Although the media can certainly pump up the volume on trivia like the DSM-5 their coverage of the critical day-to-day issues involving mental illness continue to be lacking in both depth and breadth. It is weak. From a depth perspective I will point to an article about a man convicted of shooting at people on the I-96 freeway in southeastern Michigan. His reason for the shootings? He thought he was getting coded messages from the Detroit Tigers to shoot people. He also believed that military helicopters were hovering above his home and that his home contained "advanced technologies" that caused his daughter to develop a skin disease and his wife have a miscarriage. The article contains a layman's description of a not guilty by reason of mental disorder defense and that defense was never advanced based on a judges ruling. As a psychiatrist familiar with these criteria there is an overwhelming bias to convict people who are mentally ill and mentally compromised. That is why the defense is generally a failure. In this case the defendant did not have the opportunity to present that defense because as the article explains:
"Diminished capacity is a claim that says a defendant was unable to form specific intent required to commit a crime under the law by reason of mental illness, and as a result, the defendant’s responsibility in the alleged crime is diminished. The judge earlier ruled that the defense could not make this argument because it failed to give proper notice of a defense of insanity."
In other portions of the article we learn that he has been treated for an unnamed mental illness since 2009. The symptoms are described as delusions that respond to medication and the delusions associated with the shooting incidents are currently in remission. When the defendant is asked about whether he knew that firing a gun into an automobile might hurt someone. His response was "In hindsight - yes". I have not seen the final sentencing after a no contest plea but he faces up to 12 years in prison on firearms and assault charges after they decided to drop a terrorism charge.
From a breadth of coverage perspective, I will suggest a second article that points out the critical shortage in acute care inpatient beds with the capacity to address severe mental illness and aggressive behavior. In those case Virginia State Senator Creigh Deeds discusses an incident where his son stabbed him and subsequently shot himself. After the incident Senator Deeds states that the read his son's diary and it said that if he killed his father he would go directly to heaven. In his taped discussion he talks about all of the relevant points that I try to cover here involving stigma, a lack of respect for providers, and diversion of resources to more areas of care that are viewed as more prestigious - like Cardiology. Amazingly, Virginia apparently has a rule where you must be released from the emergency department if they can't find a psychiatric bed within 6 hours. Based on his proposed reforms it doesn't seem like there has to be much of an effort to look elsewhere. The sequence of events has been managed care companies shutting down psychiatric bed capacity by defunding it. That is followed by states deciding to act like managed care companies and either shutting down their capacity or getting completely out of the field. The end result is a pool of people who cycle in and out of short stays on inpatient units to overcrowded emergency departments to the street and back again. Many permanently drop out of that cycle when they become homeless or go to America's newest mental hospitals - the county jail. This is a problem everywhere in the United States. I used to qualify that by saying it was a problem in areas of high managed care penetration. Today that is everywhere.
Apart from the isolated pieces that are written with the obvious intent to get somebody a Pulitzer Prize, these stories are typical of what you see in the press. The first article lacks basic information on what mental illness is and how decision making in a delusional state bears no resemblance to answering questions "in hindsight" after the delusions are gone. It lacks psychiatric perspective. Any newspaper reporter probably has access to acute care psychiatrists to tell them about those problems. In that situation reporters always want a "diagnosis" of the person in the news and psychiatrists cannot speculate on that without having examined the patient and getting their release for that information. But they can provide a rich perspective based on their clinical experience treating thousands of similar problems and the effect of delusions on a person's conscious state. They can also provide an opinion on the mental illness defense in this country as well as the state of psychiatric services to treat the problem. I know that I would be happy to provide those details. At the minimum somebody in charge of journalism school curricula needs to examine how reporters can come out and ignore all of those facts. I might even suggest objective criteria for coverage as at least 5 times the words used to cover the least relevant mental illness story that year. I would give the least relevant story this year as anything having to do with the DSM-5. On that basis a lot of additional writing needs to be done on these two stories.
In the case of Senator Deeds, his analysis of the problem in this brief soundbite is spot on. He needs a broader platform to advocate for his plan and support against the people who are opposing him and the 6 hour rule in state of Virginia. He should work the the American Psychiatric Association, receive their support, and have access to their social media venues. The APA should come out with their own solution to this problem. I cannot think of anything more absurd and more consistent with a managed business approach to treating severe health problems than this 6 hour rule. At some point the patient and their severe problem is totally meaningless relative to business concerns. And Senator Deeds is right. That doesn't happen with any other medical problem in the emergency department.
It only happens with mental illness.
George Dawson, MD, DFAPA
Thursday, January 30, 2014
Tuesday, January 28, 2014
Is Bullshit A Better Term Than Antipsychiatry?
I saw Professor Harry G. Frankfurt on David Letterman a few years ago. He was there to explain his recently released book entitled On Bullshit. He was joking with Dave about how somebody called him up one day and wanted to make one of his essays into a book. When asked how that happens he said "Bigger fonts and wider margins." I don't know if he was consciously trying to convey the idea that he was no bullshitter. In the book he is listed as a renowned moral philosopher and Professor of Philosophy Emeritus at Princeton University. The book is inexpensive and a quick read. Imagine an essay stretched into a book the size of an address book in 67 pages of 12 point font and 1 inch margins.
Despite the catchy title and obvious magic of marketing, I really like this book. First off, it is written by a professor of moral philosophy and I always like hearing from the experts. Secondly, Professor Frankfurt looks at the differences between lying and bullshitting and all points in between. The opening line is classic:
"One of the most salient features of our culture is that there is so much bullshit." (p. 1)
In the opening paragraph he goes on to explain that study of bullshit has not attracted much attention because most people take it for granted that they can recognize it and not get taken in. The result is a lack of theoretical understanding of bullshit. His stated goal is to articulate what it is and what it is not.
I will let any interested reader acquire a copy of the book. With its brevity I run the risk of reciting all of the high points in this post. I will quote two more lines from the book because of the amount of information they convey:
"The realms of advertising and of public relations, and the nowadays closely related realm of politics are replete with instances of bullshit so unmitigated that they can serve among the most indisputable and classic paradigms of the concept." (p. 22)
Professor Frankfurt goes on to develop the idea that the bullshitter can be imprecise and that unlike a liar he has no prerequisite that he knows the truth. He is bluffing and faking his way through. Bullshitters don't reject the truth, they pay no attention to it. In the technical sense, bullshit is not false it is phony. And perhaps the essence as it applies to a professional field (I have to use a third quote):
"Bullshitting is unavoidable whenever circumstances require someone to talk without knowing what he is talking about." (p. 63).
The last requirement is interesting because there are conscious and unconscious components. The unconscious component is the innate ability that most people have to practice folk psychology. It is the equivalent of a social brain. We recognize certain patterns in people and how they behave that allow us to make predictions about their behavior. I am quite sure that many people mistake that ability for being trained as a psychiatrist. I base that a lot on what people tell me that they "observe" and "diagnose". For all of the concern about the "medicalization" of the population - the average folk psychologist has a much lower threshold than any psychiatrist I have ever met. For example, in various workplaces I have been warned by employee supervisors that three separate coworkers that I would be working with were "paranoid", "obsessive compulsive" and "borderline". I did not see any characteristics that the amateur diagnosticians warned me about and in all three cases, I found these co workers to be excellent and had absolutely no problems working with them. This is probably an extension of Dr. Frankfurt's work - the unconscious aspects of bullshitting but I expect that it correlates closely with some descriptions in a classic paper on prevarication.
But in the case of talking without expertise, I am afraid that the unconscious aspects cover a very small part of the bullshitting spectrum. You can go to any site where psychiatry is routinely criticized, attacked or vilified and you will see any number of posts by the anonymous posters who talk about their anecdotes and proclamations about psychiatry. Many are bombastic. None are challenged. It is the general tenor of many of these sites that psychiatrists are basically incompetent assholes (yeah I said it) and should be barred from practicing medicine. Psychiatrists only injure people and have never helped anyone. If they produce any coherent arguments they generally fit the psychiatrist as bogeyman dynamic that I previously described. Some people who have seen a psychiatrist may grudgingly admit it, but nobody ever seems to acknowledge that a psychiatrist did anything to help them. The more erudite approach may be to critique psychiatry without acknowledging that psychiatrists in fact are better critics and have critiqued their own field. If anyone is questioned they may produce the indignant response: "Are you calling me an antipsychiatrist?"
Some of what passes for criticism actually ignores what really happened and attempts to cast modern psychiatry in a light that is based more on historical spin than what is applicable today. Some of these efforts are actually considered to be "good" criticism, even though it is clear to any trained psychiatrist that the author knows little to nothing about the field. You would think that anyone interested in developing a negative narrative about psychiatry would do the basic research of picking up a copy of Shorter's A History of Psychiatry and reading about the ways things were before there was any psychiatry. In his text Shorter describes severe mental illness as a death sentence (p. 2) and the following historical observation: "In a world without psychiatry, rather than being tolerated or indulged, the mentally ill were treated with a savage lack of feeling. Before the advent of the therapeutic asylum, there was no golden era, no idyllic refuge for those deviant from the values of capitalism. To maintain otherwise is a fantasy." (p. 4). But the ignorance of psychiatry extends far beyond the historical. It is apparent that many of the critics have no knowledge of the current current psychiatric literature. They often reference the New York Times as though it is authoritative. They criticize highly technical subjects and it is apparent that they have not read a journal or a book from that field. Like Frankfurt's definition they pay no attention to the truth.
Based on Professor Frankfurt's essay, I conclude that bullshit is a much more appropriate characterization of many of the misrepresentations of psychiatry. I would also suggest it may be more politically correct than implying that the author is a member of a cult or a school of philosophy. (see the footnote at this link)
They are quite simply a bullshitter and bullshit remains as it always has been (even pre-Frankfurt) - bullshit.
George Dawson, MD, DFAPA
Harry G. Frankfurt. On Bullshit. Princeton University Press, Princeton, NJ, 2005.
Despite the catchy title and obvious magic of marketing, I really like this book. First off, it is written by a professor of moral philosophy and I always like hearing from the experts. Secondly, Professor Frankfurt looks at the differences between lying and bullshitting and all points in between. The opening line is classic:
"One of the most salient features of our culture is that there is so much bullshit." (p. 1)
In the opening paragraph he goes on to explain that study of bullshit has not attracted much attention because most people take it for granted that they can recognize it and not get taken in. The result is a lack of theoretical understanding of bullshit. His stated goal is to articulate what it is and what it is not.
I will let any interested reader acquire a copy of the book. With its brevity I run the risk of reciting all of the high points in this post. I will quote two more lines from the book because of the amount of information they convey:
"The realms of advertising and of public relations, and the nowadays closely related realm of politics are replete with instances of bullshit so unmitigated that they can serve among the most indisputable and classic paradigms of the concept." (p. 22)
Professor Frankfurt goes on to develop the idea that the bullshitter can be imprecise and that unlike a liar he has no prerequisite that he knows the truth. He is bluffing and faking his way through. Bullshitters don't reject the truth, they pay no attention to it. In the technical sense, bullshit is not false it is phony. And perhaps the essence as it applies to a professional field (I have to use a third quote):
"Bullshitting is unavoidable whenever circumstances require someone to talk without knowing what he is talking about." (p. 63).
The last requirement is interesting because there are conscious and unconscious components. The unconscious component is the innate ability that most people have to practice folk psychology. It is the equivalent of a social brain. We recognize certain patterns in people and how they behave that allow us to make predictions about their behavior. I am quite sure that many people mistake that ability for being trained as a psychiatrist. I base that a lot on what people tell me that they "observe" and "diagnose". For all of the concern about the "medicalization" of the population - the average folk psychologist has a much lower threshold than any psychiatrist I have ever met. For example, in various workplaces I have been warned by employee supervisors that three separate coworkers that I would be working with were "paranoid", "obsessive compulsive" and "borderline". I did not see any characteristics that the amateur diagnosticians warned me about and in all three cases, I found these co workers to be excellent and had absolutely no problems working with them. This is probably an extension of Dr. Frankfurt's work - the unconscious aspects of bullshitting but I expect that it correlates closely with some descriptions in a classic paper on prevarication.
But in the case of talking without expertise, I am afraid that the unconscious aspects cover a very small part of the bullshitting spectrum. You can go to any site where psychiatry is routinely criticized, attacked or vilified and you will see any number of posts by the anonymous posters who talk about their anecdotes and proclamations about psychiatry. Many are bombastic. None are challenged. It is the general tenor of many of these sites that psychiatrists are basically incompetent assholes (yeah I said it) and should be barred from practicing medicine. Psychiatrists only injure people and have never helped anyone. If they produce any coherent arguments they generally fit the psychiatrist as bogeyman dynamic that I previously described. Some people who have seen a psychiatrist may grudgingly admit it, but nobody ever seems to acknowledge that a psychiatrist did anything to help them. The more erudite approach may be to critique psychiatry without acknowledging that psychiatrists in fact are better critics and have critiqued their own field. If anyone is questioned they may produce the indignant response: "Are you calling me an antipsychiatrist?"
