It was about 1989 and the era of satanic ritualistic abuse was born. I was in the middle of running a public health clinic on the northern fringe of the United States at the time and did not see any cases until I moved south to the Twin Cities (Minneapolis-St. Paul, MN). Showalter documents how the stories spread in the media until there was a fairly standard description of women "... forced to kill and eat babies at satanic ceremonies, about seeing children dismembered boiled an burned, about being drugged, tortured with cattle prods, branded with branding irons, raped with crucifixes and animal carcasses....." (p. 172). As the stories intensified prosecutions occurred in some areas based on these stories. After all, the alleged magnitude of these rituals would have left a significant amount of eye-witness and physical evidence. But it turned out that was never found. There were parallel phenomena of false prosecutions based on these accusations and ultimately malpractice cases against therapists making the diagnosis and proceeding with treatment on the basis of traumatic events that had never occurred and seemed to be introduced as a result of the therapy.
I started to see the initial traces of the multiple personality epidemic at my new job, and recall two distinct reactions from psychiatrists involved with these folks. But before I get into that, a little background about psychiatric interviewing is in order. In this era of rapid checklist diagnoses, it may be difficult to believe that psychiatrists are actually trained to interview people and question what they hear. The questions naturally come up for a number of reasons. The first has to do with how accurate the patient seems to be able to recall the history. That leads to associated questions about any inability to recall the history. The second has to do with common distortions that patients have in their perception of reality. Those distortions may occur at a neurotic or a psychotic level of consciousness. In the initial interview the focus is on understanding the patient's mental state to the point that if it was repeated back to the person they would agree with the interpretation. That interview process can be interrupted for any number of reasons along the way, ranging from cognitive disorganization to paranoid psychosis and aggressive behavior. It is important to keep in mind that the interview is a dynamic process that has elements far beyond a checklist or list of symptoms in DSM-5. Reading about confabulation is not the same thing as having assessed hundreds of patients with that problem. That assessment flows from the initial question in the mind of the psychiatrist: "Is this confabulation?' and noting all of the features in the interview situation to support or refute that question.
Of the psychiatrists I was affiliated with at the time, a few believed that there was such a diagnostic entity as dissociative identity disorder but the majority (as in >90%) did not. The psychiatric literature as early as 1988 doubted the existence of the disorder and suggested that it was iatrogenic. I can recall a journal club discussion we had about a British Journal of Psychiatry article that was not only skeptical of the diagnosis but suggested that it was iatrogenic. It seemed like a geographically based movement and in order to make the diagnoses and treat people you had to be trained by very specific people. Even though the diagnostic criteria were fairly straightforward it seemed like you needed the attend the appropriate seminars in order to make the diagnosis. You definitely did if you expected to proceed with treatment and even then it was unclear about how much additional training was necessary. I had the impression that most people affected had moderate to severe personality disorders and they could be approached using standard techniques. That approach was highly successful in stabilizing people in acute care and transitioning them to outpatient settings. The diagnosis could be reinforced by the time patients presented to a tertiary care center. Any hint of skepticism on the part of the attending physician could precipitate intense reactions if the patients thought they were not believed. That usually threatened any therapeutic relationship, created staff splitting, and great pressure on psychiatrists to accept the diagnosis and whatever the current treatment plan was at the time. There was also the novelty of the diagnosis that held a certain fascination for anyone who could not see that there was more heat than light.
At the time I was dutifully reading volumes of the Annual Review of Psychiatry and completing the CME questions. Volume 10 had an entire section on Dissociative Disorders with some optimistic introductory lines (p 143):
"Dissociation is here to stay. The chapters that follow indicate there is a growing body of clinical observation and research documenting the prevalence, phenomenology, psychophysiology, and treatment of dissociation."
