The ShrinkRap blog posted a link to an E. Fuller Torrey and D.J. Jaffe editorial in the National Review about how the government has dismantled mental health care for serious mental illnesses and some of the repercussions. Since I have been saying the exact same thing for the past 20 years, they will get no argument from me. Only in the theatre of the absurd that passes for press coverage of mental illness and psychiatry in this country can this subject be ignored and silenced for so long. It was obviously much more important to see an endless stream of articles trying to make the DSM-5 seem relevant for every man. The stunning part about the Newtown article is the commentary about what government officials responsible for policy have actually been saying about it.
The authors waste very little time examining the sequence of events in the Obama administration following the Newtown, Connecticut mass shooting. President Obama initially stated he would "make access to mental health care as easy as access to guns." and set up a Task Force under Vice President Biden to make recommendations. The authors argue that the agency that was consulted, the Substance Abuse and Mental Health Services Administration (SAMHSA) promotes a model of treating mental illness that has no proven efficacy, does not discuss serious mental illnesses in its planning document, ignores effective treatments for serious mental illnesses and actually goes so far as to fund programs that block the implementation of effective treatment programs. In an example of the obstruction of effective programming by SAMHSA funded programs following the Newtown mass shooting:
"But, alas, the situation is even worse. SAMHSA does not merely ignore effective treatments for individuals with severe mental illness. It also funds programs that attempt to undermine the implementation of such treatments at the state and county level. One such program is the Protection and Advocacy program, a $34 million SAMHSA program that was originally implemented to protect patients in mental hospitals from abuse. It was kidnapped by civil-liberties zealots and has been used to block the implementation of assisted outpatient treatment, funding efforts to undermine it in at least 13 states. For example in Connecticut, following the Newtown massacre of schoolchildren, the federally funded Connecticut Office of Protection and Advocacy for Persons with Disabilities testified before a state-legislature working group in opposition to the proposed implementation of a proposed law permitting court-ordered outpatient treatment for individuals with severe mental illness who have been proven dangerous. The law did not pass." (page 3, par 2.)
In other words, a SAMHSA funded program was opposed to a law in Connecticut that could potentially reduce violence from persons with severe mental illness.
SAMHSA administrators are quoted at times in the article. Any quote can be taken out of context but the characterizations of severe mental illness as "severe emotional distress", "a spiritual experience" and "a coping mechanism and not a disease" reflect a serious lack of knowledge about these disorders. The idea that "the covert mission of the mental health system ...is social control" is standard antipsychiatry philosophy from the 1960s. How is it that after the Decade of the Brain and the new Obama Brain Initiative we can have a lead federal agency that apparently knows nothing about the treatment of serious mental illnesses? How is it that apart from some fairly obscure testimony, no professional organizations have pointed this out? How is it in an era where governments at all levels seem to demand evidence based care, that a lead agency on mental health promotes treatment that has no evidence basis and ignores the treatment that is evidence based?
Having been a long time advocate for the prevention of violence by the treatment of severe mental illnesses my comments parallel those of the authors. Inpatient bed capacity in psychiatry has been decimated. They point out that there are only 5% of the public psychiatry beds available that there were 50 years ago. It is well known that people with mental illnesses are being incarcerated in record numbers and some of the nation's county jails have become the largest psychiatric institutions. Where are all of the civil liberties advocates trying to get the mentally ill out of jail?
Only a small portion of the beds available can be used for potentially violent or aggressive patients and that number gets much smaller if a violent act has actually been committed. Most of the bed capacity in this country is under the purview of some type of managed care organization and that reduces the likelihood of adequate assessment or treatment. The discharge plan in some cases is to just put the patient on a bus to another state.
Community psychiatry is a valuable unmentioned resource in this area. In most of the individual cases mentioned in this article, the lack of insight into mental illness or anosognosia is prominent. It is not reasonable to expect that a person with anosognosia will follow up with outpatient appointments or even continue to take a medication that treats their symptoms into remission. Active treatment in the community by a psychiatrists and a team who knows the patient and their family is the best way to proceed. All of this active treatment has been cost shifted out of insurance coverage and is subject to budget cuts at the county and state level.
Civil commitment laws and proceedings are probably the weakest link in treatment. Further cost shifting occurs and violent patients often end up aggregating in the counties with the most resources. Even while they are there, many courts hear (from a budgetary perspective) that they are committing too many people and the interpretation of the commitment law becomes more liberal until there is an incident that leads to the interpretation tightening up again. Bureaucrats involved often become libertarians and suggest that commitment can occur only if an actual violent incident has happened rather than the threat of violence.