Some of what passes for criticism actually ignores what really happened and attempts to cast modern psychiatry in a light that is based more on historical spin than what is applicable today. Some of these efforts are actually considered to be "good" criticism, even though it is clear to any trained psychiatrist that the author knows little to nothing about the field. You would think that anyone interested in developing a negative narrative about psychiatry would do the basic research of picking up a copy of Shorter's A History of Psychiatry and reading about the ways things were before there was any psychiatry. In his text Shorter describes severe mental illness as a death sentence (p. 2) and the following historical observation: "In a world without psychiatry, rather than being tolerated or indulged, the mentally ill were treated with a savage lack of feeling. Before the advent of the therapeutic asylum, there was no golden era, no idyllic refuge for those deviant from the values of capitalism. To maintain otherwise is a fantasy." (p. 4). But the ignorance of psychiatry extends far beyond the historical. It is apparent that many of the critics have no knowledge of the current current psychiatric literature. They often reference the New York Times as though it is authoritative. They criticize highly technical subjects and it is apparent that they have not read a journal or a book from that field. Like Frankfurt's definition they pay no attention to the truth.
Based on Professor Frankfurt's essay, I conclude that bullshit is a much more appropriate characterization of many of the misrepresentations of psychiatry. I would also suggest it may be more politically correct than implying that the author is a member of a cult or a school of philosophy. (see the footnote at this link)
They are quite simply a bullshitter and bullshit remains as it always has been (even pre-Frankfurt) - bullshit.
George Dawson, MD, DFAPA
Harry G. Frankfurt. On Bullshit. Princeton University Press, Princeton, NJ, 2005.
Monday, January 27, 2014
WIll Integrity Save Psychiatry?
The answer is - it depends on how it is applied.
In the last two days, I have seen the integrity argument pulled out. Allen Frances is still using his bully pulpit on the Huffington Post, where it seems that anything critical of psychiatry is readily posted. In this case, he used the text of a blogger and the timeline created by this blogger to illustrate how there was no disclosure of a conflict of interest by a group of researchers, one of whom was the chair of the DSM-5 Task Force. The APA investigated this and acknowledged the non-disclosure of the conflict of interest. Apparently the acknowledgement in the form of an apology from the research group and the investigation by the APA is not enough for these critics. The blogger Dr. Nardo suggests that an "outside panel" be appointed to review his findings and the original materials again. I cannot think of how an "outside panel" could be convened. I have never really seen an objective analysis by an outside panel and wonder who might be selected. And yes I am suggesting that any outside panel would naturally have a significant conflict of interest. There appear to be many critics of psychiatry and only weak defenders.
He refers to a post by an anonymous web professional Neuroskeptic who summarized the state of things in his post as there being "no smoking gun." He also concludes that the idea of a psychiatric critics benefiting from book sales with the same theme suggests "by which logic, every author in history has had a financial conflict of interest in their own ideas." As a student of conflict of interest that IS a logical conclusion, especially when I see links to two of Dr. Frances' books listed right below the Huffington Post article. It is also an obvious fact that people routinely deny that applies to all human endeavors. If I am heavily invested in any subject my "ideas" can be counted upon to be fairly subjective and consistent with my self interest whether that is academic or financial. That is why I have read thousands of articles in Science, Nature, and medical journals in the past three decades and very few have panned out. At a larger level it is why Ioannides could declare that most published research is false. It is why you can count on seeing significant side effects from practically every medication approved by the FDA as safe and effective. So yes, I am afraid that same standard applies to the critics as well as the people doing the heavy lifting and trying to prove something in the first place. I would even take it a step further and suggest that the same transparency rules should be applied. How much money can you make as a critic of psychiatry or the DSM? My guess is plenty.
Both Dr. Frances and Dr. Nardo seem to be suggesting that all of the conflict of interest issues of academic psychiatrists and the way the APA handles them is sending psychiatry to hell in a handbasket. This is a historically incorrect view of the dismantling of psychiatry in the United States. Every day people in this country are getting inadequate psychiatric care. It has nothing to do with the ethical behavior of academic psychiatrists. It has a lot to do with the fact that the APA is not a very politically savvy organization and there are massive conflicts of interest interfering with the delivery of psychiatric care. Here are a few scenarios:
1. A depressed or psychotic but nonfunctional person is discharged from the emergency department because of a lack of "acute dangerousness" criteria. The family is outraged but they are told: "Look there is nothing we can do because he/she is not imminently dangerous to themselves. Upon further investigation the state has a "gravely disabled" criterion in the commitment statutes but it is practically never used. They find that local hospitals and courts never use that criteria because the patients admitted are too difficult to treat and place.
2. A person with acute alcohol and benzodiazepine withdrawal is sent home from the ER with a bottle of lorazepam and advised how to detoxify themselves. They go home and take the entire bottle to get high.
3. A person with alcoholism and depression is admitted for suicidal behavior. She was intoxicated, depressed and staring at a handgun. The next day the attending physician is contacted by a psychiatrist/utilization reviewer from the insurance company who has concluded the patient is no longer suicidal and they can be discharged. He will no longer authorize payment for inpatient treatment.
4. A pharmacy benefit manager refused to refill a 2 week prescription by a patient's psychiatrist. They have the pharmacist faxes a form to the psychiatrists office saying that they will only accept a 3 month prescription. The psychiatrist takes time to explain first to the pharmacists and then 2 different people at the PBM (total time 30 minutes) the rationale for not giving a large supply of medication to a chronically suicidal patient. The PBM refuses to change their position.
5. A managed care company refuses to cover psychotherapy provided by a psychiatrist. The psychiatrist explains that he is an expert in this type of therapy and the patient has been referred to him by the patient's primary psychiatrist. The managed care company authorizes 3 "crisis sessions".
6. A person completes a PHQ-9 scale in their primary care clinic and they score an 18. They see their primary care physician and say they would like to see a therapist. They are told to take an antidepressant and to come back in two weeks to fill out another PHQ-9. Total time of the visit is 5 minutes.
7. A person is seen in their primary care clinic and in 20 minutes is told by their nonpsychiatric physician that they have bipolar disorder. They are prescribed quetiapine, citalopram, and divalproex. Within several days they are too sedated to function at work.
The are just a few examples of thousands of people everyday who are receiving grossly inadequate care based on a specific ethical principle of physician behavior. That is the physician makes an assessment and prescribes care in what he or she believes is the best interest of the patient. That is the contract. There is no insurance company or government bureaucrat involved. There is no restricted access to mental health care or pretending that primary care physicians are psychiatrists. There is no remote "assessment" by a physician employed by a managed care company that prioritizes the financial well being of that insurance company or pharmacy benefit manager over the patient. In fact, I do not understand how that is ethical behavior at all.
That is the basis of the decline of psychiatry in this country. It has taken a proportionately larger hit than any other specialty. It is documented in detail on this blog and in E. Fuller Torrey's recent book. The adventures or misadventures of academic psychiatrists are relevant only insofar as the APA seems to use the President of the APA as a position that academics cycle in and out of. The idea that "psychiatrists in the trenches" are poorly represented by such a system is accurate with two possible exceptions that I can think of. Psychiatrists in the trenches are also poorly represented by criticism of academic psychiatrists and their conflict of interest agreements and personal employment contracts. It does nothing to address the central problems of the specialty, provides no tools that front line psychiatrist can use against all of the real conflicts of interest they face on a day by day basis, and is generally demoralizing. Before any critics suggest that I am supporting a "whitewash" - put yourself in the position of a psychiatrist who has just put in a 12 hour day taking care of 20 inpatients and putting up with passive aggressive and aggressive MCO and PBM reviewers who have been wasting your time and interfering with your care. You go home to read the paper and suddenly there is a major story of how unethical psychiatrists are - based on the appearance of conflict of interest. You try to remember that last time you saw a CME event that was sponsored by a pharmaceutical company. Then you check your files to make sure you have enough CME credits for relicensure. As an added piece of information that same psychiatrist doesn't really care about Section 3 in the DSM-5 or the issue of dimensional versus categorical diagnoses. They have not blinked an eye with the release of DSM-5 and won't in the future.
That is how the psychiatrist in the trenches experiences this academic exercise in conflict of interest. I say if you want to pull out an ethical argument and use that to help front line psychiatrists, it needs to be focused on the obvious targets in managed care and the government bureaucracies that support them.
You know - the real forces dismantling psychiatry (very effectively I might add) over the past three decades.
George Dawson, MD, DFAPA
In the last two days, I have seen the integrity argument pulled out. Allen Frances is still using his bully pulpit on the Huffington Post, where it seems that anything critical of psychiatry is readily posted. In this case, he used the text of a blogger and the timeline created by this blogger to illustrate how there was no disclosure of a conflict of interest by a group of researchers, one of whom was the chair of the DSM-5 Task Force. The APA investigated this and acknowledged the non-disclosure of the conflict of interest. Apparently the acknowledgement in the form of an apology from the research group and the investigation by the APA is not enough for these critics. The blogger Dr. Nardo suggests that an "outside panel" be appointed to review his findings and the original materials again. I cannot think of how an "outside panel" could be convened. I have never really seen an objective analysis by an outside panel and wonder who might be selected. And yes I am suggesting that any outside panel would naturally have a significant conflict of interest. There appear to be many critics of psychiatry and only weak defenders.
He refers to a post by an anonymous web professional Neuroskeptic who summarized the state of things in his post as there being "no smoking gun." He also concludes that the idea of a psychiatric critics benefiting from book sales with the same theme suggests "by which logic, every author in history has had a financial conflict of interest in their own ideas." As a student of conflict of interest that IS a logical conclusion, especially when I see links to two of Dr. Frances' books listed right below the Huffington Post article. It is also an obvious fact that people routinely deny that applies to all human endeavors. If I am heavily invested in any subject my "ideas" can be counted upon to be fairly subjective and consistent with my self interest whether that is academic or financial. That is why I have read thousands of articles in Science, Nature, and medical journals in the past three decades and very few have panned out. At a larger level it is why Ioannides could declare that most published research is false. It is why you can count on seeing significant side effects from practically every medication approved by the FDA as safe and effective. So yes, I am afraid that same standard applies to the critics as well as the people doing the heavy lifting and trying to prove something in the first place. I would even take it a step further and suggest that the same transparency rules should be applied. How much money can you make as a critic of psychiatry or the DSM? My guess is plenty.
Both Dr. Frances and Dr. Nardo seem to be suggesting that all of the conflict of interest issues of academic psychiatrists and the way the APA handles them is sending psychiatry to hell in a handbasket. This is a historically incorrect view of the dismantling of psychiatry in the United States. Every day people in this country are getting inadequate psychiatric care. It has nothing to do with the ethical behavior of academic psychiatrists. It has a lot to do with the fact that the APA is not a very politically savvy organization and there are massive conflicts of interest interfering with the delivery of psychiatric care. Here are a few scenarios:
1. A depressed or psychotic but nonfunctional person is discharged from the emergency department because of a lack of "acute dangerousness" criteria. The family is outraged but they are told: "Look there is nothing we can do because he/she is not imminently dangerous to themselves. Upon further investigation the state has a "gravely disabled" criterion in the commitment statutes but it is practically never used. They find that local hospitals and courts never use that criteria because the patients admitted are too difficult to treat and place.
2. A person with acute alcohol and benzodiazepine withdrawal is sent home from the ER with a bottle of lorazepam and advised how to detoxify themselves. They go home and take the entire bottle to get high.
3. A person with alcoholism and depression is admitted for suicidal behavior. She was intoxicated, depressed and staring at a handgun. The next day the attending physician is contacted by a psychiatrist/utilization reviewer from the insurance company who has concluded the patient is no longer suicidal and they can be discharged. He will no longer authorize payment for inpatient treatment.
4. A pharmacy benefit manager refused to refill a 2 week prescription by a patient's psychiatrist. They have the pharmacist faxes a form to the psychiatrists office saying that they will only accept a 3 month prescription. The psychiatrist takes time to explain first to the pharmacists and then 2 different people at the PBM (total time 30 minutes) the rationale for not giving a large supply of medication to a chronically suicidal patient. The PBM refuses to change their position.
5. A managed care company refuses to cover psychotherapy provided by a psychiatrist. The psychiatrist explains that he is an expert in this type of therapy and the patient has been referred to him by the patient's primary psychiatrist. The managed care company authorizes 3 "crisis sessions".
6. A person completes a PHQ-9 scale in their primary care clinic and they score an 18. They see their primary care physician and say they would like to see a therapist. They are told to take an antidepressant and to come back in two weeks to fill out another PHQ-9. Total time of the visit is 5 minutes.
