Does the FDA have a clue about the safe prescribing of opioids? Based on their September 10 press release we are about to find out. If you go to the FDA web page this appears to be the most relevant document. It contains the following warnings:
BOXED WARNING
In the boxed warning in Highlights, include the following text:
• Tradename exposes users to risks of addiction, abuse, and misuse, which can lead to overdose and death. Assess each patient’s risk before prescribing, and monitor regularly for development of these behaviors or conditions. (5.1)
• Serious, life-threatening, or fatal respiratory depression may occur. Monitor closely, especially upon initiation or following a dose increase. Instruct patients to swallow Tradename (formulation) whole to avoid exposure to a potentially fatal dose of (active opioid). (5.2)
• Accidental consumption of Tradename, especially in children, can result in fatal overdose of (active opioid). (5.2)
• For patients who require opioid therapy while pregnant, be aware that infants may require treatment for neonatal opioid withdrawal syndrome. Prolonged use during pregnancy can result in life-threatening neonatal opioid withdrawal syndrome. (5.3)
For products with an interaction with alcohol, also include the following:
• Instruct patients not to consume alcohol or any products containing alcohol while taking Tradename because co-ingestion can result in fatal plasma (active opioid) levels. (5.4)
As I read through these warnings I have several associations. First off, physicians were told 12 years ago in JAMA that they were undertreating pain, misunderstood pain, and that pain treatment needed to change. That was a naive document that depended on an assumption that pain could be "quantitated" on a 10 point scale. Over a decade and 100,000 opioid overdose deaths later we are not told that providing this information on drug labels will make a difference. That leads me to my second association, there is nothing in the above warning that I didn't learn in medical school 30 years ago, including the risk of neonatal withdrawal. The third association is that this definition and intervention is almost completely naive about addiction. A person with an addiction does not care about dire warnings. They don't care about their pain ratings. They care about acquiring and using addictive drugs. It is the nature of addiction. Their entire conscious state has changed. The tendency toward opiate addiction or not is probably biologically determined and a doctor cannot predict who is at risk. If you take an initial dose of opiate and experience intense euphoria, high energy and productivity, and intense sense of well being or feel like you finally have become the person you always wanted to be - you may be a person at high risk for opiate addiction. It doesn't really matter if they have a chronic pain disorder.
What needs to be done? What should the FDA being doing immediately. The four most important misconceptions driving both the epidemic of opioid dependence and the accidental overdose trend are:
1. Opioids are a silver bullet and will eliminate chronic pain if the dose is high enough.
2. Once a maintenance dose is achieved the level of pain relief should be constant.
3. Opioids are only taken for primary gain - the analgesic effect or the elimination of pain.
4. Opiates - prescribed by a doctor will not lead to reactivation of a previous addiction.
What do people need to know now? Probably not the new package insert for opioids. Most physicians don't read it. Every person taking an opioid need to know that it can affect their subjective state in such a way that it will place them at risk for addiction. They need to know at that time that they need to contact their physician and discuss it and the possibility of alternate or more closely monitored treatment. They need to know that there is no medicine that will treat chronic pain into remission. Physicians need to know a number of things including the fact that there is no medication that will eliminate chronic pain. They also need to know that it takes time and detailed evaluations (calls to pharmacy, tox screens, limited prescriptions, assessment of functional capacity) to optimize treatment and prevent addiction.
The warning on a package insert from the FDA containing seriously dated information will not do it. Dire warnings about an epidemic won't do it.
George Dawson, MD, DFAPA
Showing posts with label opioid overdose. Show all posts
Showing posts with label opioid overdose. Show all posts
Monday, September 16, 2013
Friday, February 1, 2013
Treatment of chronic pain with opioids - back to the future
I thought I would wade in on this issue largely because I am not hearing a lot of rational discussion about the problem. You might ask: "What does a psychiatrist know about this issue?" and the answer like most questions about psychiatry is "plenty". I worked on a busy inpatient unit for 22 years and saw plenty of people with with severe chronic pain and episodic pain crises. In that same facility, I also covered consults on medical and surgical patients many having problems with chronic pain and addiction. As an addiction psychiatrist, I have talked with countless people who ran into problems with pain medications or relapsed to using another drug after being exposed to opiates for treatment of acute or chronic pain. There seems to be very little reality based information out there to inform people about the risks and benefits of pain treatment with opiate medication. The argument like most in our society is politically polarized to those who believe it is unconscionable to not treat pain even if it means a long course of opioids to those who believe that opioids are dangerous medications that should be conservatively prescribed. So where does the truth lie?