Although Torrey and Jaffe are using the extreme situation of violence in the seriously mentally ill to make their point, the majority of the seriously mentally ill are not violent. They need the same resources. It has been thirty years of systematic discrimination against these people, their families and the doctors trying to treat them that has led to these problems. I pointed out earlier on this blog the problem I have with SAMHSA and the use of the term "behavioral health". The problems with SAMHSA and current federal policy are covered in this article and I encourage anyone with an interest to read it. If history is any indication, I don't expect anything serious to come of the criticism. I anticipate a lot of rhetorical blow back at Dr. Torrey. But as a psychiatrist who has worked in these environments for most of my career, his analysis of the problem is right on the mark.
George Dawson, MD, DFAPA
E. Fuller Torrey & D.J. Jaffe. After Newtown. National Review Online.
White House. Now Is The Time. The President's plan to protect our children and our communities by reducing gun violence. January 16, 2013.
Showing posts with label aggression. Show all posts
Showing posts with label aggression. Show all posts
Saturday, August 17, 2013
Saturday, July 13, 2013
The Real Lesson of the George Zimmerman Trial
The latest reality based media event has been the George Zimmerman trial. Zimmerman shot and killed Trayvon Martin and most media outlets have reviewed the details of the case including courtroom reenactments of the physical confrontation that resulted in the shooting. The secondary story is how the public will react to a verdict. A tertiary story that is building at this time is media criticism - has the media gone to far and should there be cameras in the courtroom?
My point is not to reconstruct the arguments of case but to speculate about how unnecessary violent confrontations may occur in the first place. They do occur frequently and the majority of those confrontations are not covered by the press. You might read about them in your local newspaper or if you are a health professional you have probably encountered the victims or the combatants. In my experience, the level of violence and the resulting injuries are always surprising. People are punched in the face or head and die instantly. People are struck or pushed and strike their heads on the way to the ground and die. People are severely beaten on the street for either a trivial reason or the victims of gang violence and die or sustain disabling injuries. Weapons are used against friends and family. It is as if people think that you can engage in Hollywood style mayhem and in the end only the bad guys suffer. The idea that the human body, especially the brain is extremely vulnerable and needs to be protected seems to be suspended. But that in itself is not the root cause of the problem.
Violence and aggression as a means to resolve interpersonal conflict has been with the human race since prehistoric times. I have found that Keeley offers the best historical account and analysis at the level of conflicting villages, city-states, and nations. His original intent was to dispel the notion of the noble savage or the peaceful prehistoric man living in an idyllic situation. He ends up showing that warfare has been a remarkably constant feature across time. From his text:
"According to the most extreme views, war is an inherent feature of human existence, a constant curse of all social life, or (in guise of a real war) a perversion of human sociability created by the centralized political structures of states and civilizations. In fact, cross cultural research on warfare has established that although some societies that did not engage in war or did so extremely rarely, the overwhelming majority of known societies (90-95%) have been involved in this activity." (p 27-28)
In reviewing some of the smaller pacifist pastoral societies, Keeley cites their low population density as well as their strong moral distaste for violence (p 31) as a likely reason that the Semai could return to a peaceful existence after being recruited by the British to fight against Communist insurgents in the 1950s. In his chapter "Crying Havoc-The Question of Causes", Keeley takes a fairly detailed look at how war starts as a combination of psychological and political factors starting off with a conflict between two villages where one village owed the other village a debt. He demonstrates how that that conflict escalates to the point of violence and death for several reasons. He cites prestige, theft, adultery, and poaching as common reasons for conflicts with aggression resulting in death. He concludes that the specific information from an archaeological standpoint is generally difficult to discern and considers broader contexts.
I think the implicit strength of Keeley's work is that he does have a lot of information on warfare and conflict in small and large societies and through all of that information the common thread is that humans resort to violence as a way to resolve conflict, even in situations that are relatively trivial and could easily be resolved by other means. I have made that observation repeatedly in clinical situations and the only exceptions are where the violence is driven by a psychiatric disorder. It is also obvious that learning other strategies can definitely occur often times for the worst possible reasons. An example is an aggressive man with antisocial personality disorder who typically gets what he wants by threatening or harming people. If he survives long enough, he may get to the point where that is a losing tactic and he becomes less aggressive with age. A more common example is the case of people referred to anger control groups through their contact with law enforcement or the courts. Many find that the strategies they learn in these groups are very effective.
So what is the real lesson in this case? The real lesson is that this violent confrontation did not need to occur. All of the energy being expended in the debate about who was the victim and whether or not legal penalties should be assigned misses that point. It should be fairly obvious that each side can construct a detailed narrative of what happened and how that should affect the outcome. My courtroom experience has left me with the impression that it is possible that neither narrative is an entirely accurate representation of what happened. Who would want their future decided by those circumstances?
All of the sensational coverage by the press misses even more widely. Solving conflicts between people by aggression and homicide is a strategy of primitive man. It arose out of a time before there was a legal system or designated police. It came from a time where there was no recognition that every person is unique and society may be less if that unique person is lost. Until there is the realization that violent confrontations are a toxic byproduct of of our prehistoric ancestors and that they are no longer necessary - there will continue to be unnecessary tragedies. Society is currently complex and aggression will never be a final solution. Coming up with better solutions at this point is the next logical step.