7. A person is seen in their primary care clinic and in 20 minutes is told by their nonpsychiatric physician that they have bipolar disorder. They are prescribed quetiapine, citalopram, and divalproex. Within several days they are too sedated to function at work.
The are just a few examples of thousands of people everyday who are receiving grossly inadequate care based on a specific ethical principle of physician behavior. That is the physician makes an assessment and prescribes care in what he or she believes is the best interest of the patient. That is the contract. There is no insurance company or government bureaucrat involved. There is no restricted access to mental health care or pretending that primary care physicians are psychiatrists. There is no remote "assessment" by a physician employed by a managed care company that prioritizes the financial well being of that insurance company or pharmacy benefit manager over the patient. In fact, I do not understand how that is ethical behavior at all.
That is the basis of the decline of psychiatry in this country. It has taken a proportionately larger hit than any other specialty. It is documented in detail on this blog and in E. Fuller Torrey's recent book. The adventures or misadventures of academic psychiatrists are relevant only insofar as the APA seems to use the President of the APA as a position that academics cycle in and out of. The idea that "psychiatrists in the trenches" are poorly represented by such a system is accurate with two possible exceptions that I can think of. Psychiatrists in the trenches are also poorly represented by criticism of academic psychiatrists and their conflict of interest agreements and personal employment contracts. It does nothing to address the central problems of the specialty, provides no tools that front line psychiatrist can use against all of the real conflicts of interest they face on a day by day basis, and is generally demoralizing. Before any critics suggest that I am supporting a "whitewash" - put yourself in the position of a psychiatrist who has just put in a 12 hour day taking care of 20 inpatients and putting up with passive aggressive and aggressive MCO and PBM reviewers who have been wasting your time and interfering with your care. You go home to read the paper and suddenly there is a major story of how unethical psychiatrists are - based on the appearance of conflict of interest. You try to remember that last time you saw a CME event that was sponsored by a pharmaceutical company. Then you check your files to make sure you have enough CME credits for relicensure. As an added piece of information that same psychiatrist doesn't really care about Section 3 in the DSM-5 or the issue of dimensional versus categorical diagnoses. They have not blinked an eye with the release of DSM-5 and won't in the future.
That is how the psychiatrist in the trenches experiences this academic exercise in conflict of interest. I say if you want to pull out an ethical argument and use that to help front line psychiatrists, it needs to be focused on the obvious targets in managed care and the government bureaucracies that support them.
You know - the real forces dismantling psychiatry (very effectively I might add) over the past three decades.
George Dawson, MD, DFAPA
Sunday, January 26, 2014
Why Has Suboxone Turned Into A Problem?
The short answer is that it is like very other drug and there was always the potential for a problem. Any practicing physician realizes that when a drug is approved by the FDA for general release to the public there are all kinds of unintended consequences that are possible. That is the basis of post marketing surveillance by the FDA. There is invariably a lot of hype associated with the release of a drug, but as I have previously pointed out the FDAs approval process is not in place to guarantee a drug that is safe for everyone. It is focused on a releasing a drug that is a potential tool for responsible practitioners. That means any drug can potentially cause a small number of serious unexpected reactions (liver failure, cardiac arrhythmia) that even the most experienced practitioners will not be able to predict. There is also an implicit understanding that the practitioners prescribing the drug have a thorough understanding of its pharmacology, indications and contraindications. Many practitioners advise against trying out a product that has just been released but that advice is tempered by the severity of individual circumstances and the hope of relief and also the general bias that new drugs are somehow better than the old ones. That bias has been repeatedly disproven.
Suboxone prescribers have to take a special course in order to get a prescriber number in addition to their usual DEA number. I took the Suboxone prescriber course about 7 years ago. It was a total of 8 hours of lectures given in a convention center room in a hotel. It was jointly sponsored by state medical association. The morning sessions were largely a review of the pharmacology of the drug and the scope of the opioid addiction problem at the time. The afternoon session focused on vignettes of patients with addictions of varying complexities and the exercise was to determine of Suboxone should be prescribed to that person and how the induction would be done. That was the first suggestion that something was problematic. There apparently were no contraindications to Suboxone. The clear message was that it should be given to anyone with an opioid addiction no matter what their social circumstances or comorbid psychiatric diagnoses and addictions. There was a definite implication that this was a drug that would revolutionize the treatment of opioid addiction.
Suboxone is a combination of buprenorphine and naloxone. Buprenorphine is the active ingredient in terms of treating addiction. In this post I will use Suboxone and buprenorphine interchangeably. The pharmacological properties of buprenorphine that were interesting in terms of potential use for addiction included the fact that it was a opioid mu receptor partial agonist and antagonist at the kappa receptor. The partial agonist effects relevant for addiction such as euphoria and sedation occur at the lower doses and the antagonist effects occur at higher doses. The antagonist effects like preventing respiratory depression were thought to put a ceiling effect on this side effects and make it safer than pure mu receptor agonists that would produce dose related toxicities. In the Suboxone course the mixed agonist/antagonist effects were described as producing less toxicity and less risk of abuse. The naloxone component of Suboxone is a pure mu receptor antagonist. In the course I took, the explanation for the combination of buprenorphine and naloxone was that it reduced the risk of intravenous drug use and that this had occurred in Europe and it resulted in several deaths. The company also sold Subutex which was buprenorphine only and indicated for use in pregnant women.
The pharmacodynamics and pharmacokinetics in real life can differ quite a bit from the idealized cases that the initial marketing and advertising was based upon. Like many medications it can be a life changing drug. People can recover and break the cycle of addiction, recovery and relapse and go on to productive lives. It is the outliers that physicians need to be most concerned about. In real life there are always going to be people who get significant side effects even at low doses and cannot tolerate the drug. There are also people who tolerate the drug at high doses and do not experience the ceiling effect of mu receptor antagonism. The people are probably very low in number but they are significant because they are not protected by the ceiling effect that is supposed to be there from the drug. Drug addiction always attracts or produces a significant number of people who become amateur pharmacologists and use the drug to facilitate their addiction. The word gets out and suddenly buprenorphine has street value (about $1,000 for a 1 month prescription) and opioid addicts can use it when they run out of heroin or oxycodone. In a few people it is their preferred opioid because it has a longer half life.
The politics of Suboxone are as complicated as you will find in the pharmaceutical industry. There are plenty of conflicts of interest in terms of how the drug was initially marketed and plenty of crossover between regulators and the company who developed, marketed and sold it - Reckitt-Benckiser. According to a New York Times article last fall, the company was granted a period of exclusive sales that ended in 2009. After that they went on the offensive to suggest that their new product - a Suboxone film was superior to the generic tablets especially in the area of child safety. They stopped selling the Suboxone tablets at that point. Insurance companies can work any controversy to their advantage and people on buprenorphine maintenance have been cut off based solely on the amount of time they have been taking the drug. There are no scientific guidelines for how long a person should take buprenorphine and like most drugs used for maintenance therapy there will never be a study that looks at that question due to the expense. Most experts would agree that if you have a severe addiction and have recovered based on buprenorphine there is no reason why you would be cut off. In fact discontinuing buprenorphine seems to present a more significant problem as dose is tapered to 2 mg and lower. We also have a familiar political theme in the issue of opioids with the government seeming to create the problems in the first place and now saying: "Trust us we have the solution." That may have explained the desperation in the descriptions of how public health officials were trying to increase Suboxone prescribers to address a public health opioid epidemic that was a likely result of government initiatives to improve the treatment of pain.
Suboxone has become a problem for the same reason that every other drug becomes a problem - unrealistic expectations, conflicts of interest, and a knowledge deficit on the part of the practitioners. The title of the New York Times article illustrates how the press can look at the dual nature of drugs and imply that there is a larger problem. I don't know of two many drugs that do not have a "Dark Side". The negative trends in buprenorphine use can be reversed but it will take more than the suggested strategy in the NY Times article. Here are a few ideas:
1. The CDC needs to get involved and look at Suboxone/buprenorphine related deaths and study it in the same manner that they studied methadone. It would be very instructive to see exactly where Suboxone/buprenorphine falls on the spectrum of deaths/100 kg MME (milligram morphine equivalents). The expectation of some in the article is that it is much safer, I would prefer to see the numbers. Only the CDC has access to the detailed data to look at this issue. I would take it a step farther and suggest that the CDC recalculate this table on an annual basis as a key metric in reversing the significant public health problem of accidental opioid overdose deaths.
2. The physicians prescribing the buprenorphine need to be highly motivated and well versed in prescribing medications to individuals with addictions. The NY Times article suggests that there are many who take an entrepreneurial approach to the prescription of buprenorphine with cash only practices that vary from $100 - $250 a visit. I have no problem with cash only practices if there is a quality approach. By definition that involves a lot more than handing someone a prescription in 5 minutes. The problem is the rest of what happens during that time is poorly defined. The original prescribing information said that the physician needed to refer the patient to counseling services. In many presentations of research that I have seen there is a clear movement to illustrate that - counseling adds little to nothing to outcomes when buprenorphine is prescribed. There are problems drawing that conclusion about this research given the modest outcomes of the buprenorphine treatment.
3. At least part of the interview of any patient recovering from the severe addiction that occurs with opioids is assessing their functional capacity. What are they doing on a day to day basis and is that routine consistent with both recovery and a lack of cognitive side effects from the buprenorphine? Being able to corroborate that improvement with a third party makes it even more reliable.
4. A big part of the unconscious aspects of addiction is the behaviors that are present to continue the addiction despite the best conscious efforts of the person affected. Good examples include craving, lying, and hiding use from others. That requires prescribing physicians to engage their patients at this level and not develop a law enforcement transference. A lot of physicians don't know how to respond to an accusation of: "You don't trust me!" when there is a question of the need for a toxicology screen or a discussion of a positive toxicology. The interpersonal aspect of treatment is very important and it received no attention in the standard Suboxone prescribing course.
5. Continued work on a model of treatment looking at all of the potential positive factors is needed. There is nothing worse in medicine than to treat a scientific topic like a political one and not have a rational approach to the person with the problem. Like the original course I took, there are people out there who say that buprenorphine prescribed out of a physicians office is all that is needed. Is that the case when you have a person who takes two to three times the prescribed amount to get high? Or the person who is crushing it and snorting or injecting it? Or the person who is selling it on the street to get purchase heroin? Or the person who can't function due to cognitive problems at 2 mg a day? Or the person who is hospitalized for recurrent bowel obstructions due to severe constipation? As the prescribing physician - are you confident that you can accurately screen for these problems? What about competing approaches like the long acting mu antagonist naltrexone injections? Where does 12-step recovery like Narcotics Anonymous fit in? Where do sober housing and residential treatment fit in? And finally - where can a person get detoxified and should anyone be forced to go through acute opioid withdrawal when they are incarcerated?
All of these questions are currently unanswered. But like most treatments in medicine, the solution is typically a lot more than a pill. Drugs with addictive potential always add the complication of significant financial gain from a captive audience.
George Dawson, MD, DFAPA
Deborah Sontag. Addiction Treatment With A Dark Side. New York Times. November 16, 2013.
SAMHSA. Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. A Treatment Improvement Protocol. TIP 40.
NICE. Naltrexone for the management of opioid dependence. 2010.
NICE. Methadone and buprenorphine for the management of opioid dependence. 2010.
Suboxone prescribers have to take a special course in order to get a prescriber number in addition to their usual DEA number. I took the Suboxone prescriber course about 7 years ago. It was a total of 8 hours of lectures given in a convention center room in a hotel. It was jointly sponsored by state medical association. The morning sessions were largely a review of the pharmacology of the drug and the scope of the opioid addiction problem at the time. The afternoon session focused on vignettes of patients with addictions of varying complexities and the exercise was to determine of Suboxone should be prescribed to that person and how the induction would be done. That was the first suggestion that something was problematic. There apparently were no contraindications to Suboxone. The clear message was that it should be given to anyone with an opioid addiction no matter what their social circumstances or comorbid psychiatric diagnoses and addictions. There was a definite implication that this was a drug that would revolutionize the treatment of opioid addiction.

Suboxone is a combination of buprenorphine and naloxone. Buprenorphine is the active ingredient in terms of treating addiction. In this post I will use Suboxone and buprenorphine interchangeably. The pharmacological properties of buprenorphine that were interesting in terms of potential use for addiction included the fact that it was a opioid mu receptor partial agonist and antagonist at the kappa receptor. The partial agonist effects relevant for addiction such as euphoria and sedation occur at the lower doses and the antagonist effects occur at higher doses. The antagonist effects like preventing respiratory depression were thought to put a ceiling effect on this side effects and make it safer than pure mu receptor agonists that would produce dose related toxicities. In the Suboxone course the mixed agonist/antagonist effects were described as producing less toxicity and less risk of abuse. The naloxone component of Suboxone is a pure mu receptor antagonist. In the course I took, the explanation for the combination of buprenorphine and naloxone was that it reduced the risk of intravenous drug use and that this had occurred in Europe and it resulted in several deaths. The company also sold Subutex which was buprenorphine only and indicated for use in pregnant women.