I can tell you how it was in Minnesota in the 1990's. There were very few pain specialists. The wide spread prescription of opiate medications for chronic noncancer pain by generalists was uncommon. In many cases if it seemed indicated, the generalist would refer their patient to a pain specialist who would provide them with a letter of agreement on the use of chronic opioids. That all changed with a Joint Commission initiative on pain in 2000. At least some authors see it that way and that was my experience. Since then opioid prescriptions have been taking off with an associated increase in the production of these compounds. This graphic from the CDC is instructive (click to enlarge). The rates of increase of sales, deaths, and treatment admissions are all increasing at an astronomical rate relative to population growth.


Like most political debates the current debate about how to stop the epidemic of opioid overdoses ignores that fact that the problem may have originated with a political initiative in the first place. Using the NICE algorithm to get us back to the Minnesota practice model of the 1990s is a logical solution.
George Dawson, MD, DFAPA
Rowbotham MC, Twilling L, Davies PS, Reisner L, Taylor K, Mohr D. Oral opioid therapy for chronic peripheral and central neuropathic pain. N Engl J Med. 2003 Mar 27;348(13):1223-32. PubMed PMID: 12660386.
National Institute for Health and Clinical Excellence. Neuropathic pain: the pharmacological management of neuropathic pain in adults in non-specialist settings. NHS. March 2010.
Supplementary 1:
The Care Pathway Graphic is copyrighted © National Institute for Health and Care Excellence (2010) and is posted based on their allowance for reproduction for educational and not-for-profit purposes. See their updated and revised guideline at: http://www.nice.org.uk/nicemedia/live/14301/65782/65782.pdf
I can tell you how it was in Minnesota in the 1990's. There were very few pain specialists. The wide spread prescription of opiate medications for chronic noncancer pain by generalists was uncommon. In many cases if it seemed indicated, the generalist would refer their patient to a pain specialist who would provide them with a letter of agreement on the use of chronic opioids. That all changed with a Joint Commission initiative on pain in 2000. At least some authors see it that way and that was my experience. Since then opioid prescriptions have been taking off with an associated increase in the production of these compounds. This graphic from the CDC is instructive (click to enlarge). The rates of increase of sales, deaths, and treatment admissions are all increasing at an astronomical rate relative to population growth.

The issue that is debated in the media and some government web sites is why is this happening and what is the best way to deal with it. The FDA has recently incentivized drug manufacturers to come up with better tamper proof opioids. The enforcement arm of the government is rigorously prosecuting some doctors. The FDA has also initiated a course for doctors who prescribe opioids. None of these measures addresses the core problems that were successfully addressed in Minnesota in the 1990s. I will take a look at the specific issues involved:
1. The genetics of opioid preference: People at risk for abuse and addiction to opioids have intensely positive subjective experiences from taking opioids. People not at risk have intensely negative experiences or the opioids make them physically ill. We currently know nothing about the genetics of this response, but it makes sense to let patients know that if they do have an intensely positive response in terms of feeling euphoric or energetic that is not a good sign in terms of addiction potential. It might even be reasonable to come up with a plan about what to do if that happens. Seeing people back in a month who have no knowledge of this risk is probably not the best plan. It is critical that there is a good therapeutic alliance between the patient and physician and that they are both focused on the full spectrum of problems.
2. The genetics of opioid response: Individuals studies and reviews of studies generally show that a subset of patients respond to opioids. There may be additional factors that should factor into patient selection such as the specific type of neuropathic pain. The current concern and reaction to the opioid epidemic is based on the concept that opioid prescribing is a potentially high risk intervention. If that is the case we need a better options for patient selection than a subjective report of pain.
3. The public perception that opioids are the silver bullet of pain relief must be dispelled: This is the driving force behind escalating doses of opioids and the addition of benzodiazepines (an equally bad idea). Excellent double blind placebo controlled studies of self titrated opioids in chronic neuropathic pain have showed moderate pain relief that is on par with non-opioid medication.
