to practice drift and provide clear markers for uniform prescribing.
George Dawson, MD, DFAPA
Allen Schwartz, Sarah Cohen.
ADHD Seen in 11% of US Children as Diagnoses Rise. NYTimes
March 31, 2013.
Merikangas KR, He J, Rapoport J, Vitiello B, Olfson M.
Medication Use in US Youth With Mental Disorders. JAMA Pediatr.2013;167(2):141-148.
doi:10.1001/jamapediatrics.2013.431.
Rubin D. Conflicting Data on Psychotropic Use by Children:
Two Pieces to the Same Puzzle. JAMA Pediatr. 2013;167(2):189-190.
doi:10.1001/jamapediatrics.2013.433.
Fairlie T, Shapiro
DJ, Hersh AL, Hicks LA. National Trends in Visit Rates and Antibiotic
Prescribing for Adults With Acute Sinusitis.
Arch
Intern Med. 2012;172(19):1513-1514.
doi:10.1001/archinternmed.2012.4089
Gonzales R, Ackerman
S, Handley M. Can Implementation Science Help to Overcome Challenges in
Translating Judicious Antibiotic Use Into Practice?: Comment on “National
Trends in Visit Rates and Antibiotic Prescribing for Adults With Acute
Sinusitis” and “Geographic Variation in Outpatient Antibiotic Prescribing Among
Older Adults”. Arch
Intern Med.2012;172(19):1471-1473. doi:10.1001/2013.jamainternmed.532
Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA,
Lowery JC. Fostering implementation of health services research findings into
practice: a consolidated framework for advancing implementation science. Implement Sci. 2009
Aug 7;4:50. doi: 10.1186/1748-5908-4-50. PubMed PMID: 19664226; PubMed Central PMCID:
PMC2736161.
Hebert C, Beaumont J, Schwartz G, Robicsek A. The influence of
context on antimicrobial prescribing for febrile respiratory illness: a cohort
study. Ann Intern
Med. 2012 Aug 7;157(3):160-9. doi: 10.7326/0003-4819-157-3-201208070-00005.
PubMed PMID: 22868833.
The Duty to Warn, Law Enforcement and the Public Health
The issue of reporting dangerousness to law enforcement was in
the news this week with a story 2 days ago about the accused Colorado theater
shooter James Holmes. I happened to catch
it on public radio where it was announced that NPR had been one of the news
organizations who had petitioned the court for access to suppressed information
about the psychiatrist’s role. The New
York Times story
states that the psychiatrist – Dr. Lynne Fenton contacted campus police about
Holmes' potential dangerousness and they deactivated his student ID and access
to campus building. Various sources state
that he was threatening his psychiatrist by e-mail. The new information is more detailed than an
original article
from the Denver Post on August 30, 2012.
In the original article Dr. Fenton testified that her
physician-patient relationship with the patient ended on June 11. At that appointment there are some reports
that Holmes told Dr. Fenton that he fantasized about killing a lot of
people. The shooting occurred on July
20. The newly unsealed documents show that the
psychiatrist “told a police officer that her patient had confessed homicidal
thoughts and was a danger to the public.”
The documents also show that the psychiatrist was being threatened by
both e-mails and texts. Dr. Fenton also
advised the police officer that she was fulfilling her legal requirement by
making the report to the police. A
related article states that police officer asked Dr. Fenton if she wanted the
subject apprehended and placed on a 72 hour hold and she said that she did not.
In addition to the public health concern about homicide
prevention, psychiatrists in this situation have a concern about the need to
prevent their patients from harming others.
That forms the basis of at least one dimension of most state civil commitment
laws. Most state laws describe a duty to
warn potential victims, but forensic psychiatry texts talk about more general
responsibilities. For example, Gutheil
and Appelbaum state:
“Psychiatrists have
always faced the potential of suits as a result of negligently allowing
patients to be released or to escape from inpatient facilities when these
patients later cause harm to others…” (p. 148)
In a typical outpatient setting, the modern duty to protect
identifiable persons dates back to the Tarasoff
case or Tarasoff v. Regents of the University
of California. In this case a
psychologist was informed by his patient that he intended to kill a young
woman. The psychologist contacted campus
police and advised them that the patient had schizophrenia and should be
detained and committed. The police temporarily
detained the subject but he was released and several months later and killed
the identified victim. The courts found
that there was a duty to warn the identified victim that superseded confidentiality. I encourage anyone to read the details of the
original review of the case to notice how negligence in this case passes from
the mental health professionals to the police and back. I think that there may be a more straightforward
analysis and I would invite any evidence to the contrary. My understanding is that the legal profession
studies negligence from the perspective that there is no one who is free from
responsibility. In any complex activity like
needing to report dangerousness, there will always be some sharing of responsibility if there is a bad outcome. From a
physicians perspective the probability of that happening increases with the
presence of liability insurance.