George Dawson, MD, DFAPA
Lawrence H. Keeley. War Before Civilization. Oxford University Press, 1997
My point is not to reconstruct the arguments of case but to speculate about how unnecessary violent confrontations may occur in the first place. They do occur frequently and the majority of those confrontations are not covered by the press. You might read about them in your local newspaper or if you are a health professional you have probably encountered the victims or the combatants. In my experience, the level of violence and the resulting injuries are always surprising. People are punched in the face or head and die instantly. People are struck or pushed and strike their heads on the way to the ground and die. People are severely beaten on the street for either a trivial reason or the victims of gang violence and die or sustain disabling injuries. Weapons are used against friends and family. It is as if people think that you can engage in Hollywood style mayhem and in the end only the bad guys suffer. The idea that the human body, especially the brain is extremely vulnerable and needs to be protected seems to be suspended. But that in itself is not the root cause of the problem.
Violence and aggression as a means to resolve interpersonal conflict has been with the human race since prehistoric times. I have found that Keeley offers the best historical account and analysis at the level of conflicting villages, city-states, and nations. His original intent was to dispel the notion of the noble savage or the peaceful prehistoric man living in an idyllic situation. He ends up showing that warfare has been a remarkably constant feature across time. From his text:
"According to the most extreme views, war is an inherent feature of human existence, a constant curse of all social life, or (in guise of a real war) a perversion of human sociability created by the centralized political structures of states and civilizations. In fact, cross cultural research on warfare has established that although some societies that did not engage in war or did so extremely rarely, the overwhelming majority of known societies (90-95%) have been involved in this activity." (p 27-28)
In reviewing some of the smaller pacifist pastoral societies, Keeley cites their low population density as well as their strong moral distaste for violence (p 31) as a likely reason that the Semai could return to a peaceful existence after being recruited by the British to fight against Communist insurgents in the 1950s. In his chapter "Crying Havoc-The Question of Causes", Keeley takes a fairly detailed look at how war starts as a combination of psychological and political factors starting off with a conflict between two villages where one village owed the other village a debt. He demonstrates how that that conflict escalates to the point of violence and death for several reasons. He cites prestige, theft, adultery, and poaching as common reasons for conflicts with aggression resulting in death. He concludes that the specific information from an archaeological standpoint is generally difficult to discern and considers broader contexts.
I think the implicit strength of Keeley's work is that he does have a lot of information on warfare and conflict in small and large societies and through all of that information the common thread is that humans resort to violence as a way to resolve conflict, even in situations that are relatively trivial and could easily be resolved by other means. I have made that observation repeatedly in clinical situations and the only exceptions are where the violence is driven by a psychiatric disorder. It is also obvious that learning other strategies can definitely occur often times for the worst possible reasons. An example is an aggressive man with antisocial personality disorder who typically gets what he wants by threatening or harming people. If he survives long enough, he may get to the point where that is a losing tactic and he becomes less aggressive with age. A more common example is the case of people referred to anger control groups through their contact with law enforcement or the courts. Many find that the strategies they learn in these groups are very effective.
So what is the real lesson in this case? The real lesson is that this violent confrontation did not need to occur. All of the energy being expended in the debate about who was the victim and whether or not legal penalties should be assigned misses that point. It should be fairly obvious that each side can construct a detailed narrative of what happened and how that should affect the outcome. My courtroom experience has left me with the impression that it is possible that neither narrative is an entirely accurate representation of what happened. Who would want their future decided by those circumstances?
All of the sensational coverage by the press misses even more widely. Solving conflicts between people by aggression and homicide is a strategy of primitive man. It arose out of a time before there was a legal system or designated police. It came from a time where there was no recognition that every person is unique and society may be less if that unique person is lost. Until there is the realization that violent confrontations are a toxic byproduct of of our prehistoric ancestors and that they are no longer necessary - there will continue to be unnecessary tragedies. Society is currently complex and aggression will never be a final solution. Coming up with better solutions at this point is the next logical step.
George Dawson, MD, DFAPA
Lawrence H. Keeley. War Before Civilization. Oxford University Press, 1997
Sunday, March 17, 2013
More on Homicide Prevention – LA County Style
I have been developing a theme of how to prevent homicide
and mass killing for more than a decade.
As previously
posted, I think that this needs to be done independent of the firearms issue
with a public health focus on both primary and secondary prevention. There have been a couple of developments
recently that I would like to highlight and whether or not they are consistent
with the public health approach.