4. Tolerance to analgesia and opioid induced hyperalgesia: Education about these phenomena is needed because both lead to escalating doses of opioids. The dose escalation may be appropriate, but in many cases the dose is increased with the goal of eradicating pain and that is an unrealistic goal. In people who have analgesic induced hyperalgesia, they are often shocked that their pain improves with discontinuation of the opioids.
5. Assessment of functional capacity is critical: Functional capacity is the ability to function in daily life. It must be carefully assessed in anyone who is on chronic opioid therapy. At moderate doses and in combination with other pain medications opioids can impair coordination, cause excessive sedation, and lead to significant impairment in daily functioning. This is a sign that the dose of the opioid may be too high and reducing the dose is indicated.
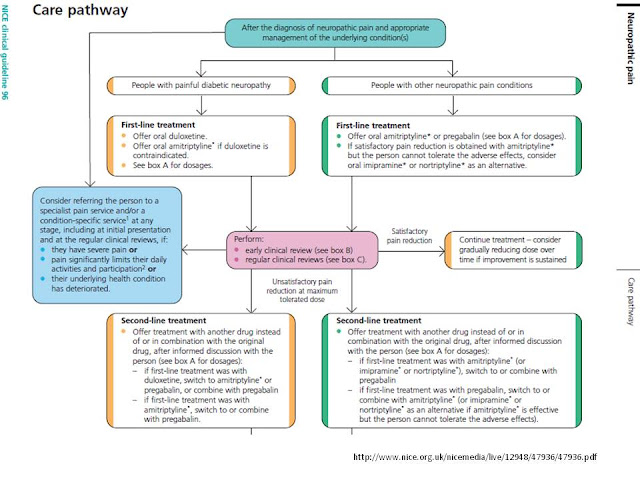
6. A hierarchical approach to pain treatment is still necessary and is the most rational approach to reducing the current epidemic of excessive opioid prescriptions: If the degree of pain relief across a population is the same, why not use the drug with the lowest abuse and overdose potential? That was the default model in the 1990s in Minnesota. The National Health Service in the United Kingdom has operationalized that as their current pathway for treating neuropathic pain in the algorithm below (click to enlarge). Note that the medications with no abuse potential are at the entry levels in this diagram and that pain specialists are the gatekeepers for opioids.


Like most political debates the current debate about how to stop the epidemic of opioid overdoses ignores that fact that the problem may have originated with a political initiative in the first place. Using the NICE algorithm to get us back to the Minnesota practice model of the 1990s is a logical solution.
George Dawson, MD, DFAPA
Rowbotham MC, Twilling L, Davies PS, Reisner L, Taylor K, Mohr D. Oral opioid therapy for chronic peripheral and central neuropathic pain. N Engl J Med. 2003 Mar 27;348(13):1223-32. PubMed PMID: 12660386.
National Institute for Health and Clinical Excellence. Neuropathic pain: the pharmacological management of neuropathic pain in adults in non-specialist settings. NHS. March 2010.
Supplementary 1:
The Care Pathway Graphic is copyrighted © National Institute for Health and Care Excellence (2010) and is posted based on their allowance for reproduction for educational and not-for-profit purposes. See their updated and revised guideline at: http://www.nice.org.uk/nicemedia/live/14301/65782/65782.pdf
Monday, July 30, 2012
PROP Petitions the FDA on Opiates
Physicians for Responsible Opioid Prescribing (PROP) has petitioned the FDA to modify the warnings about opioids. They cite the well known dimensions of the current epidemic including a four fold increase in opioid prescribing and a four fold increase in opioid related overdose deaths. They also cite numerous references about the real risks of prescribing opioids for chronic non cancer pain with very little guidance.
PROP highlights a big problem in medical research and associated public policy and that is the biasing influence of the pharmaceutical industry and a few people at the top. The Institute of Medicine was instrumental in highlighting the issue of chronic pain and framing it as a discrete disease. Although not mentioned specifically by PROP, the Joint Commission (then known as JCAHO) promoted pain recognition and treatment in the year 2000. As this excerpt shows that initiative did not go well.
