
The AHRQ was started 30 years ago in 1999 when it was renamed from the Agency for Health Care Policy and Research (AHCPR) to the Agency for Healthcare Research and Quality (AHRQ) by legislative action. I have referenced their guidelines on this blog for ADHD and depression. The post on the depression guideline illustrated that AHCPR guidelines were generally of higher quality than the current managed care guidelines and screening guidelines.
Even looking at the web site today before it is taken down illustrates the depth of research and recommendation on the site. A search for psychiatry yields 600 references including research and policy recommendations. Interesting the guidelines at guidelines.gov has 74 psychiatric guidelines ranging from depression in children and adolescents to a guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. A wide number of physician and nonphysician organizations have produced the guidelines. These are unique sites with few comparable sites in the world. Only the National Institute for Health and Care Excellence (NICE) in the UK seems similar. The NICE guidelines are produced by a more uniform methodology rather than disparate organizations.
When the current administration announced it was defunding AHRQ guidelines, there was some hope that someone else would take it over - at least the existing databases. Some physician professional organizations were suggested. Given the government's shaky history of ancient information technology and dubious failed upgrades, I am speculating that would be the reason why nobody else would want to take that on. Clearly nobody in the administration is interested in a smooth transition. The smoothest transition I can think of would be to make the data available through the National Library of Medicine and their collection of databases. But as I type this there are about 8 hours to make that transition.
There are several serious questions for the Trump administration. Some are speculative, but when people question how doctors are influenced by a slice of pizza, I think it is reasonable to ask about health care corporations that are influenced by tens to hundreds of billions of dollars and how they influence politicians.
1. How does it make sense to take this data and these initiatives offline when the costs are trivial compared to other government projects?
Cost analyses have been done showing not much of a price increase corrected for inflation. Various analyses have been suggested such as this one pointed out the agency's role in reducing hospital infections resulting in 124,000 fewer fatalities per year a cost saving of about $28 billion.
2. And possibly even more important - what are the conflicts of interest involved?
The most significant one that I can see is that industry guidelines and standards go unchecked. There are any number of groups that are primarily comprised of health care executives that are producing standards of care that have nothing to do with medical practice or standards. Review practices by pharmaceutical benefit managers come under the same category. These physician intimidation strategies have nothing to do the scientific evidence or quality of care. In this regard the wholesale suspension of guidelines that counter industry practices are suddenly gone. It is far easier to do than reverse Environmental Protection Agency (EPA) regulations - but the zeitgeist is the same.
Taking down AHRQ means there is one less place in government healthcare sites with the word quality. I don't think that is an accident either. Today's healthcare industry would rather advertise how they are the best without using the quality word or any scientifically valid metrics.
3. As a corollary to the above - what about the professional guidelines that are collated and listed on the site?
I don't have the time to follow other physician professional organizations but the American Psychiatric Association has fallen off greatly over the years. Critical issues have not been addressed in some cases for decades. The commonest cause for this problem is cited as the expense it takes to collect all of the experts and data, but in the information age it would seem to be easier than ever. I speculate the the real reason is that these guidelines are just ignored. Why produce a hundred page guideline on all the aspects of the treatment of depression when the dominant managed care standard is a 2 minute screening exam and an antidepressant prescription? Why produce that document when it affects only 5% of the work force for mental disorders? Why produce that document when the psychiatrists involved have so little political leverage against the industry and the government that they can never use it.
AHRQ at least provided a broader forum for discussion.
4. Why the minimal notification and lack of feedback?
There are so many guidelines and so much information available on this site, it is impossible to know who is using it all and for what purpose. Unilaterally taking down a resource like this with 4 months notice has to be considered nothing more than a political decision at this point. If the number of people and organizations accessing this site was published somewhere - I have never seen it.