The first is an article
in the NY Times today on a unique approach to school threat assessment and
intervention. The article describes LA
County’s School Threat Assessment
Response Team. Several threat
scenarios are described that trigger a multidisciplinary response from team members
representing law enforcement, school officials, and mental health. The way the program is described it is unique
in terms of engagement. Threats at
school generally result in one dimensional and fragmented approach to the
problem. The school has a protocol that
may result in suspension. Referral to
mental health providers is frequently a limiting step due to the lack of
appointments, insurance problems, or debate over whether the school system or
the health care system is responsible for assessment and treatment. This patchwork system is a set up for people
with severe problems falling through the cracks.
The LA County response is for the team to make a rapid same
day assessment at the point of the threat and at the student’s home including looking
at their room. How many times have we
read about the marginal teenager who is thrown out of school for threatening
behavior and they end up sitting in their room focused on the same thought
patterns or watching other forms of violent activity on the Internet or in
video games? Getting right into that
environment seems like a powerful intervention to me and one that is likely to
yield better results. The main reason
for failure in situations where a threat has been identified is that lack of follow
up. People who are threatening and aggressive are
not likely to care if they are thrown out of school and they are not likely to
follow through with mental health interventions. The response team also spends time educating
people about how to communicate in emergency situations where there are many
misunderstandings about confidentiality.
The LA approach is innovative and exactly what is needed to
assess and intervene in crisis situations involving threats and dangerous
behavior. In situation after situation,
tragedies occur when people people come to the attention of someone and there
is no clear map for assessment and treatment.
That is true in the school system, in colleges and universities, in the
workplace and in family situations. I have
personally talked with people who said that they either did not know what to do
or they actively tried several resources and were told that there were no appointments
available or that the person was not dangerous enough to treat and unless they
agreed to a voluntary assessment and treatment that nothing could be done. But it doesn’t stop at that point. I am also aware of situations where there
clearly was enough evidence that the person was dangerous enough to meet
criteria for an emergency assessment but it was not done of the person was
released for the emergency department.
In many of these cases there was an adverse outcome. What is the problem?
There is a significant bias against aggressive and violent
people. To some extent that bias is self
protective. Any reasonable adult knows
the obvious advantages of avoiding conflicts or even irrational behavior. There are always plenty of stories in the
news about the lack of Good Samaritans in situations where an aggressive act is
being perpetrated in public. Many
psychological explanations of this behavior are offered but I think the obvious
motivation is avoiding the conflict and possible injury.
That same code of silence often applies in cases where there have been
sudden changes in behavior and the person involved has a treatable
problem. A second level of bias is the
moralistic approach to aggressive and violent behavior that equates this
behavior with bad moral conduct. That
applies in situations where criminals use aggression to intimidate people and
get what they want. It does not apply when
the aggression is a symptom of mental illness.
The bias extends beyond members of the general public. The health care system is activated by a
legal concept called “dangerousness” or “imminent dangerousness”. Every state has different statutory requirements
and those statutes are interpreted on a highly variable basis across every
county in the state. In some counties it
comes down to some of the public officials involved seeing themselves as
protectors of people’s rights. In other
counties, assessment and treatment are more of a priority. At the level of the health care system there
is another layer of bias. The
overwhelming bias these days is that people should not be assessed or treated
in a psychiatric facility for more than 4 or 5 days and any assessment or
treatment should be kept to the bare minimum.
It is easy to find different clinicians make entirely different
decisions when presented with the same potentially dangerous patient. The end result is a patchwork of acute care
settings where people can go for help.
Because of all the biases involved unless an aggressive act has been
committed the likelihood of an intervention occurring is basically a coin toss.
That is why the LA County response is so important. It is an intervention that activates a
rational response to threats from people who are likely in distress and
possibly mentally ill. There is no dangerousness
standard initially and that is a critical departure from the current nonsystem. The goal of the LA County response is to
engage the person and their social network and not make a one-time assessment
and decide to admit or discharge the patient based on a dangerousness
concept. The LA County response is
unique in that it is based on behavior and the goal is to help the person
involved rather than decide on whether or not they should be committed. The overall approach is very similar to
community psychiatry case management teams except LA County teams seem to have
more latitude because they are not limited initially by commitment standards.
The is an excellent approach to the problem and I hope that
it is researched, expanded to mental health crisis teams and widely adopted if
effective. I don’t know why it would not
be effective.
George Dawson, MD, DFAPA
Erica Goode. Focusing
on Violence Before It Happens. NY Times
March 14, 2003.
Saturday, August 4, 2012
"Preventing Violence: Any Thoughts?"
The title of this post may look familiar because it was the title of a recent topic on the ShrinkRap blog. That is why I put it in quotes. I put in a post consistent with some the posts and articles I have written over the past couple of years on this topic. I know that violence, especially violence associated with mental illness can be prevented. It is one of the obvious jobs of psychiatrists and one of the dimensions that psychiatrists are supposed to assess on every one of their evaluations. It was my job in acute care setting for over 25 years and during that time I have assessed and treated all forms of violence and suicidal behavior. I have also talked with people after it was too late - after a homicide or suicide attempt had already occurred.