"In 2001, the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) introduced the concept that pain was the “fifth vital sign,” in an effort to increase the awareness of pain in the hospitalized patient, and by design, improve the treatment of that pain. Unfortunately, the current emphasis on pain assessment as the fifth vital sign has resulted in the potential overmedication of a group of patients (139)" (see ref 1).
Without going into detail at this time, I think that are recurrent patterns of federal and state governments, the managed care industry, and the pharmaceutical industry and their affiliated organisations driving practice patterns and treatment guidelines based on very little evidence. That culminates in broad initiatives like the PPACA that are widely hyped as advances in medical treatment, but they are basically an experiment in medicine founded on business and financial rather than scientific principles. There may be no better example than the practice of prescribing opioids for chronic non cancer pain.
Another contrast for this essay is the comparison with what has been years of psychiatric criticism based on the same principles. The basic argument from the media, antipsychiatrists, generic psychiatric critics, and grandstanding politicians has been that the pharmaceutical industry has been able to financially influence psychiatrists to prescribe drugs that are at the best worthless or at the worst downright dangerous (their characterizations). That despite the fact that black box warnings on psychiatric medication may be held to a much higher standard than other medication even if they target the same level of morbidity and mortality. After all, there is no known psychiatric medication that is mass prescribed and has resulted in overdose deaths at the rate that people are currently dying from prescribed opioids.
Just a few weeks ago, the FDA posted a number of initiatives on their web site focused on the prescription of extended release opioids. My read through the most detailed document shows that it does not touch on the principles outlined by PROP. The idea that this is strictly a matter of educating physicians is an oversimplification. This is a matter of creating initiatives that governments and sanctioning bodies insist that physicians follow and then coming up with other rules when the original ideas fail.
George Dawson, MD, DFAPA
PROP highlights a big problem in medical research and associated public policy and that is the biasing influence of the pharmaceutical industry and a few people at the top. The Institute of Medicine was instrumental in highlighting the issue of chronic pain and framing it as a discrete disease. Although not mentioned specifically by PROP, the Joint Commission (then known as JCAHO) promoted pain recognition and treatment in the year 2000. As this excerpt shows that initiative did not go well.
"In 2001, the Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) introduced the concept that pain was the “fifth vital sign,” in an effort to increase the awareness of pain in the hospitalized patient, and by design, improve the treatment of that pain. Unfortunately, the current emphasis on pain assessment as the fifth vital sign has resulted in the potential overmedication of a group of patients (139)" (see ref 1).
Without going into detail at this time, I think that are recurrent patterns of federal and state governments, the managed care industry, and the pharmaceutical industry and their affiliated organisations driving practice patterns and treatment guidelines based on very little evidence. That culminates in broad initiatives like the PPACA that are widely hyped as advances in medical treatment, but they are basically an experiment in medicine founded on business and financial rather than scientific principles. There may be no better example than the practice of prescribing opioids for chronic non cancer pain.
Another contrast for this essay is the comparison with what has been years of psychiatric criticism based on the same principles. The basic argument from the media, antipsychiatrists, generic psychiatric critics, and grandstanding politicians has been that the pharmaceutical industry has been able to financially influence psychiatrists to prescribe drugs that are at the best worthless or at the worst downright dangerous (their characterizations). That despite the fact that black box warnings on psychiatric medication may be held to a much higher standard than other medication even if they target the same level of morbidity and mortality. After all, there is no known psychiatric medication that is mass prescribed and has resulted in overdose deaths at the rate that people are currently dying from prescribed opioids.
Just a few weeks ago, the FDA posted a number of initiatives on their web site focused on the prescription of extended release opioids. My read through the most detailed document shows that it does not touch on the principles outlined by PROP. The idea that this is strictly a matter of educating physicians is an oversimplification. This is a matter of creating initiatives that governments and sanctioning bodies insist that physicians follow and then coming up with other rules when the original ideas fail.
George Dawson, MD, DFAPA
1. Trescot AM, Helm S, Hansen H, Benyamin R, Glaser SE, Adlaka R, Patel S, Manchikanti L. Opioids in the management of chronic non-cancer pain: an update of American Society of the Interventional Pain Physicians' (ASIPP) Guidelines. Pain Physician. 2008 Mar;11(2 Suppl):S5-S62. Review. PubMed PMID: 18443640.
Subscribe to:
Posts (Atom)