The pharmacodynamics and pharmacokinetics in real life can differ quite a bit from the idealized cases that the initial marketing and advertising was based upon. Like many medications it can be a life changing drug. People can recover and break the cycle of addiction, recovery and relapse and go on to productive lives. It is the outliers that physicians need to be most concerned about. In real life there are always going to be people who get significant side effects even at low doses and cannot tolerate the drug. There are also people who tolerate the drug at high doses and do not experience the ceiling effect of mu receptor antagonism. The people are probably very low in number but they are significant because they are not protected by the ceiling effect that is supposed to be there from the drug. Drug addiction always attracts or produces a significant number of people who become amateur pharmacologists and use the drug to facilitate their addiction. The word gets out and suddenly buprenorphine has street value (about $1,000 for a 1 month prescription) and opioid addicts can use it when they run out of heroin or oxycodone. In a few people it is their preferred opioid because it has a longer half life.
The politics of Suboxone are as complicated as you will find in the pharmaceutical industry. There are plenty of conflicts of interest in terms of how the drug was initially marketed and plenty of crossover between regulators and the company who developed, marketed and sold it - Reckitt-Benckiser. According to a New York Times article last fall, the company was granted a period of exclusive sales that ended in 2009. After that they went on the offensive to suggest that their new product - a Suboxone film was superior to the generic tablets especially in the area of child safety. They stopped selling the Suboxone tablets at that point. Insurance companies can work any controversy to their advantage and people on buprenorphine maintenance have been cut off based solely on the amount of time they have been taking the drug. There are no scientific guidelines for how long a person should take buprenorphine and like most drugs used for maintenance therapy there will never be a study that looks at that question due to the expense. Most experts would agree that if you have a severe addiction and have recovered based on buprenorphine there is no reason why you would be cut off. In fact discontinuing buprenorphine seems to present a more significant problem as dose is tapered to 2 mg and lower. We also have a familiar political theme in the issue of opioids with the government seeming to create the problems in the first place and now saying: "Trust us we have the solution." That may have explained the desperation in the descriptions of how public health officials were trying to increase Suboxone prescribers to address a public health opioid epidemic that was a likely result of government initiatives to improve the treatment of pain.
Suboxone has become a problem for the same reason that every other drug becomes a problem - unrealistic expectations, conflicts of interest, and a knowledge deficit on the part of the practitioners. The title of the New York Times article illustrates how the press can look at the dual nature of drugs and imply that there is a larger problem. I don't know of two many drugs that do not have a "Dark Side". The negative trends in buprenorphine use can be reversed but it will take more than the suggested strategy in the NY Times article. Here are a few ideas:
1. The CDC needs to get involved and look at Suboxone/buprenorphine related deaths and study it in the same manner that they studied methadone. It would be very instructive to see exactly where Suboxone/buprenorphine falls on the spectrum of deaths/100 kg MME (milligram morphine equivalents). The expectation of some in the article is that it is much safer, I would prefer to see the numbers. Only the CDC has access to the detailed data to look at this issue. I would take it a step farther and suggest that the CDC recalculate this table on an annual basis as a key metric in reversing the significant public health problem of accidental opioid overdose deaths.
2. The physicians prescribing the buprenorphine need to be highly motivated and well versed in prescribing medications to individuals with addictions. The NY Times article suggests that there are many who take an entrepreneurial approach to the prescription of buprenorphine with cash only practices that vary from $100 - $250 a visit. I have no problem with cash only practices if there is a quality approach. By definition that involves a lot more than handing someone a prescription in 5 minutes. The problem is the rest of what happens during that time is poorly defined. The original prescribing information said that the physician needed to refer the patient to counseling services. In many presentations of research that I have seen there is a clear movement to illustrate that - counseling adds little to nothing to outcomes when buprenorphine is prescribed. There are problems drawing that conclusion about this research given the modest outcomes of the buprenorphine treatment.
3. At least part of the interview of any patient recovering from the severe addiction that occurs with opioids is assessing their functional capacity. What are they doing on a day to day basis and is that routine consistent with both recovery and a lack of cognitive side effects from the buprenorphine? Being able to corroborate that improvement with a third party makes it even more reliable.
4. A big part of the unconscious aspects of addiction is the behaviors that are present to continue the addiction despite the best conscious efforts of the person affected. Good examples include craving, lying, and hiding use from others. That requires prescribing physicians to engage their patients at this level and not develop a law enforcement transference. A lot of physicians don't know how to respond to an accusation of: "You don't trust me!" when there is a question of the need for a toxicology screen or a discussion of a positive toxicology. The interpersonal aspect of treatment is very important and it received no attention in the standard Suboxone prescribing course.
5. Continued work on a model of treatment looking at all of the potential positive factors is needed. There is nothing worse in medicine than to treat a scientific topic like a political one and not have a rational approach to the person with the problem. Like the original course I took, there are people out there who say that buprenorphine prescribed out of a physicians office is all that is needed. Is that the case when you have a person who takes two to three times the prescribed amount to get high? Or the person who is crushing it and snorting or injecting it? Or the person who is selling it on the street to get purchase heroin? Or the person who can't function due to cognitive problems at 2 mg a day? Or the person who is hospitalized for recurrent bowel obstructions due to severe constipation? As the prescribing physician - are you confident that you can accurately screen for these problems? What about competing approaches like the long acting mu antagonist naltrexone injections? Where does 12-step recovery like Narcotics Anonymous fit in? Where do sober housing and residential treatment fit in? And finally - where can a person get detoxified and should anyone be forced to go through acute opioid withdrawal when they are incarcerated?
All of these questions are currently unanswered. But like most treatments in medicine, the solution is typically a lot more than a pill. Drugs with addictive potential always add the complication of significant financial gain from a captive audience.
George Dawson, MD, DFAPA
Deborah Sontag. Addiction Treatment With A Dark Side. New York Times. November 16, 2013.
SAMHSA. Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction. A Treatment Improvement Protocol. TIP 40.
NICE. Naltrexone for the management of opioid dependence. 2010.
NICE. Methadone and buprenorphine for the management of opioid dependence. 2010.
Wednesday, January 22, 2014
Snorting Smarties
"Throughout the history of the United States, popular attitudes and legal responses regarding the consumption of mood-altering substances have oscillated from tolerance to disapproval and back again in cycles roughly the length of a lifetime." David F. Musto, MD; Drugs in America, 2002 (p 3)
I heard about this story on my way in to work this morning. Middle school kids crushing a particular brand of candy and snorting it. I prefer the term insufflation but that is probably a bit too stodgy for a talk radio venue. I will let any readers who are interested in it Google it and look for relevant links and significant complications. Before we go any farther I will say that I am unequivocally against snorting anything. I am commenting on it here as an observation of two cultural phenomena - children's behavior mimicking adults and possibly predisposing them to the adult behavior and the cultural phenomenon of permissive versus prohibitive use of intoxicants.
I had an immediate association to a Psycritic blogpost that I responded to last night on whether marijuana legalization puts children and adolescents at risk. Having lived through the era of an 18 year old drinking age, I would say that it definitely does. The idea that you will now "tax and control" a newly legal intoxicant is a myth that only a politician or marijuana advocate would believe. My high school class of predominantly 17 year olds was one of the first locked up in an all night graduation party in order to prevent drinking and driving deaths. I don't imagine that anyone will be any more successful in keeping marijuana out of the hands of underage marijuana smokers than they were in keeping alcohol out of the hands of underage drinkers.
I found this behavior interesting because I observed a similar pattern of behavior among some of my classmates as early as the sixth grade. People were smoking various materials that were not meant to be smoked. They were ingesting materials that they believed would make them high, even when it was pharmacologically impossible. Even before that I remember candy cigarettes. They were in packs that resembled the real thing. My father was a two pack a day smoker of high tar and high nicotine cigarettes and I had asthma so smoking even at a dress rehearsal level never interested me. Candy cigarettes were frequently bought for children when I was growing up and everyone seemed to enjoy watching kids pretend to smoke.
It raises a larger question about addictive behaviors and whether modelling and rehearsing them can lead to practicing with the real thing. A related question would be whether a society that is permissive about a particular drug would be more likely to support behaviors that mimic using the actual drug. In the addiction field it is common to encounter these behaviors using both addictive and non-addictive compounds. For example, many people in the first stages of stimulant, sedative, or opioid addiction will start by crushing prescription tablets and smoking, snorting, or injecting them. Using a prescription in this manner is typically not a good sign in terms of controlled use of a potentially addictive medication because all of these methods of use are designed to deliver high levels of drug to the brain in a shorter period of time. That will often produce a temporary high after tolerance occurs to the oral form of the medication. In some settings, non-addicting medications like antihistamines, antidepressants, and others will be smoked, injected, or snorted. This can occur in correctional settings or situations where people may be trying to block out their conscious state and choose to produce a delirium consistent with that goal. It can get to the point where medications in general are banned from a certain setting because there is a black market for them right in the prison even though they have no value out side of the prison setting.
Getting back to the mimicking of addictive behavior and whether it may predispose you to using the compound at risk it was investigated for smoking. The authors of the study take a look at incomplete and indirect evidence and conclude that there is some evidence that candy cigarettes were possibly used as a marketing device by cigarette manufacturers. In one survey 5.3% of adult smokers attributed their smoking to a past use of candy cigarettes. I want to be clear that I am using the current trend of snorting candy as an example of mimicking addictive behavior with a substance that is meant to be eaten as candy.
I don't consider myself a crusader for one law versus another. I have beaten my head against the wall on numerous political issues in the past and know that there are many hidden forces in this country that you can bet have much more leverage than I do either as a private citizen or a member of a medical professional organization. There is one thing that you can count on in America and that is money will carry the day. Politicians believing that there will be new tax revenue from the sales of an intoxicant is very reinforcing for them. Their friends in the business world creating a monopoly product that people will line up to buy is another. Don't forget that in 1884 Heroin was the brand name of an over-the-counter patent medication that was originally marketed by a pharmaceutical company. At about the same time a competitor was selling 15 different brands of cocaine for smoking, injecting, and sniffing. All of them were available over the counter without a prescription. The restriction on that practice did not occur until the Harrison Act in 1914.
The coming rush to see who sells marijuana in this country will be an interesting one. The outcome should be as predictable as the previous oscillations toward tolerance in this country.
George Dawson, MD, DFAPA
Klein JD, Forehand B, Oliveri J, Patterson CJ, Kupersmidt JB, Strecher V. Candy cigarettes: do they encourage children's smoking? Pediatrics. 1992 Jan;89(1):27-31. PubMed PMID: 1728016.
Klein JD, Clair SS. Do candy cigarettes encourage young people to smoke? BMJ.2000 Aug 5;321(7257):362-5. Review. PubMed PMID: 10926600; PubMed Central PMCID: PMC1118335.
I heard about this story on my way in to work this morning. Middle school kids crushing a particular brand of candy and snorting it. I prefer the term insufflation but that is probably a bit too stodgy for a talk radio venue. I will let any readers who are interested in it Google it and look for relevant links and significant complications. Before we go any farther I will say that I am unequivocally against snorting anything. I am commenting on it here as an observation of two cultural phenomena - children's behavior mimicking adults and possibly predisposing them to the adult behavior and the cultural phenomenon of permissive versus prohibitive use of intoxicants.
I had an immediate association to a Psycritic blogpost that I responded to last night on whether marijuana legalization puts children and adolescents at risk. Having lived through the era of an 18 year old drinking age, I would say that it definitely does. The idea that you will now "tax and control" a newly legal intoxicant is a myth that only a politician or marijuana advocate would believe. My high school class of predominantly 17 year olds was one of the first locked up in an all night graduation party in order to prevent drinking and driving deaths. I don't imagine that anyone will be any more successful in keeping marijuana out of the hands of underage marijuana smokers than they were in keeping alcohol out of the hands of underage drinkers.
I found this behavior interesting because I observed a similar pattern of behavior among some of my classmates as early as the sixth grade. People were smoking various materials that were not meant to be smoked. They were ingesting materials that they believed would make them high, even when it was pharmacologically impossible. Even before that I remember candy cigarettes. They were in packs that resembled the real thing. My father was a two pack a day smoker of high tar and high nicotine cigarettes and I had asthma so smoking even at a dress rehearsal level never interested me. Candy cigarettes were frequently bought for children when I was growing up and everyone seemed to enjoy watching kids pretend to smoke.