The responses to my post are instructive and I thought required a longer response than the brief back and forth on another blog. The arguments against me are basically:
1. You not only can't prevent violence but you are arrogant for suggesting it.
2. You really aren't interested in violence prevention but you are a cog machine of the police state and inpatient care is basically an extension of that.
3. You can treat aggressive people in an inpatient setting basically by oversedating them.
4. People who are mentally ill who have problems with violence and aggression aren't stigmatized any more than people with mental illness who are not aggressive.
These are all common arguments that I will discuss in some detail, but there is also an overarching dynamic and that is basically that psychiatrists are arrogant, inept, unskilled, add very little to the solution of this problem and should just keep quiet. All part of the zeitgeist that people get well in spite of psychiatrists not because of psychiatrists. Nobody would suggest that a Cardiologist with 25 years experience in treating acute cardiac conditions should not be involved in discussing public health measures to prevent acute cardiac disorders. Don't tell anyone that you are having chest pain? Don't call 911? Those are equivalent arguments. We are left with the curious situation where the psychiatrist is held to same medical level of accountability as other physicians but his/her opinion is not wanted. Instead we can listen to Presidential candidates and the talking heads all day long who have no training, no experience, no ideas, and they all say the same thing: "Nothing can be done."
It is also very interesting that nobody wants to address the H-bomb - my suggestion that there should be direct discussion of homicidal ideation. Homicidal ideation and behavior can be a symptom. There should be public education about this. Why no discussion? Fear of contagion? Where does my suggestion come from? Is anyone interested? I guess not. It is far easier to continue saying that nothing can be done. The media can talk about sexual behavior all day long. They can in some circumstances talk about suicide. But there is no discussion of violence and aggression other than to talk about what happened and who is to blame. That is exactly the wrong discussion when aggression is a symptom related to mental illness.
So what about the level of aggression that psychiatrists typically contain and what is the evidence that they may be successful. Any acute care psychiatric unit that sees patients who are taken involuntarily to an emergency department sees very high levels of aggression. That includes, threats, assaults, violent confrontations with the police, and actual homicide. The causes of this behavior are generally reversible because they are typically treatable mental illnesses or drug addiction or intoxication states. The news media likes to use the word "antisocial personality" as a cause and it can be, but people with that problem are typically not taken to a hospital. The police recognize their behavior as more goal oriented and they do not have signs and symptoms of mental illness. Once the psychiatric cause of the aggression is treated the threat of aggression is significantly diminished if not resolved.
In many cases people with severe psychiatric illnesses are treated on an involuntary basis. They are acutely symptomatic and do not recognize that their judgment is impaired. That places them at risk for ongoing aggression or self injury. Every state has a legal procedure for involuntary treatment based on that principle. The idea that involuntary treatment is necessary to preserve life has been established for a long time. Civil commitment and guardianship proceedings are recognition that treatment and in some cases emergency placement can be life saving solutions.
The environment required to contain and treat these problems is critical. It takes a cohesive treatment team that understands that the aggressive behavior that they are seeing is a symptom of mental illness. The meaning is much different than dealing with directed aggression by people with antisocial personalities who are intending to harm or intimidate for their own personal gain. That understanding is critical for every verbal and nonverbal interaction with aggressive patients. Aggression cannot be contained if the hospital is run by administrators who are not aware of the cohesion necessary to run these units and who do not depend on staff who have special knowledge in treating aggression. All of the staff working on these units have to be confident in their approach to aggression and comfortable being in these settings all day long.
Medication is frequently misunderstood in inpatient settings. In 25 years of practice it is still very common to hear that medication turns people into "zombies". Comments like: "I don't want to be turned into a zombie" or "You have turned everyone into zombies" are common. I remember the last comment very well because it was made by an observer who was looking at people who were not taking any medication. In fact, medication is used to treat acute symptoms and in this particular case symptoms that increase the risk of aggression. The medications typically used are not sedating. They cannot be because frequent discussions need to occur with the patient and a plan needs to be developed to reduce the risk of aggression in the future. An approach developed by Kroll and MacKenzie many years ago is still a good blueprint for the problem.
There is no group of people stigmatized more than those with mental illness and aggression. It is a Hollywood stereotype but I am not going to mention the movies. This group is also disenfranchised by advocates who are concerned that any focus on this problem will add stigma to the majority of people with mental illness who are not aggressive or violent. There are some organizations with an interest in preventing violence and aggression, but they are rare.
At some point in future generations there may be a more enlightened approach to the primitive thoughts about human consciousness, mental illness and aggression. For now the collective consciousness seems to be operating from a perspective that is not useful for science or public health purposes. There is no better example than aggression as a symptom needing treatment rather than incarceration and the need to identify that symptom as early as possible.