5. What about the Centers for Medicare and Medicaid services, the CMS web site?
Since CMS is essentially the billing and regulatory web site for Medicare - I don't think it is any danger of being shut down. But it does promote and spread a lot of unscientific information that is biased toward running the business side of health care at the expense of the medical side. It is a massive bureaucracy that is responsible for the bulk of physicians paperwork burden every day. Some clear evidence for the lack of science is psychiatric diagnosis related groups and how they don't accurately reflect diagnoses or the expected course of treatment for hospitalized psychiatric patients. The most recent post on this blog looks at the rationing of inpatient psychiatric services and how a lot of that has resulted from CMS regulation. Just a few years ago, I wrote a blog piece about a 55 page CMS document about what psychiatrists would have to do to document the diagnosis and treatment of depression. That was subsequently taken down.
Even looking at the web site today before it is taken down illustrates the depth of research and recommendation on the site. A search for psychiatry yields 600 references including research and policy recommendations. Interesting the guidelines at guidelines.gov has 74 psychiatric guidelines ranging from depression in children and adolescents to a guideline for CYP2D6 and CYP2C19 genotypes and dosing of tricyclic antidepressants. A wide number of physician and nonphysician organizations have produced the guidelines. These are unique sites with few comparable sites in the world. Only the National Institute for Health and Care Excellence (NICE) in the UK seems similar. The NICE guidelines are produced by a more uniform methodology rather than disparate organizations.
When the current administration announced it was defunding AHRQ guidelines, there was some hope that someone else would take it over - at least the existing databases. Some physician professional organizations were suggested. Given the government's shaky history of ancient information technology and dubious failed upgrades, I am speculating that would be the reason why nobody else would want to take that on. Clearly nobody in the administration is interested in a smooth transition. The smoothest transition I can think of would be to make the data available through the National Library of Medicine and their collection of databases. But as I type this there are about 8 hours to make that transition.
There are several serious questions for the Trump administration. Some are speculative, but when people question how doctors are influenced by a slice of pizza, I think it is reasonable to ask about health care corporations that are influenced by tens to hundreds of billions of dollars and how they influence politicians.
1. How does it make sense to take this data and these initiatives offline when the costs are trivial compared to other government projects?
Cost analyses have been done showing not much of a price increase corrected for inflation. Various analyses have been suggested such as this one pointed out the agency's role in reducing hospital infections resulting in 124,000 fewer fatalities per year a cost saving of about $28 billion.
2. And possibly even more important - what are the conflicts of interest involved?
The most significant one that I can see is that industry guidelines and standards go unchecked. There are any number of groups that are primarily comprised of health care executives that are producing standards of care that have nothing to do with medical practice or standards. Review practices by pharmaceutical benefit managers come under the same category. These physician intimidation strategies have nothing to do the scientific evidence or quality of care. In this regard the wholesale suspension of guidelines that counter industry practices are suddenly gone. It is far easier to do than reverse Environmental Protection Agency (EPA) regulations - but the zeitgeist is the same.
Taking down AHRQ means there is one less place in government healthcare sites with the word quality. I don't think that is an accident either. Today's healthcare industry would rather advertise how they are the best without using the quality word or any scientifically valid metrics.
3. As a corollary to the above - what about the professional guidelines that are collated and listed on the site?
I don't have the time to follow other physician professional organizations but the American Psychiatric Association has fallen off greatly over the years. Critical issues have not been addressed in some cases for decades. The commonest cause for this problem is cited as the expense it takes to collect all of the experts and data, but in the information age it would seem to be easier than ever. I speculate the the real reason is that these guidelines are just ignored. Why produce a hundred page guideline on all the aspects of the treatment of depression when the dominant managed care standard is a 2 minute screening exam and an antidepressant prescription? Why produce that document when it affects only 5% of the work force for mental disorders? Why produce that document when the psychiatrists involved have so little political leverage against the industry and the government that they can never use it.
AHRQ at least provided a broader forum for discussion.
4. Why the minimal notification and lack of feedback?
There are so many guidelines and so much information available on this site, it is impossible to know who is using it all and for what purpose. Unilaterally taking down a resource like this with 4 months notice has to be considered nothing more than a political decision at this point. If the number of people and organizations accessing this site was published somewhere - I have never seen it.