On a personal level, occupational stress goes through the
roof in situations like this. Imagine
that you are seeing patients in a clinic and trying to be as helpful as
possible and you have just seen a person who you think is dangerous. The situations is more complex if that
patient has threatened a specific person, threatened you and your family, or brought
a weapon into the clinic. The first
order of business is to try and calm down.
In some cases you may have colleagues available for consultation, but in
many cases a psychiatrist is on their own.
The next step is figuring out whether you are in a situation that
requires a duty to warn and what must be done to fulfill that obligation. State statutes are complicated and not uniform. In a recent review
of state Tarasoff laws, the statutes of all 50 states and the District of
Columbia were categorized into whether or not reporting was mandatory,
discretionary, or no law at all. The definition of mandatory for this classification
was a requirement to warn. Discretionary
allows for a breach of patient or client privileges for the purpose of
warning. Using this analysis 33 states
have a mandatory duty, 11 states are discretionary and 7 states have no law. Psychiatrists at this point may seek legal
consultation due to the complexity of the situation and may still receive vague
advice. A good example is something
along the lines of: “Well I would rather defend you for this rather than that.” –
based on their preceding legal advice.
The first time I bumped up against that advice I realized that doctors
were cannon fodder for the legal profession.
The second critical point is the call to the police. In both of the cases mentioned so far campus
police were involved. Are there courts
where that would be questioned? I don’t
think that duty to warn laws specify any particular law enforcement. Despite that lack of specificity, the police
have widely variable capacities to respond to these calls. The police can be notified and nothing can
happen. As illustrated in this post, the
police can be notified and decide on their own that the patient is not dangerous
and release them. That also applies to
what type of protection the police can offer potential victims. I have seen the police go directly to a the
person issuing the threats and tell them there will be clear legal problems if
they do not stop to mailing a fax of a handgun receipt of transaction where the
potential perpetrator who had already issued threats had acquired a
handgun. There is often a significant
gap between any report to the police and palpable decrease in danger to those
threatened. In many cases an entire clinic
is threatened and a safety plan needs to be put in place.
The final consideration is whether the person needs an acute
evaluation and emergency hospitalization for psychiatric assessment. I have several previous posts giving my
perspective on the issue of homicide prevention and how acute psychiatric
treatment can prevent aggression and violence, but it takes a functional
commitment court and facilities that have the expertise to provide this level
of treatment. Many decisions seem to be
made based on existing resources rather than any absolute quality marker. Should any person who is homicidal because of
an acute psychiatric disorder not be hospitalized because the local community
hospital does not treat aggressive individuals?
Should that decision be made on a decision by Medicare or the managed
care industry on how many days of hospital care they will pay for? Hospitalizations for these patients typically
outrun the funding by 2 – 3 weeks.
Like all of the piecemeal approaches to involuntary treatment
there is an easy fix. I did not digress
into the tremendous amount of stress these situations cause and how that stress
can drag on for weeks to months. If
there is an adverse outcome the stress level is even worse. What is needed is a clear pathway that
maintains the boundary between law enforcement and psychiatry. A uniform law implemented across the country should
clearly say that a psychiatrist has a duty to report to law enforcement and at
that point law enforcement has a duty to assess and potentially detain the
person making the threat. That would
include transporting them to a hospital that does civil commitments for
emergency treatment as necessary. Law enforcement
also needs to warn the potential victim and protect them. Psychiatrists should have no duty to track
down identified victims or apprehend or take threatening
patients into custody. That is clearly the purview of
law enforcement.
The technical details of the interface between the law and
psychiatry in the case of a threatening or potentially violent patient needs a
great deal of improvement. There are
very few situations as stressful in the rest of medicine. Some psychiatrists will encounter these
situations only a few times in their career and others are immersed in
aggression and violence. Improving the
approach will enhance assessment and treatment of the problem and also make it easier to
recruit talented people to focus on the problem.
George Dawson, MD, DFAPA
Edwards, Griffin Sims, Database of State Tarasoff Laws
(February 11, 2010). Available at SSRN: http://ssrn.com/abstract=1551505 or http://papers.ssrn.com/sol3/papers.cfm?abstract_id=1551505
Gutheil TG, Appelbaum PS.
Clinical Handbook of Psychiatry and the Law. Lippincott, Williams & Wilkins. Phialdelphia (2000): p 148
Subscribe to:
Posts (Atom)