It raises a larger question about addictive behaviors and whether modelling and rehearsing them can lead to practicing with the real thing. A related question would be whether a society that is permissive about a particular drug would be more likely to support behaviors that mimic using the actual drug. In the addiction field it is common to encounter these behaviors using both addictive and non-addictive compounds. For example, many people in the first stages of stimulant, sedative, or opioid addiction will start by crushing prescription tablets and smoking, snorting, or injecting them. Using a prescription in this manner is typically not a good sign in terms of controlled use of a potentially addictive medication because all of these methods of use are designed to deliver high levels of drug to the brain in a shorter period of time. That will often produce a temporary high after tolerance occurs to the oral form of the medication. In some settings, non-addicting medications like antihistamines, antidepressants, and others will be smoked, injected, or snorted. This can occur in correctional settings or situations where people may be trying to block out their conscious state and choose to produce a delirium consistent with that goal. It can get to the point where medications in general are banned from a certain setting because there is a black market for them right in the prison even though they have no value out side of the prison setting.
Getting back to the mimicking of addictive behavior and whether it may predispose you to using the compound at risk it was investigated for smoking. The authors of the study take a look at incomplete and indirect evidence and conclude that there is some evidence that candy cigarettes were possibly used as a marketing device by cigarette manufacturers. In one survey 5.3% of adult smokers attributed their smoking to a past use of candy cigarettes. I want to be clear that I am using the current trend of snorting candy as an example of mimicking addictive behavior with a substance that is meant to be eaten as candy.
I don't consider myself a crusader for one law versus another. I have beaten my head against the wall on numerous political issues in the past and know that there are many hidden forces in this country that you can bet have much more leverage than I do either as a private citizen or a member of a medical professional organization. There is one thing that you can count on in America and that is money will carry the day. Politicians believing that there will be new tax revenue from the sales of an intoxicant is very reinforcing for them. Their friends in the business world creating a monopoly product that people will line up to buy is another. Don't forget that in 1884 Heroin was the brand name of an over-the-counter patent medication that was originally marketed by a pharmaceutical company. At about the same time a competitor was selling 15 different brands of cocaine for smoking, injecting, and sniffing. All of them were available over the counter without a prescription. The restriction on that practice did not occur until the Harrison Act in 1914.
The coming rush to see who sells marijuana in this country will be an interesting one. The outcome should be as predictable as the previous oscillations toward tolerance in this country.
George Dawson, MD, DFAPA
Klein JD, Forehand B, Oliveri J, Patterson CJ, Kupersmidt JB, Strecher V. Candy cigarettes: do they encourage children's smoking? Pediatrics. 1992 Jan;89(1):27-31. PubMed PMID: 1728016.
Klein JD, Clair SS. Do candy cigarettes encourage young people to smoke? BMJ.2000 Aug 5;321(7257):362-5. Review. PubMed PMID: 10926600; PubMed Central PMCID: PMC1118335.
Sunday, January 19, 2014
The Great Unconscious - Why REMS Are Bound To Fail
REMS is an acronym for Risk Evaluation and Mitigation Strategy. It is an FDA initiative to deal with the risks associated with certain medications. I first encountered this new concept because one of my lectures is on the current opioid epidemic and looking at the potential risks of opioids. The FDA has an REMS section on their web site including a list of all currently approved REMS. For the purpose of this post I am going to focus on the REMS for Extended Release and Long Acting Opioids. The actual document is 42 pages long. I read it twice and really cannot see anything in the document that would detect the major problems with opioids or potentially prevent those problems. It suggests a thorough evaluation of the type than many primary care physicians no longer have the time to do. The basic elements of a complete history and physical exam, pain diagnosis and examination for addiction and psychiatric comorbidity needs to be taken in the context that substantial numbers of patients with psychiatric diagnoses are now diagnosed by a symptom checklist that is checked off in about 2 minutes. If there is any take home message from this REMs it should be that chronic pain requiring opioid therapy should be referred to a specialty center where they have the time and staff to do the required assessment.
The biggest misconception here seems to be that patients are accurate reporters and they have no unconscious agenda. It leads me to question whether the FDA employs any psychiatrists. It also highlights a naive approach to medicine that suggests physicians and patients are automatons who are basically reading and completing checklists. The complete checklist suggests the diagnosis. On what planet does this happen? With regard to the population of patients with an addiction seeking treatment of chronic pain with opioids, the following graphic may apply.
 The data represented in the above diagram are from the National Survey on Drug Use and Health. The sample size is 70,000 persons, but the conclusions in the diagram are all drawn from the survey and have the usual limitations. What the diagram shows is that most people who believe they need treatment for an addiction do not make an effort to get it. The NSDUH looks at detailed information across a number of treatment settings and reasons for not accessing treatment.
The data represented in the above diagram are from the National Survey on Drug Use and Health. The sample size is 70,000 persons, but the conclusions in the diagram are all drawn from the survey and have the usual limitations. What the diagram shows is that most people who believe they need treatment for an addiction do not make an effort to get it. The NSDUH looks at detailed information across a number of treatment settings and reasons for not accessing treatment.
I use the above diagram when I am taking with primary care physicians or residents about the situation where they are trying to determine whether or not it is safe to prescribed opioids for chronic pain. I point out that the people they are seeing in their office probably resemble the sample participants from the NSDUH. How would those evaluations of themselves affect their response to questions about addiction during their assessment? By the time people see me and they have an entirely different frame of reference. They may have had one (or several) near death experiences from overdosing on opioids. They may have become homeless and lost the support of their friends and family. They may have encountered a number of situations making the drug use problem very difficult to deny. The people receiving the REMS evaluation from their physicians will almost always be similar to the NSDUH sample. The implication is that these folks won't be "honest" with their physician, but the problem is much more than an honesty problem. Anyone with an addiction has lost their capacity to fully recognize the nature and severity of the problem. Their responses are based on a number of biased decision-making processes that continue the addiction. The primary care physician is in the impossible position of needing to be a lie detector with a person who may not feel like they are lying. It is another operation of the great unconscious but in this case one that is unrecognizably biased by addiction.
The response to opioids is the first clue that there may be a problem. People disposed to addiction have a striking response to opioids. The described an intense euphorigenic effect. In contrast to the usual ideas that opioids are sedating many will feel much more energetic and productive. A distinct feeling that a hoped for potential has finally been realized with the expected boost in confidence is often a third feature that is extremely reinforcing. These are generally the opioid response features that place a person at high risk for opioid addiction.
The unconscious aspects of drug addiction are described in a number of ways. Sellman describes it as compulsive drug seeking being initiated outside of consciousness. Koob talks about the process going from an initial process of an impulse control disorder involving positive reinforcement to compulsive activity that is driven by the negative reinforcement of avoiding withdrawal phenomena. Most people are not conscious of that process unless it it reviewed with them in detail. Another unconscious aspect of addiction is cravings. Cravings can vary from a spontaneous intense urge to use a drug to an urge associated with sensory phenomena that occurs after exposure to a drug cue like seeing people use the drug on television. Whether the craving is cue-induced or spontaneous they represent a drug induced change in a person's conscious state that can be present long after there has been exposure to a drug.
A risk management strategy to identify problems with opioid prescriptions needs to incorporate a strategy that takes these features into account. Information about limiting access to prescription opioids and destroying unused opioids is certainly a useful public health strategy but it does nothing for a person who has a strongly reinforcing reaction to the drug. At the minimum there needs to be education that the response to the drug is a key feature to identify addiction risk. Patients need to be educated about that as well as addictive behaviors and those anchor points need to be revisited at every physician visit where response to pain, addictive behavior, psychiatric comorbidity and functional capacity needs to be assessed. These are also the areas where the bulk of physician education needs to occur. There is also the issue of whether teaching primary care physicians is the best strategy to limit opioid overprescription. It may ultimately be the best strategy because the lessons learned could be applied to the overprescription of many drugs with similar dynamics like antibiotics, benzodiazepines, and stimulants. There is also the model of specialty referral to reduce the burden on primary care clinic. This model was popular in many states prior to the more widespread practice of prescribing opioids for chronic noncancer pain and it is the basis of the guideline for treating chronic neuropathic pain by the National Institute for Health and Care Excellence (NICE).
George Dawson, MD, DFAPA
The biggest misconception here seems to be that patients are accurate reporters and they have no unconscious agenda. It leads me to question whether the FDA employs any psychiatrists. It also highlights a naive approach to medicine that suggests physicians and patients are automatons who are basically reading and completing checklists. The complete checklist suggests the diagnosis. On what planet does this happen? With regard to the population of patients with an addiction seeking treatment of chronic pain with opioids, the following graphic may apply.

I use the above diagram when I am taking with primary care physicians or residents about the situation where they are trying to determine whether or not it is safe to prescribed opioids for chronic pain. I point out that the people they are seeing in their office probably resemble the sample participants from the NSDUH. How would those evaluations of themselves affect their response to questions about addiction during their assessment? By the time people see me and they have an entirely different frame of reference. They may have had one (or several) near death experiences from overdosing on opioids. They may have become homeless and lost the support of their friends and family. They may have encountered a number of situations making the drug use problem very difficult to deny. The people receiving the REMS evaluation from their physicians will almost always be similar to the NSDUH sample. The implication is that these folks won't be "honest" with their physician, but the problem is much more than an honesty problem. Anyone with an addiction has lost their capacity to fully recognize the nature and severity of the problem. Their responses are based on a number of biased decision-making processes that continue the addiction. The primary care physician is in the impossible position of needing to be a lie detector with a person who may not feel like they are lying. It is another operation of the great unconscious but in this case one that is unrecognizably biased by addiction.
The response to opioids is the first clue that there may be a problem. People disposed to addiction have a striking response to opioids. The described an intense euphorigenic effect. In contrast to the usual ideas that opioids are sedating many will feel much more energetic and productive. A distinct feeling that a hoped for potential has finally been realized with the expected boost in confidence is often a third feature that is extremely reinforcing. These are generally the opioid response features that place a person at high risk for opioid addiction.
The unconscious aspects of drug addiction are described in a number of ways. Sellman describes it as compulsive drug seeking being initiated outside of consciousness. Koob talks about the process going from an initial process of an impulse control disorder involving positive reinforcement to compulsive activity that is driven by the negative reinforcement of avoiding withdrawal phenomena. Most people are not conscious of that process unless it it reviewed with them in detail. Another unconscious aspect of addiction is cravings. Cravings can vary from a spontaneous intense urge to use a drug to an urge associated with sensory phenomena that occurs after exposure to a drug cue like seeing people use the drug on television. Whether the craving is cue-induced or spontaneous they represent a drug induced change in a person's conscious state that can be present long after there has been exposure to a drug.
A risk management strategy to identify problems with opioid prescriptions needs to incorporate a strategy that takes these features into account. Information about limiting access to prescription opioids and destroying unused opioids is certainly a useful public health strategy but it does nothing for a person who has a strongly reinforcing reaction to the drug. At the minimum there needs to be education that the response to the drug is a key feature to identify addiction risk. Patients need to be educated about that as well as addictive behaviors and those anchor points need to be revisited at every physician visit where response to pain, addictive behavior, psychiatric comorbidity and functional capacity needs to be assessed. These are also the areas where the bulk of physician education needs to occur. There is also the issue of whether teaching primary care physicians is the best strategy to limit opioid overprescription. It may ultimately be the best strategy because the lessons learned could be applied to the overprescription of many drugs with similar dynamics like antibiotics, benzodiazepines, and stimulants. There is also the model of specialty referral to reduce the burden on primary care clinic. This model was popular in many states prior to the more widespread practice of prescribing opioids for chronic noncancer pain and it is the basis of the guideline for treating chronic neuropathic pain by the National Institute for Health and Care Excellence (NICE).
George Dawson, MD, DFAPA
Saturday, January 18, 2014
The Drive To Do Good Work When No One Is Looking
Himmelstein and Woolhandler have hit it out of the park again. This time in a seemingly modest letter to the editor in the weeks JAMA. Although their main point was the perversity of pay-for-performance incentives in the final paragraph they make this observation:
"We fear that pay-for-performance incentives will undermine the mindset required for good physician practice (ie, the drive to do good work even when no one is looking)." (p.304)
This is a quote that everyone should pay attention to because the so-called financial incentives that have been with us for years are highly problematic and have not contributed a thing to the quality of medical practice. The first consideration is whether or not what Himmelstein and Woolhandler say is true? It has clear validity. Physicians are trained to do the right thing in terms of individual patient care. That involves dedication and adhering to professional standards like continuity of care. Physicians as a group are driven people. They will work past the point of exhaustion especially f they feel that they need to follow up a certain problem for a certain patient. Many primary care physicians are working 24/7 in order to keep up on paperwork, labs, prescriptions, and test results. It is not possible to "call it a night" if there is a critical lab value that needs to be evaluated or a patient that needs to be informed. There are plenty of decisions in medicine that have a high inherent degree of uncertainty and that can lead to sleepless nights searching for an answer. The electronic health record (EHR) has increased that burden. I have colleagues that tell me that every morning when they walk into clinic they may have as many as 200 lab results waiting for them in the EHR. If they do not have assistance with triage, they have to personally view these results and do something about them. They may also have to respond to direct e-mails if they are affiliated with a plan that allows patients to directly e-mail their physician. That is before they begin seeing a full schedule of patients and seeing urgent problems that day. Responsibility to the patient is what drives this process not trivial financial rewards and penalties based on illogical outcome measures.