George Dawson, MD, DFAPA
The responses to my post are instructive and I thought required a longer response than the brief back and forth on another blog. The arguments against me are basically:
1. You not only can't prevent violence but you are arrogant for suggesting it.
2. You really aren't interested in violence prevention but you are a cog machine of the police state and inpatient care is basically an extension of that.
3. You can treat aggressive people in an inpatient setting basically by oversedating them.
4. People who are mentally ill who have problems with violence and aggression aren't stigmatized any more than people with mental illness who are not aggressive.
These are all common arguments that I will discuss in some detail, but there is also an overarching dynamic and that is basically that psychiatrists are arrogant, inept, unskilled, add very little to the solution of this problem and should just keep quiet. All part of the zeitgeist that people get well in spite of psychiatrists not because of psychiatrists. Nobody would suggest that a Cardiologist with 25 years experience in treating acute cardiac conditions should not be involved in discussing public health measures to prevent acute cardiac disorders. Don't tell anyone that you are having chest pain? Don't call 911? Those are equivalent arguments. We are left with the curious situation where the psychiatrist is held to same medical level of accountability as other physicians but his/her opinion is not wanted. Instead we can listen to Presidential candidates and the talking heads all day long who have no training, no experience, no ideas, and they all say the same thing: "Nothing can be done."
It is also very interesting that nobody wants to address the H-bomb - my suggestion that there should be direct discussion of homicidal ideation. Homicidal ideation and behavior can be a symptom. There should be public education about this. Why no discussion? Fear of contagion? Where does my suggestion come from? Is anyone interested? I guess not. It is far easier to continue saying that nothing can be done. The media can talk about sexual behavior all day long. They can in some circumstances talk about suicide. But there is no discussion of violence and aggression other than to talk about what happened and who is to blame. That is exactly the wrong discussion when aggression is a symptom related to mental illness.
So what about the level of aggression that psychiatrists typically contain and what is the evidence that they may be successful. Any acute care psychiatric unit that sees patients who are taken involuntarily to an emergency department sees very high levels of aggression. That includes, threats, assaults, violent confrontations with the police, and actual homicide. The causes of this behavior are generally reversible because they are typically treatable mental illnesses or drug addiction or intoxication states. The news media likes to use the word "antisocial personality" as a cause and it can be, but people with that problem are typically not taken to a hospital. The police recognize their behavior as more goal oriented and they do not have signs and symptoms of mental illness. Once the psychiatric cause of the aggression is treated the threat of aggression is significantly diminished if not resolved.
In many cases people with severe psychiatric illnesses are treated on an involuntary basis. They are acutely symptomatic and do not recognize that their judgment is impaired. That places them at risk for ongoing aggression or self injury. Every state has a legal procedure for involuntary treatment based on that principle. The idea that involuntary treatment is necessary to preserve life has been established for a long time. Civil commitment and guardianship proceedings are recognition that treatment and in some cases emergency placement can be life saving solutions.
The environment required to contain and treat these problems is critical. It takes a cohesive treatment team that understands that the aggressive behavior that they are seeing is a symptom of mental illness. The meaning is much different than dealing with directed aggression by people with antisocial personalities who are intending to harm or intimidate for their own personal gain. That understanding is critical for every verbal and nonverbal interaction with aggressive patients. Aggression cannot be contained if the hospital is run by administrators who are not aware of the cohesion necessary to run these units and who do not depend on staff who have special knowledge in treating aggression. All of the staff working on these units have to be confident in their approach to aggression and comfortable being in these settings all day long.
Medication is frequently misunderstood in inpatient settings. In 25 years of practice it is still very common to hear that medication turns people into "zombies". Comments like: "I don't want to be turned into a zombie" or "You have turned everyone into zombies" are common. I remember the last comment very well because it was made by an observer who was looking at people who were not taking any medication. In fact, medication is used to treat acute symptoms and in this particular case symptoms that increase the risk of aggression. The medications typically used are not sedating. They cannot be because frequent discussions need to occur with the patient and a plan needs to be developed to reduce the risk of aggression in the future. An approach developed by Kroll and MacKenzie many years ago is still a good blueprint for the problem.
There is no group of people stigmatized more than those with mental illness and aggression. It is a Hollywood stereotype but I am not going to mention the movies. This group is also disenfranchised by advocates who are concerned that any focus on this problem will add stigma to the majority of people with mental illness who are not aggressive or violent. There are some organizations with an interest in preventing violence and aggression, but they are rare.
At some point in future generations there may be a more enlightened approach to the primitive thoughts about human consciousness, mental illness and aggression. For now the collective consciousness seems to be operating from a perspective that is not useful for science or public health purposes. There is no better example than aggression as a symptom needing treatment rather than incarceration and the need to identify that symptom as early as possible.