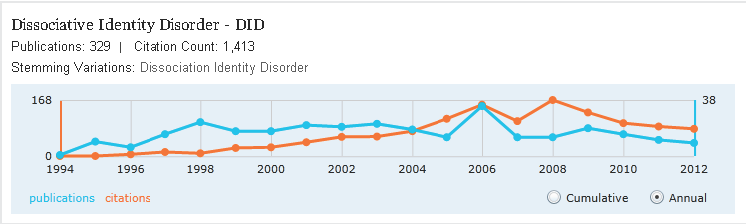
What happened instead was a flattening of publications as indicated by this Microsoft academic search and the end of a specialty journal (click to enlarge)
Despite the solid review that SRA probably did not exist, some bizarre reports began to surface. According to Elaine Showalter's book Hystories: hysterical epidemics and modern media:
"....almost half the patients.......were "reporting vividly detailed memories of cannibalistic revels and extensive experiences such as being used by cults during adolescence as serial baby breeders for ritual sacrifices."
My position on the subject has always been the position quoted by Elaine Showalter in her excellent book Hystories: hysterical epidemics and modern media. That position is all of these events never happened. But I took it one step further. Near the end of the decade, I contacted the author to see if she had any updated information. She did not and so I put in a Freedom of Information Act request for all of the information suggested in the book - specifically the results of of the investigations by Kenneth V. Lanning, then Special Agent of the FBI Behavioral Science Unit in Quantico, Virginia. I have previously listed problems with FOIA requests to the FBI and this was no exception. I was looking for the results of 300 case investigations that were all negative. After sending in the request through proper channels I was told that the information did not exist. In the 2000s, that report surfaced on the Internet, but it is still difficult to find a reliable copy.
I invite any reader to place themselves in the position of interviewing a person making claims, like the statements made in paragraph two of this post. Keep in mind that these patients are generally talking about local geography that everyone is aware of and the descriptions involve fairly massive abuse and homicide of large numbers of people. Even an untrained interviewer should have a degree of skepticism based on the fact that there have not been large numbers of missing persons and when these reports invariably get to local law enforcement, no hard evidence of a crime can be found. The reports did create considerable confusion among family members, prosecuting attorneys, inpatient staff and some psychiatrists but in the end even the psychiatrists who thought the SRA phenomenon was real realized that it was a distortion.
In answer to the idea that this era needs to be "reopened" I guess it depends on the intent. If the intent to illustrate once again that some or all psychiatrists are fools - there is more than enough propaganda out there already for the detractors of psychiatry to use. My perspective is that not only were the vast majority of psychiatrists not fooled by this phenomena there were articles at the time accurately describing the problem as a non-specific diagnosis and an iatrogenic problem and what to do about it. I would also question the applicability of the term moral panic. The phrase seems a bit too strong. It could apply in very small areas, but the majority of people in any community were generally unaware of the stories that were being told to psychiatrists in that era. If people were aware there would have been a larger buzz created by the media asking clinicians for examples and an analysis of the event. I suppose it would have been interesting to see what the local investigative news team found out if they were directed to a site where ritualistic abuse was alleged to have occurred. I would also not forget that in the majority of cases there were no attempted prosecutions. I think the moral panic was forgotten because for most people it was under their radar rather than a cataclysmic event like the Influenza Pandemic of 1918 where people were dropping dead in the streets. There were also psychiatrists at the time who investigated the issue of repression and false memory syndrome and became an asset to families affected by the hysteria. I would Showalter's book for a good discussion of the cultural determinants of the problem (there were many). If the suggestion is to reopen the issue with the appropriate perspective that it was a controversial and erroneous phenomenon that in some cases hurt individuals and families rather than a moral panic, that mistakes were made, and for the purpose of teaching appropriate evaluations and interviewing technique, then I am all for it. In addition to diagnostic issues, the area of dissociation and trauma in general also have treatment implications. Psychiatric residents need to know how to plan and conduct therapy on affected individuals, particularly since the main part of that treatment does not involve medications. They also need to know how to interview people without introducing artifacts as part of the interview process.