Why all of the confusion? I think the problem can be analyzed at several levels. At the antiphysician level there are obvious forces in play that want to coopt the professionalism of physicians and make it seem like without a business and government bureaucracy that physicians would be out of control. In other words the public needs the government and big business to control physicians. This was the essential rhetoric that led to the managed care era in the first place. Physicians were greedy, did too many procedures for financial gain, and needed to be managed by a large and expensive business administration. The managed care theory completely ignores two basic facts. The most obvious fact is that three decades of managed care has not controlled health care inflation or increased health care access as promised. That is compounded by the fact that many of these companies currently own all of the means of production including the doctors, hospitals, labs, and MRI scanners. But nobody has accused them of being greedy. The second fact is that independent review of the problem from the 1990s showed that the political theory that physicians were engaged in massive overutilization was so inaccurate that they closed the government review program down. How often does a government program get shut down?
The assault on the professionalism of physicians reached new heights in the 1990s when the federal government under the Clinton administration decided that fraud conducted by physicians was also a major driver of health care inflation. Armed with billing codes and guns, it was an era where FBI agents were trained to enter offices, get the records and determine of the documentation matched the billing code. There were several high profile cases where the Department of Justice decided that "fraud" had occurred. The fraud they were referring to in one of the landmark cases was attending physicians not writing an extensive enough note in addition to whatever note the resident physician wrote. That led to about two decades of excessive and unnecessary documentation. Right up until the point that the federal government could grant this power to managed care companies and give them the power to deny payment and demand reimbursement back based on their interpretation of whether the documentation supported the service provided.
Throughout all of this heavy handed political intervention physicians have continued to do the right thing and maintain their professionalism but the rhetoric has taken a heavy toll. It is not unusual for a person to enter a health facility owned by a managed care company and see some credos from the physician code of conduct plastered on the walls in an elevator. When that happens the company is generally sending a clear message: "It is only because of us that medical professionals behave in a professional manner." Nothing is farther from the truth. There is no carrot or stick that keeps a neurosurgery residents on call in a hospital every day and night for a year at a time. There is no carrot or stick that keeps psychiatrists treating aggressive patients who continually threaten and may try to assault them. There is no carrot or stick that keeps physicians going to the point of exhaustion and to the point that they realize that they are clearly spending much more time caring for other people than their own families. A typical response from people with those scenarios is either: "You don't have to do that." or "You don't have to work that hard." Physicians currently waste 20-30% of their time on bureaucratic nonsense dreamt up by people who themselves do not provide direct patient care. In the time left they are expected to see more patients and do more documentation than physicians have ever had to do at any point in history.
I don't mean to suggest that there are not people in all walks of life who do the right thing at work. As I am typing this I recall my father describing one of his coworkers sometime back in the 1960s. My father was a railroad engineer. He drove locomotives of both the diesel and steam variety. The railroad world in those days was a parallel universe that I would occasionally get a glimpse of. Massive buildings smelling of diesel fuel storing massive, loud, pulsating diesel locomotives. They just let them run 24 hours a day. My father and a group of his railroad colleagues were rebuilding the porch on our house one day and they were all talking very positively about a car knocker who worked for the same railroad. A car knocker is a rail car repairman. They keep trains rolling. All of my father's co workers and my father all praised this person because at work he always seemed to do the right thing. The quality that they seemed to admire the most was that he would always attend to part of the task even when he lacked a certain skill that required him to pass part of the job on. That was apparently a rare trait and that was my first observation of the quality of doing good work and how it was widely admired on its own merit. No financial reward or employee of the week parking spot. Just the mostly hidden admiration of your coworkers.
To me the most perverse aspect of physician "incentives" is that they are already earned by physicians. In the managed care world, groups of physicians are subjected to a "holdback" of anywhere from 5-15% of their gross billing. The idea is that unless the entire department makes the productivity expectation (an arbitrary number set by an administrator) the money is lost. If the financial target is made money "awarded" was already earned. There are no bonuses only penalties. A lot of the incentives for reporting various measurements or complying with the next bureaucratic hoop are in the 1-2% range. That is important only for the bean counters described in the letter. Make no mistake about it - they will exert whatever pressure they can on physicians to "make" that 1 or 2%. And make no mistake about it - twenty years that bean counter job would not have existed.
And there still would have been physicians in hospitals all night long trying to do the right thing and not caring who knows about it.
George Dawson, MD, DFAPA
Himmelstein DU, Woolhandler S. Physician payment incentives to improve care quality. JAMA. 2014 Jan 15;311(3):304. doi: 10.1001/jama.2013.284475. PubMed PMID: 24430325.
Additional Clinical Note 1: Some health care settings have really taken the incentive programs to an absurd level. Mandatory pep rallys for the employees, employee of the week or month awards and the expectation that everyone generates a huge amount of false enthusiasm for these rewards. At the same time the confidential 360 degree performance review is the latest tool that administrators can use against physicians. In this exercise a panel of anonymous multidisciplinary coworkers rate physicians on a number of non-medical standards (like how well they support corporate standards). The performance review is basically a combination of subjective impressions that have very little to do with the physicians medical competence. It is all part of the corporate beauty contest that is passed off as medical quality. Most managed care companies seem to not know the meaning of the word.
Additional Clinical Note 2: Governments and managed care companies are never at a loss for measuring things that are completely irrelevant to the provision of quality medical care. The best example is patient satisfaction surveys. If you are ever handed one as you leave the hospital or clinic the first question to ask yourself is whether the questions seem familiar. If they do it is because your were scripted. That means that the person you just talked with covered a number of bullet points corresponding to your survey. It is designed to maximize the score on that satisfaction survey. These results are often linked with incentives. But nobody ever talks about the fact that you could have received the best care in the world and may not been able to complete a survey when you left the hospital.
"We fear that pay-for-performance incentives will undermine the mindset required for good physician practice (ie, the drive to do good work even when no one is looking)." (p.304)
This is a quote that everyone should pay attention to because the so-called financial incentives that have been with us for years are highly problematic and have not contributed a thing to the quality of medical practice. The first consideration is whether or not what Himmelstein and Woolhandler say is true? It has clear validity. Physicians are trained to do the right thing in terms of individual patient care. That involves dedication and adhering to professional standards like continuity of care. Physicians as a group are driven people. They will work past the point of exhaustion especially f they feel that they need to follow up a certain problem for a certain patient. Many primary care physicians are working 24/7 in order to keep up on paperwork, labs, prescriptions, and test results. It is not possible to "call it a night" if there is a critical lab value that needs to be evaluated or a patient that needs to be informed. There are plenty of decisions in medicine that have a high inherent degree of uncertainty and that can lead to sleepless nights searching for an answer. The electronic health record (EHR) has increased that burden. I have colleagues that tell me that every morning when they walk into clinic they may have as many as 200 lab results waiting for them in the EHR. If they do not have assistance with triage, they have to personally view these results and do something about them. They may also have to respond to direct e-mails if they are affiliated with a plan that allows patients to directly e-mail their physician. That is before they begin seeing a full schedule of patients and seeing urgent problems that day. Responsibility to the patient is what drives this process not trivial financial rewards and penalties based on illogical outcome measures.
Why all of the confusion? I think the problem can be analyzed at several levels. At the antiphysician level there are obvious forces in play that want to coopt the professionalism of physicians and make it seem like without a business and government bureaucracy that physicians would be out of control. In other words the public needs the government and big business to control physicians. This was the essential rhetoric that led to the managed care era in the first place. Physicians were greedy, did too many procedures for financial gain, and needed to be managed by a large and expensive business administration. The managed care theory completely ignores two basic facts. The most obvious fact is that three decades of managed care has not controlled health care inflation or increased health care access as promised. That is compounded by the fact that many of these companies currently own all of the means of production including the doctors, hospitals, labs, and MRI scanners. But nobody has accused them of being greedy. The second fact is that independent review of the problem from the 1990s showed that the political theory that physicians were engaged in massive overutilization was so inaccurate that they closed the government review program down. How often does a government program get shut down?
The assault on the professionalism of physicians reached new heights in the 1990s when the federal government under the Clinton administration decided that fraud conducted by physicians was also a major driver of health care inflation. Armed with billing codes and guns, it was an era where FBI agents were trained to enter offices, get the records and determine of the documentation matched the billing code. There were several high profile cases where the Department of Justice decided that "fraud" had occurred. The fraud they were referring to in one of the landmark cases was attending physicians not writing an extensive enough note in addition to whatever note the resident physician wrote. That led to about two decades of excessive and unnecessary documentation. Right up until the point that the federal government could grant this power to managed care companies and give them the power to deny payment and demand reimbursement back based on their interpretation of whether the documentation supported the service provided.
Throughout all of this heavy handed political intervention physicians have continued to do the right thing and maintain their professionalism but the rhetoric has taken a heavy toll. It is not unusual for a person to enter a health facility owned by a managed care company and see some credos from the physician code of conduct plastered on the walls in an elevator. When that happens the company is generally sending a clear message: "It is only because of us that medical professionals behave in a professional manner." Nothing is farther from the truth. There is no carrot or stick that keeps a neurosurgery residents on call in a hospital every day and night for a year at a time. There is no carrot or stick that keeps psychiatrists treating aggressive patients who continually threaten and may try to assault them. There is no carrot or stick that keeps physicians going to the point of exhaustion and to the point that they realize that they are clearly spending much more time caring for other people than their own families. A typical response from people with those scenarios is either: "You don't have to do that." or "You don't have to work that hard." Physicians currently waste 20-30% of their time on bureaucratic nonsense dreamt up by people who themselves do not provide direct patient care. In the time left they are expected to see more patients and do more documentation than physicians have ever had to do at any point in history.
I don't mean to suggest that there are not people in all walks of life who do the right thing at work. As I am typing this I recall my father describing one of his coworkers sometime back in the 1960s. My father was a railroad engineer. He drove locomotives of both the diesel and steam variety. The railroad world in those days was a parallel universe that I would occasionally get a glimpse of. Massive buildings smelling of diesel fuel storing massive, loud, pulsating diesel locomotives. They just let them run 24 hours a day. My father and a group of his railroad colleagues were rebuilding the porch on our house one day and they were all talking very positively about a car knocker who worked for the same railroad. A car knocker is a rail car repairman. They keep trains rolling. All of my father's co workers and my father all praised this person because at work he always seemed to do the right thing. The quality that they seemed to admire the most was that he would always attend to part of the task even when he lacked a certain skill that required him to pass part of the job on. That was apparently a rare trait and that was my first observation of the quality of doing good work and how it was widely admired on its own merit. No financial reward or employee of the week parking spot. Just the mostly hidden admiration of your coworkers.
To me the most perverse aspect of physician "incentives" is that they are already earned by physicians. In the managed care world, groups of physicians are subjected to a "holdback" of anywhere from 5-15% of their gross billing. The idea is that unless the entire department makes the productivity expectation (an arbitrary number set by an administrator) the money is lost. If the financial target is made money "awarded" was already earned. There are no bonuses only penalties. A lot of the incentives for reporting various measurements or complying with the next bureaucratic hoop are in the 1-2% range. That is important only for the bean counters described in the letter. Make no mistake about it - they will exert whatever pressure they can on physicians to "make" that 1 or 2%. And make no mistake about it - twenty years that bean counter job would not have existed.
And there still would have been physicians in hospitals all night long trying to do the right thing and not caring who knows about it.
George Dawson, MD, DFAPA
Himmelstein DU, Woolhandler S. Physician payment incentives to improve care quality. JAMA. 2014 Jan 15;311(3):304. doi: 10.1001/jama.2013.284475. PubMed PMID: 24430325.
Additional Clinical Note 1: Some health care settings have really taken the incentive programs to an absurd level. Mandatory pep rallys for the employees, employee of the week or month awards and the expectation that everyone generates a huge amount of false enthusiasm for these rewards. At the same time the confidential 360 degree performance review is the latest tool that administrators can use against physicians. In this exercise a panel of anonymous multidisciplinary coworkers rate physicians on a number of non-medical standards (like how well they support corporate standards). The performance review is basically a combination of subjective impressions that have very little to do with the physicians medical competence. It is all part of the corporate beauty contest that is passed off as medical quality. Most managed care companies seem to not know the meaning of the word.
Additional Clinical Note 2: Governments and managed care companies are never at a loss for measuring things that are completely irrelevant to the provision of quality medical care. The best example is patient satisfaction surveys. If you are ever handed one as you leave the hospital or clinic the first question to ask yourself is whether the questions seem familiar. If they do it is because your were scripted. That means that the person you just talked with covered a number of bullet points corresponding to your survey. It is designed to maximize the score on that satisfaction survey. These results are often linked with incentives. But nobody ever talks about the fact that you could have received the best care in the world and may not been able to complete a survey when you left the hospital.