5. What about the Centers for Medicare and Medicaid services, the CMS web site?
Since CMS is essentially the billing and regulatory web site for Medicare - I don't think it is any danger of being shut down. But it does promote and spread a lot of unscientific information that is biased toward running the business side of health care at the expense of the medical side. It is a massive bureaucracy that is responsible for the bulk of physicians paperwork burden every day. Some clear evidence for the lack of science is psychiatric diagnosis related groups and how they don't accurately reflect diagnoses or the expected course of treatment for hospitalized psychiatric patients. The most recent post on this blog looks at the rationing of inpatient psychiatric services and how a lot of that has resulted from CMS regulation. Just a few years ago, I wrote a blog piece about a 55 page CMS document about what psychiatrists would have to do to document the diagnosis and treatment of depression. That was subsequently taken down.
6. Finally what does this imply for other federally funded information programs?
My biggest concern in this era of massive profits for publishers is the National Library of Medicine (NLM) - commonly used by physicians offices on a daily basis. It is a major resource for researchers, but it is also becoming a competitor for profitable online publishers. If research is publicly funded - a copy is accessible without charge on the PubMed web site. Will the day come when for profit medical publishers have enough leverage to put the NLM out of business? Stranger things have happened.
It is easy to blame that President Trump. He is heading the first blatantly anti-science and pro-business administration that I can recall in my decades of existence. But the reality is that the American healthcare system has been designed by an endless stream of bad decisions for the past 30 years all occurring in the confluence of special interest politics and massive special interest money with a little medical science (and a few doctors) sprinkled in. The press seems to focus on the influence of pharmaceutical companies, but the bulk of those bad decisions have been rationing decisions by the managed care industry.
George Dawson, MD, DFAPA
References:
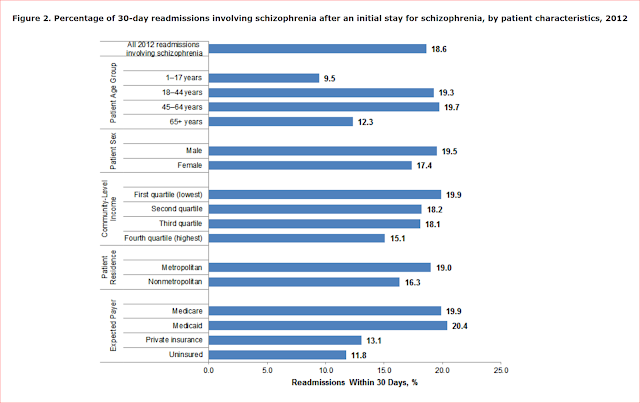
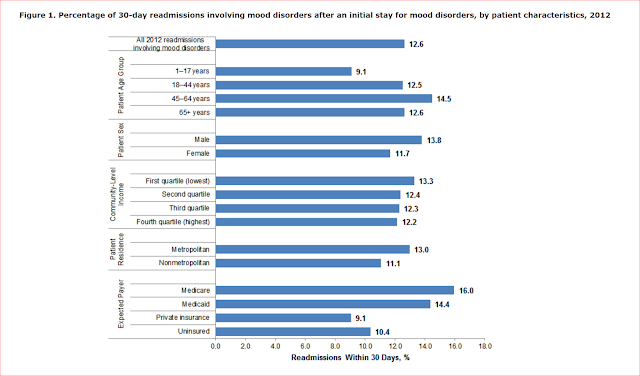
1: Heslin KC (AHRQ), Weiss AJ (Truven Health Analytics). Hospital Readmissions Involving Psychiatric Disorders, 2012. HCUP Statistical Brief #189. May 2015. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb189-Hospital-Readmissions-Psychiatric-Disorders-2012.pdf.
Supplementary:
I pulled the following figures on lengths of stay for mood disorders and schizophrenia out of the above article. If the site goes down at midnight this may be the only place that you can find it and any paper referencing it may lead to a dead end.
Updates:
07/16/2018: 3:30 PM AHRQ.gov web site is up and running at this point but guidelines.gov is not found.
Supplementary:
I pulled the following figures on lengths of stay for mood disorders and schizophrenia out of the above article. If the site goes down at midnight this may be the only place that you can find it and any paper referencing it may lead to a dead end.


Updates:
07/16/2018: 3:30 PM AHRQ.gov web site is up and running at this point but guidelines.gov is not found.