George Dawson, MD, DFAPA
Saturday, July 21, 2012
Colorado Mass Shooting Day 2
I have been watching the media coverage of
the mass shooting incident today - Interviews of family members,
medical personnel and officials. I saw a trauma surgeon at one
of the receiving hospitals describe the current status of patients taken to
his hospital. He described this as a "mass casualty
incident". One reporter said that people don’t want insanity to
replace evil as a focus of the prosecution.
In an interview that I think surprised the interviewer, a family member talked about the significant impact on
her family. When asked about how she would "get her head around
this" she calmly explained that there are obvious
problems when a person can acquire this amount of firearms, ammunition, and
explosives in a short period of time. She went on to add that she works
in a school and is also aware of the fact that there are many children with
psychological problems who never get adequate help. She thought a lot of
that problem was a lack of adequate financing.
I have not listened to any right wing talk radio
today, but from the other side of the aisle the New York Times headline
this morning was "Gunman Kills 12 in Colorado, Reviving Gun Debate."
Mayor Bloomberg is quoted: “Maybe it’s time that the two people who
want to be president of the United States stand up and tell us what they are
going to do about it,” Mr. Bloomberg said during his weekly radio program,
“because this is obviously a problem across the country.”
How did the Presidential candidates respond?
They both pulled down the campaign ads and apparently put the
attack ads on hold. From the President today: " And if there’s
anything to take away from this tragedy, it’s a reminder that life is
fragile. Our time here is limited and it is precious. And what
matters in the end are not the small and trivial things which often consume our
lives. It’s how we choose to treat one another, and love one
another. It’s what we do on a daily basis to give our lives meaning and
to give our lives purpose. That’s what matters. That’s why we’re
here." A similar excerpt from Mitt Romney: "There will be
justice for those responsible, but that’s another matter for another day. Today
is a moment to grieve and to remember, to reach out and to help, to appreciate
our blessings in life. Each one of us will hold our kids a little closer,
linger a bit longer with a colleague or a neighbor, reach out to a family
member or friend. We’ll all spend a little less time thinking about the worries
of our day and more time wondering about how to help those who are in need of
compassion most."
These are the messages that we usually hear from
politicians in response to mass shooting incidents. At this point these messages are necessary, but the transition from this incident is as important. After the messages of condolences, shared grief, and
imminent justice that is usually all that happens. Will either candidate
respond to Mayor Bloomberg's challenge? Based on the accumulated history
to date it is doubtful.
A larger question is whether anything can be done apart from the reduced access to firearms argument. In other words, is there an approach to directly intervene with people who develop homicidal ideation? Popular consensus says no, but I think that it is much more likely than the repeal of the Second Amendment.
A larger question is whether anything can be done apart from the reduced access to firearms argument. In other words, is there an approach to directly intervene with people who develop homicidal ideation? Popular consensus says no, but I think that it is much more likely than the repeal of the Second Amendment.
George Dawson, MD, DFAPA
Barack Obama. Weekly
Address: Remembering the Victims of the Aurora Colorado Shooting.
July 21, 2012.
Mitt Romney. Remarks by Mitt
Romney on the Shooting in Aurora, Colorado. NYTimes July 20,
2012.
Friday, July 20, 2012
Mass shootings - How Many Will Be Tolerated?
I have been asking myself that question repeatedly for the past several decades. I summarized the problem a couple of months ago in this blog. In the 12 hour aftermath of the incident in Aurora, Colorado I have already seen the predictable patterns. Condolences from the President and the First Lady. Right wing talk radio focused on gun rights and how the liberals will predictably want to restrict access to high capacity firearms. Those same radio personalities talking about how you can never predict when these events will happen. They just do and they cannot be prevented. One major network encouraging viewers to tune in for more details on the "Batman Massacre."
We can expect more of the same over the next days to weeks and I will not expect any new solutions. Mass shootings are devastating for the families involved. They are also significant public health problems. There is a body of knowledge out there that has not been applied to prevent these incidents and these incidents have not been systematically studied. The principles in the commentary statement listed below still apply.
It is time to stop acting like this is a problem that cannot be solved.
George Dawson, MD, DFAPA
A Commentary Statement submitted to the StarTribune January 18, 2011 from the Minnesota Psychiatric Society, The Barbara Schneider Foundation, and SAVE - Suicide Awareness Voices of Education
We can expect more of the same over the next days to weeks and I will not expect any new solutions. Mass shootings are devastating for the families involved. They are also significant public health problems. There is a body of knowledge out there that has not been applied to prevent these incidents and these incidents have not been systematically studied. The principles in the commentary statement listed below still apply.
It is time to stop acting like this is a problem that cannot be solved.