Thursday, January 16, 2014
A Better Way To Manage - Lessons From the Coach
I ran across a basic article on Phil Jackson the other day in the AARP newsletter. Like most people unfamiliar with his story I get the occasional stories about him that describe him as a guru. I can see the movie now with novices climbing to the top of some mountain in the Himalaya's only to find him seated in an wooden temple, speaking the basic truths about NBA coaching in a way that only he is capable of. He is a legendary basketball coach. The AARP newsletter was brief but it contained huge advice. In it we learn that he is the son of two clergy and spirituality naturally guides his decision making. When people think about spirituality they frequently equate that with religion and react to it on that basis. They miss the point that spirituality can be the essence of a person. It can be a connection with a process greater than one's self and have nothing to do with religion. One of my colleagues John MacDougall captures this well in his definition of spirituality as: "the quality or nature of our relationships in three dimensions - relationships with our Higher Power, with ourselves and with other people."
The other Phil Jackson observation from the article that impressed me was the notion that he used nonauthoritarian methods to empower his players and these methods came directly from a spiritual direction that allowed him to be true to himself. He talked about knowing that "things of a higher calling could unite groups of men."
Contrast that with typical managed care or business strategies that leave the people out of the equation. The best way to look at that contrast is by looking at some team situations I have been in the past. I wrote about my Renal Medicine team in the past. It was my last rotation in medical school and I walked off that service at about 8 PM on the last day before graduation. The whole raison d'etre of that team was the two goals of excellent medical care and education. The approach to both goals was intensive. Even as a medical student, I felt like a critical part of the team. My job was to go out into the large medical complex on the grounds of the Milwaukee County Medical Center and do consults. On the last day, the two residents I was working with approached me and said: "Look George, we know this is your big day but we are getting killed. Can you do these consults?" Of course I did. The only meaning that my action had at the time was the I was a part of this team and I wanted to share the workload. After we completed rounds that night at about 9 PM, those same residents joked about how I was a super medical student and some of the jokes were quite funny. But that rotation (with a few others) was one of the most meaningful educational experiences of my life. To this day, I miss working with that team. It was a spiritual experience!
Teams on inpatient psychiatric units can be a different story in part because they are influenced by the typical silo style management of big hospitals. The managers are ego rather than team driven. There are separate nursing and physician structures. Some of the team members may be in separate unions. There are multiple disciplines that can be split be numerous administrative hierarchies. It is always easy for administrators to try to play one discipline against the next. Institutional attitudes can affect psychiatric teams at multiple levels. At various times I have been in teams where one or more members were being influenced by administrators to the detriment of the team. That almost always translates to suboptimal patient care. The administrative message to teams can be fairly extreme. At one point I can recall being told that we were no longer doing team meetings. Productivity measured as individual physician-patient contacts was more important. At that time we had already been told that our documentation was supposed to include a blurb about observations made in the team meeting or it would not "meet criteria" for the correct billing code. At other times we were plagued by observers - bureaucrats, consultants, or business types who clearly did not know anything about the work or at least the work we were doing. Many were hired guns brought in by our own administration as the "next big idea" or an attempt to manipulate the team in some way. In the most extreme situation, a representative of the administration was sitting in team meetings and telling us what to do. I say extreme because the administrator had never assessed any of the patients and did not know them. They also did not have the expertise to make a diagnosis or treatment plan. All of their decisions were strictly financial. They needed us to carry them out to provide the legitimacy of having licensed professionals names in the charts, especially on the discharge orders.
All of those last scenarios are at the extreme other end of the spectrum from Phil Jackson's approach. My guess is that Phil Jackson would not have been able to keep Kobe Bryant in LA when he wanted to be traded with just financial incentives and a business approach. It took a spiritual one. He had to feel like he was part of a larger process. That is the spiritual atmosphere that needs to be created on treatment teams. You won't get to that by expecting physicians or nurses or social workers or occupational therapists to be mini-administrators focused on "cost effectiveness". In fact, it is exactly the wrong approach.
The correct spiritual ground for a team is unity, appropriate concern for other team members, common goals and positive affect associated with being on that team. Team members need to to have a uniform neutral and spiritual approach to the people they are trying to help. One of John MacDougall's suggested approach to improve spirituality is: "try treating every human being that you meet as if he or she were a beloved child of a Higher Power." It has nothing to do with being a bean counter and in fact if the bean counters can't support the development and maintenance of teams - it is time for everybody to walk away and start over.
Phil Jackson's elaboration of a non-authoritarian spiritual approach to managing people on teams is just another important way that the government and the managed care world miss the boat and end up providing the worst possible management of health care workers, especially mental health care workers. Micromanagement and a general cluelessness about managing knowledge workers is another. We don't have a shortage of worker productivity or a shortage of workers - we have grossly mismanaged workers and some of the worst managers in the world.
George Dawson, MD, DFAPA
John A. MacDougall. Being Sober and Becoming Happy. CreateSpace Independent Publishing Platform, 2013. p. 40.
Phil Jackson and Hugh Delehanty. Sacred Hoops. Spiritual Lessons of a Hardwood Warrior. Hyperion, New York, 1995.
The other Phil Jackson observation from the article that impressed me was the notion that he used nonauthoritarian methods to empower his players and these methods came directly from a spiritual direction that allowed him to be true to himself. He talked about knowing that "things of a higher calling could unite groups of men."
"I've learned that the most effective way to forge a winning team is to call on the players need to connect with something larger than themselves...... It requires the individuals involved to surrender their self interest for the greater good so that the whole adds up to more than the sum of its parts." - Phil Jackson in Sacred Hoops (p. 5)
Contrast that with typical managed care or business strategies that leave the people out of the equation. The best way to look at that contrast is by looking at some team situations I have been in the past. I wrote about my Renal Medicine team in the past. It was my last rotation in medical school and I walked off that service at about 8 PM on the last day before graduation. The whole raison d'etre of that team was the two goals of excellent medical care and education. The approach to both goals was intensive. Even as a medical student, I felt like a critical part of the team. My job was to go out into the large medical complex on the grounds of the Milwaukee County Medical Center and do consults. On the last day, the two residents I was working with approached me and said: "Look George, we know this is your big day but we are getting killed. Can you do these consults?" Of course I did. The only meaning that my action had at the time was the I was a part of this team and I wanted to share the workload. After we completed rounds that night at about 9 PM, those same residents joked about how I was a super medical student and some of the jokes were quite funny. But that rotation (with a few others) was one of the most meaningful educational experiences of my life. To this day, I miss working with that team. It was a spiritual experience!
Teams on inpatient psychiatric units can be a different story in part because they are influenced by the typical silo style management of big hospitals. The managers are ego rather than team driven. There are separate nursing and physician structures. Some of the team members may be in separate unions. There are multiple disciplines that can be split be numerous administrative hierarchies. It is always easy for administrators to try to play one discipline against the next. Institutional attitudes can affect psychiatric teams at multiple levels. At various times I have been in teams where one or more members were being influenced by administrators to the detriment of the team. That almost always translates to suboptimal patient care. The administrative message to teams can be fairly extreme. At one point I can recall being told that we were no longer doing team meetings. Productivity measured as individual physician-patient contacts was more important. At that time we had already been told that our documentation was supposed to include a blurb about observations made in the team meeting or it would not "meet criteria" for the correct billing code. At other times we were plagued by observers - bureaucrats, consultants, or business types who clearly did not know anything about the work or at least the work we were doing. Many were hired guns brought in by our own administration as the "next big idea" or an attempt to manipulate the team in some way. In the most extreme situation, a representative of the administration was sitting in team meetings and telling us what to do. I say extreme because the administrator had never assessed any of the patients and did not know them. They also did not have the expertise to make a diagnosis or treatment plan. All of their decisions were strictly financial. They needed us to carry them out to provide the legitimacy of having licensed professionals names in the charts, especially on the discharge orders.
All of those last scenarios are at the extreme other end of the spectrum from Phil Jackson's approach. My guess is that Phil Jackson would not have been able to keep Kobe Bryant in LA when he wanted to be traded with just financial incentives and a business approach. It took a spiritual one. He had to feel like he was part of a larger process. That is the spiritual atmosphere that needs to be created on treatment teams. You won't get to that by expecting physicians or nurses or social workers or occupational therapists to be mini-administrators focused on "cost effectiveness". In fact, it is exactly the wrong approach.
The correct spiritual ground for a team is unity, appropriate concern for other team members, common goals and positive affect associated with being on that team. Team members need to to have a uniform neutral and spiritual approach to the people they are trying to help. One of John MacDougall's suggested approach to improve spirituality is: "try treating every human being that you meet as if he or she were a beloved child of a Higher Power." It has nothing to do with being a bean counter and in fact if the bean counters can't support the development and maintenance of teams - it is time for everybody to walk away and start over.
Phil Jackson's elaboration of a non-authoritarian spiritual approach to managing people on teams is just another important way that the government and the managed care world miss the boat and end up providing the worst possible management of health care workers, especially mental health care workers. Micromanagement and a general cluelessness about managing knowledge workers is another. We don't have a shortage of worker productivity or a shortage of workers - we have grossly mismanaged workers and some of the worst managers in the world.
George Dawson, MD, DFAPA
John A. MacDougall. Being Sober and Becoming Happy. CreateSpace Independent Publishing Platform, 2013. p. 40.
Phil Jackson and Hugh Delehanty. Sacred Hoops. Spiritual Lessons of a Hardwood Warrior. Hyperion, New York, 1995.
Thursday, January 9, 2014
Latest Bad Ideas From the FDA - Zohydro and Adasuve
Like them or not the FDA is the critical agency in terms of pharmaceutical regulation and the politics of pharmaceuticals. It is easy to confuse the politics of drugs with pharmaceutical science. Clear examples include special interest groups lobbying the FDA and members of Congress for rapid access to medications that have not been approved for specific indications. Some of those medications have significant side effects and very low therapeutic efficacy. At the same time, the FDA is criticized for approving medications that add nothing to the existing pharmacopeia or that have marginal evidence for efficacy. If you view medications as tools that need to be applied in various on and off label ways by practicing physicians, that is by definition a lower threshold for regulatory approval than the standard that a medication must be very effective and very safe. It turns out that there are very few medications with that profile. Some problems and inconsistencies are more glaring than others.
I was surprised to get a recent warning letter from the FDA on an inhaled preparation of loxapine called Adasuve. Loxapine is an antipsychotic drug of medium potency. Back in the late 1980s we had a drug trial of loxapine versus haloperidol on one of the inpatient units I was running at the time. It was a fairly effective drug for acute symptoms of psychosis and was less potent than haloperidol so it has fewer neurological side effects. It never seemed like a very popular medication with psychiatrists. There was some recurrent interest around the issue of first and second generation antipsychotics with some authors suggesting that it had a receptor profile that was more similar to second generation or atypical antipsychotics. During the initial period when it was approved and marketed under the brand name Loxitane it was available in both oral and injectable forms.
I could only locate one study at PubMed on the Adasuve in the current medical literature searching on the brand name. There were 20 studies at clinicaltrials.gov web site but unfortunately no results were posted. Some of them appear to be very interesting including one that looks at the QTc interval effects of inhaled loxapine. A review of the Adasuve web site shows that bronchospasm is a black box warning and that there is a Risk Evaluation and Mitigation Strategy (REMS) to assess prior to prescribing and monitoring the patient after each administered dose. It looks like it can only be given in a registered health care facility by personnel who can assess and manage any pulmonary complications. Although the pulmonary conditions that contraindicate use seem fairly straightforward (asthma, COPD, any pulmonary diagnosis associated with bronchospasm) the actual diagnoses are probably more complex due to a number of factors including smoking status, body weight, and the complexity of the underlying pulmonary syndromes. Staff administering this medication should assess the patient for pulmonary problems at every episode and not depend on historical diagnoses.
From a philosophical standpoint, there needs to be an active debate about new patents or patent extensions on medications that are currently generic drugs like loxapine. During the time it was primarily used it certainly did not demonstrate any superior efficacy or side effect profile relative to other typical or atypical antipsychotics. Loxapine is metabolized to amoxapine, an FDA approved antidepressant that has been used on a limited basis in psychiatric practice and is generally not considered a first or second line antidepressant. The metabolic relationship led some authors to speculate that the combination may be effective in psychotic depression but that application was never realized. So in this case we have a drug with limited applications that has been repackaged in a riskier dosage form. That seems like several steps in the wrong direction. The details about the pharmacokinetics are available in the package insert. Looking at this data, the main advantage appears to be the short time is takes to reach maximum plasma concentration (1-2 minutes). A useful study here would have looked at a subgroup of patients taking parenteral loxapine and similar pharmacokinetic measures. In the study I alluded to from the 1980s loxapine was compared directly to haloperidol for acute agitation in schizophrenia or bipolar disorder.