If the Psychiatric Times has pulled the original article, it probably makes sense to write a book or a review article for a journal less concerned about litigation. There are a number of public access online journals that I am sure would be willing to publish the article and probably consider a theme issue on the topic.
George Dawson, MD, DFAPA
Elaine Showalter. Hystories: hysterical epidemics and modern media. Columbia University Press. New York, 1997.
Merskey H. Multiple personality disorder and false memory syndrome. Br J Psychiatry. 1995 Mar;166(3):281-3. PubMed PMID: 7788115.
Piper A Jr. Multiple personality disorder. Br J Psychiatry. 1994 May;164(5):600-12. Review. PubMed PMID: 7921709.
Supplementary 1:
From Merskey 20 years ago:
"It has been all right to treat patients on the basis of dynamic notions of repression so long as the concept was only one which was exchanged between therapist and patient and merely served to revise, in a positive fashion, the patient's view of himself or herself in the world. Using repression as an idea which works to the detriment of other people, disrupts families, wipes out the life savings of parents, abolishes their contact with children and grandchildren, and embroils some in painful legal battles, is another matter altogether and not compatible with the old principle "first do no harm"."
From Piper 20 years ago:
"However, there is a profound difference between standard psychiatric interview procedures -where practitioners take great care not to bias patients' reports-and the techniques and treatment espoused by the leading contributors in the MPD field. It is absurd to maintain that those techniques are not vehicles of grossly overt suggestion to patients. It is equally absurd to believe that in any other branch of psychiatry, one would see a clinician prodding a schizophrenic patient to produce more voices, or taking part in a 4 hour interview with a patient who might possibly be bulimic to suggest more frequent binging."
Supplementary 2: To this day I have not been able to locate a copy on any FBI report describing the investigation of 300 case reports of alleged SRA activity. My FOIA experience with the FBI is very negative and it is clear to me that if they don't want to give you information you will not get it. If anyone has this report consider sending me a copy.
Supplementary 3: The Psychiatric Times decided to publish an edited version of Nolls original article today. That is certainly the preferable course. Their rationale:
"Editorial Note: In light of the responses we have received regarding this article by Richard Noll, PhD, that was posted on our website on December 6, 2013, the article has been reposted with a modification. Additionally, we are posting responses from certain of the individuals mentioned in the article and from Dr. Noll in order to leave analysis of the article up to our readers"
From Merskey 20 years ago:
"It has been all right to treat patients on the basis of dynamic notions of repression so long as the concept was only one which was exchanged between therapist and patient and merely served to revise, in a positive fashion, the patient's view of himself or herself in the world. Using repression as an idea which works to the detriment of other people, disrupts families, wipes out the life savings of parents, abolishes their contact with children and grandchildren, and embroils some in painful legal battles, is another matter altogether and not compatible with the old principle "first do no harm"."
From Piper 20 years ago:
"However, there is a profound difference between standard psychiatric interview procedures -where practitioners take great care not to bias patients' reports-and the techniques and treatment espoused by the leading contributors in the MPD field. It is absurd to maintain that those techniques are not vehicles of grossly overt suggestion to patients. It is equally absurd to believe that in any other branch of psychiatry, one would see a clinician prodding a schizophrenic patient to produce more voices, or taking part in a 4 hour interview with a patient who might possibly be bulimic to suggest more frequent binging."
Supplementary 2: To this day I have not been able to locate a copy on any FBI report describing the investigation of 300 case reports of alleged SRA activity. My FOIA experience with the FBI is very negative and it is clear to me that if they don't want to give you information you will not get it. If anyone has this report consider sending me a copy.
Supplementary 3: The Psychiatric Times decided to publish an edited version of Nolls original article today. That is certainly the preferable course. Their rationale:
"Editorial Note: In light of the responses we have received regarding this article by Richard Noll, PhD, that was posted on our website on December 6, 2013, the article has been reposted with a modification. Additionally, we are posting responses from certain of the individuals mentioned in the article and from Dr. Noll in order to leave analysis of the article up to our readers"