George Dawson, MD, DFAPA
A Commentary Statement submitted to the StarTribune January 18, 2011 from the Minnesota Psychiatric Society, The Barbara Schneider Foundation, and SAVE - Suicide Awareness Voices of Education
Monday, March 5, 2012
Violence and Gunplay - Why Nobody is Informed by the Media Anymore
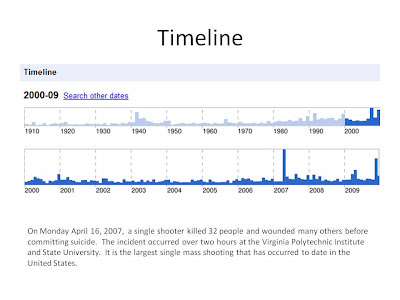
Mass shootings have been a phenomenon of my lifetime. I can still clearly remember the University at Texas-Austin shootings that occurred on August 6, 1966. A single gunman killed 16 people and wounded 32 while holed up on the observation deck of an administrative building until he was shot and killed by the police. I first read about it in Life magazine. All the pictures in those days were black and white. Some of those pictures are available online on sites such as "Top 10 School Massacres.” I generated this timeline of mass shootings when Google still had that feature in their search engine.
The problem of course is that the mass shootings never really stop. In the USA, the press is so used to them that they seem to have a protocol. Discuss the tragedy and whether or not the perpetrator was mentally ill, had undiagnosed problems or perhaps risk factors for aggression and violence. Discuss any heroic deeds. Make the unbelievable statement that the victims were "in the wrong place at the wrong time." And then move on as soon as possible. There is never a solution or even a call for finding one. It is like everyone has resigned themselves to to repetitive cycles of gunfire and death. It is clear that the press does not want to see it any other way.
When you are practicing psychiatry especially in emergency situations and hospitals, you need to be more practical. When I took the oral boards exams back in 1988 and subsequently when I was an examiner, one of the key dimensions that the examiners focused on was the assessment of dangerousness. Failing to explore that could be an exam failing mistake. Any psychiatric inpatient unit has aggression toward self or others as one of the main reasons for admission to acute care and forensic settings. With the recent fragmentation and rationing of psychiatric services, many people who would have been treated in hosptials are diverted to jails instead. That led one author to describe LA County jail as the country's largest psychiatric facility.
I have introduced the idea of looking for solutions into professional and political forums for over a decade now and it is always met with intense resistance. Some mental health advocates are threatened by the idea that it will further stigmatize the mentally ill as violent. Many people consider the problem to be hopeless. Others see it as the natural product of a heavily armed society and no matter what side you are on that argument - that is where the conversation ends.
In an attempt to reframe the issue so that this impasse could possibly be breached the Minnesota Psychiatric Society partnered with the the Barbara Schneider Foundation and SAVE Minnesota in the wake of a national shooting incident to suggest alternatives. Rather than speculate about psychiatric disorders or gun control we were focused on solutions that you can read through the link below.
The actual commentary was never published by the editor who apparently stated that there was a conflict of interest because we seemed to be fishing for research dollars. It appears that the press can only hear the cycle of tragedy, speculation about mental health problems, and the need to move on. The problem with that is that we continue to move on to another shooting.
George Dawson, MD
A Commentary Statement submitted to the StarTribune January 18, 2011 from the Minnesota Psychiatric Society, The Barbara Schneider Foundation, and SAVE - Suicide Awareness Voices of Education

When you are practicing psychiatry especially in emergency situations and hospitals, you need to be more practical. When I took the oral boards exams back in 1988 and subsequently when I was an examiner, one of the key dimensions that the examiners focused on was the assessment of dangerousness. Failing to explore that could be an exam failing mistake. Any psychiatric inpatient unit has aggression toward self or others as one of the main reasons for admission to acute care and forensic settings. With the recent fragmentation and rationing of psychiatric services, many people who would have been treated in hosptials are diverted to jails instead. That led one author to describe LA County jail as the country's largest psychiatric facility.
I have introduced the idea of looking for solutions into professional and political forums for over a decade now and it is always met with intense resistance. Some mental health advocates are threatened by the idea that it will further stigmatize the mentally ill as violent. Many people consider the problem to be hopeless. Others see it as the natural product of a heavily armed society and no matter what side you are on that argument - that is where the conversation ends.
In an attempt to reframe the issue so that this impasse could possibly be breached the Minnesota Psychiatric Society partnered with the the Barbara Schneider Foundation and SAVE Minnesota in the wake of a national shooting incident to suggest alternatives. Rather than speculate about psychiatric disorders or gun control we were focused on solutions that you can read through the link below.
The actual commentary was never published by the editor who apparently stated that there was a conflict of interest because we seemed to be fishing for research dollars. It appears that the press can only hear the cycle of tragedy, speculation about mental health problems, and the need to move on. The problem with that is that we continue to move on to another shooting.
George Dawson, MD
A Commentary Statement submitted to the StarTribune January 18, 2011 from the Minnesota Psychiatric Society, The Barbara Schneider Foundation, and SAVE - Suicide Awareness Voices of Education
Subscribe to:
Posts (Atom)