With this medication released into practice, if I was still working on an acute inpatient unit I would be very skeptical of using this medication for acute agitation. Use is limited to a single dose in a 24 hour period. The people who need this medication are generally medically complex, may still have street drugs in their system, are generally cigarette smokers and their pulmonary and in many cases their cardiac status may be unknown. If the initial dose is not effective, the question becomes - now what? Patient preference may be an issue since some patients request a fast acting medication but they do not want parenteral injections. Patients with an addiction history may have used drugs by insufflation, inhalation, and intravenous injection and that may be a factor in their decision making. All other factors considered there have been studies of patient preference for specific medications to treat acute agitation and of the antipsychotic class of medications only olanzapine is highly rated. Besides the degree of acceptance, post marketing surveillance will be important in terms of medication side effects. The current approval was based on pooled data from three studies looking at a total of 259 patients getting the active medication and 263 patient receiving placebo. That is not many doses of this medication.
Zohydro probably requires less discussion. Zohydro is advertised as the only acetaminophen free, extended release form of hydrocodone available in the United States. It is available in dosage forms ranging from 10 mg to 50 mg intended as a twice-a-day dose schedule. Zohydro comes with the following black box warning:
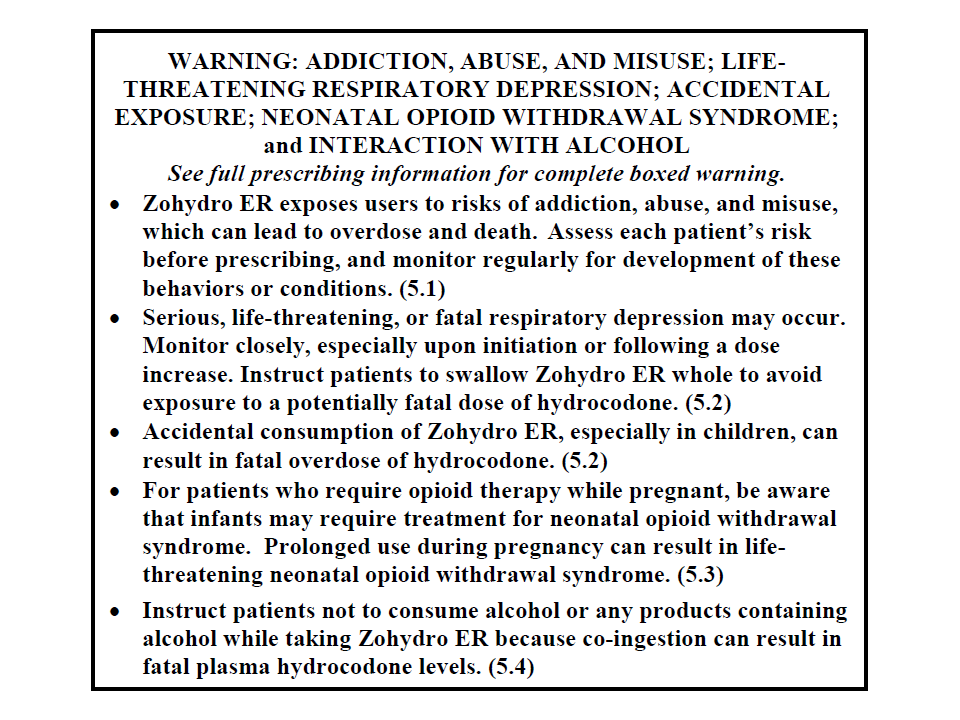
The interesting part of this approval process was that the scientific advisory panel, for the FDA voted overwhelmingly against approving this medication, but it was approved anyway. We are currently in the midst of an opioid epidemic based on a number of metrics including emergency department visits for complications, deaths from accidental overdose, per capita consumption of opioids relative to the rest of the world, and the increasing number of people addicted to opioids. We are also entering a period of increased policing of physicians by numerous agencies for opioid prescribing practices. There is fairly good evidence that the "opioid epidemic" started with a pain treatment initiative suggesting that physicians were not treating pain aggressively enough. The pendulum has swung to the point where there will be clear blame for at least some physicians who are using opioids to treat chronic pain.
There are a couple of additional problems with the FDA approved package insert for Zohydro. The first is the Indication or reason the FDA approved this drug in the first place. The indication for Zohydro is: ".....the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment for which alternative treatment options are inadequate." That is a shockingly inadequate description of a pain syndrome. In keeping with a medication as a tool model for regulatory approval this is acceptable. But any physician prescribing this medication should have a more specific pain diagnosis that specifically addresses the chronicity of the pain and why this might be an acceptable approach.
The second problem on my first read through of the package insert is the following graphic of the efficacy of this medication. It plots the results of an study of Zohydro versus placebo in 510 subjects who were already on chronic opioid therapy for chronic back pain.
![]()
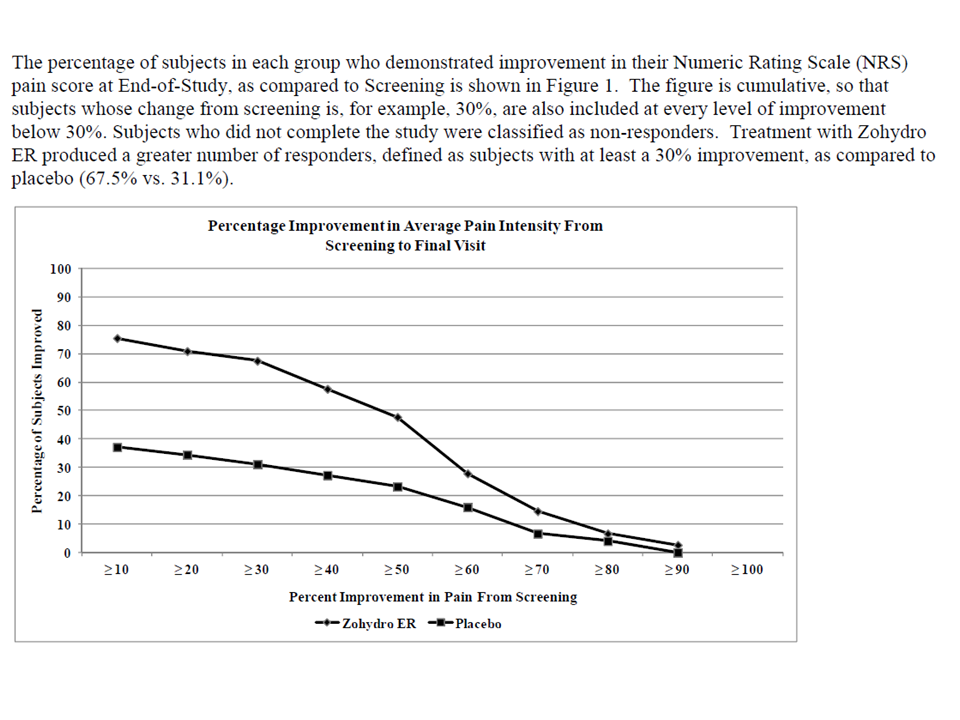 I think that these examples highlight the fact that the FDA does not seem to have any guiding philosophy when it comes to some new drug approvals of repackaged generics other a Darwinian free market approach. Since the original drug passed the safety and efficacy standards why wouldn't the repackaged generic? Physicians should demand a more specific regulatory approach. At the minimum there needs to be clearer evidence of an advance in pharmacotherapy in terms of increased efficacy or a better side effect profile. Repackaging generic drugs without that kind of guidance and obvious risks seems like a mistake to me. There also needs to be a better approach to chronic pain and drugs that are clearly addictive and a more uniform methodology for measuring efficacy. Most studies looking at opioid use in chronic pain show modest pain relief at best. In clinical practice, the relief is generally on the order of what is expected with non-opioids on population wide comparisons. There should be an easy way to operationalize that knowledge and instruct pharmaceutical manufacturers on the appropriate design of clinical trials to answer these questions. There is also the issue of conflict of interest and the need for complete disclosure of who is advocating for the use of the medications in question.
I think that these examples highlight the fact that the FDA does not seem to have any guiding philosophy when it comes to some new drug approvals of repackaged generics other a Darwinian free market approach. Since the original drug passed the safety and efficacy standards why wouldn't the repackaged generic? Physicians should demand a more specific regulatory approach. At the minimum there needs to be clearer evidence of an advance in pharmacotherapy in terms of increased efficacy or a better side effect profile. Repackaging generic drugs without that kind of guidance and obvious risks seems like a mistake to me. There also needs to be a better approach to chronic pain and drugs that are clearly addictive and a more uniform methodology for measuring efficacy. Most studies looking at opioid use in chronic pain show modest pain relief at best. In clinical practice, the relief is generally on the order of what is expected with non-opioids on population wide comparisons. There should be an easy way to operationalize that knowledge and instruct pharmaceutical manufacturers on the appropriate design of clinical trials to answer these questions. There is also the issue of conflict of interest and the need for complete disclosure of who is advocating for the use of the medications in question.
From an addiction standpoint, hydrocodone and acetaminophen compounds are some of the most frequently diverted and abused compounds. It is not uncommon to get a history of people taking amounts that are the equivalent of chronic overdoses with the acetaminophen component. Many if not most of the people with this addiction are aware of the risks of the acetaminophen component but when the chronic phase of the addiction develops they will continue to use it and ignore that danger. Patient preferences can be a factor in the decision to prescribe an opioid. Hydrocodone combination medications are in high demand on the street indicating to me that is is a preferred product to many addicts. The package insert contains remarkably little useful practical information on abuse, dependence, and addiction. We are told that there is a REMS strategy and that the FDA is requiring manufacturers of newly approved long acting opioids to conduct long term follow up studies to look at the "serious risks of long term use."
I think it would be a lot easier if FDA regulators just looked at the current data on the CDC web site about the addiction risk of opioids and answer the question: "Why would Zohydro be any different?"
George Dawson, MD, DFAPA
FDA. Adasuve Full Prescribing Information. (Click on appropriate link).
European Medicines Agency. Adasuve EPAR (European Public Assessment Report).
Additional Clinical Note 1: On 1/14/2014 the FDA issued a recommendation that health professionals stop using combination products that contain more than 325 mg acetaminophen. That same page has a link to a letter that will be sent to manufacturers that these dose strengths be withdrawn over the next three years. Based on their rationale (no increased efficacy with acetaminophen and risk for hepatotoxicity), I don't know why 325 mg acetaminophen is the magic number. The addiction experience with combination products suggest that people will routinely use potentially toxic doses as part of their addiction, even when they know that there is a potential problem with the amount of acetaminophen. This new rule may increase increase the amount of opioids prescribed.
I was surprised to get a recent warning letter from the FDA on an inhaled preparation of loxapine called Adasuve. Loxapine is an antipsychotic drug of medium potency. Back in the late 1980s we had a drug trial of loxapine versus haloperidol on one of the inpatient units I was running at the time. It was a fairly effective drug for acute symptoms of psychosis and was less potent than haloperidol so it has fewer neurological side effects. It never seemed like a very popular medication with psychiatrists. There was some recurrent interest around the issue of first and second generation antipsychotics with some authors suggesting that it had a receptor profile that was more similar to second generation or atypical antipsychotics. During the initial period when it was approved and marketed under the brand name Loxitane it was available in both oral and injectable forms.
I could only locate one study at PubMed on the Adasuve in the current medical literature searching on the brand name. There were 20 studies at clinicaltrials.gov web site but unfortunately no results were posted. Some of them appear to be very interesting including one that looks at the QTc interval effects of inhaled loxapine. A review of the Adasuve web site shows that bronchospasm is a black box warning and that there is a Risk Evaluation and Mitigation Strategy (REMS) to assess prior to prescribing and monitoring the patient after each administered dose. It looks like it can only be given in a registered health care facility by personnel who can assess and manage any pulmonary complications. Although the pulmonary conditions that contraindicate use seem fairly straightforward (asthma, COPD, any pulmonary diagnosis associated with bronchospasm) the actual diagnoses are probably more complex due to a number of factors including smoking status, body weight, and the complexity of the underlying pulmonary syndromes. Staff administering this medication should assess the patient for pulmonary problems at every episode and not depend on historical diagnoses.
From a philosophical standpoint, there needs to be an active debate about new patents or patent extensions on medications that are currently generic drugs like loxapine. During the time it was primarily used it certainly did not demonstrate any superior efficacy or side effect profile relative to other typical or atypical antipsychotics. Loxapine is metabolized to amoxapine, an FDA approved antidepressant that has been used on a limited basis in psychiatric practice and is generally not considered a first or second line antidepressant. The metabolic relationship led some authors to speculate that the combination may be effective in psychotic depression but that application was never realized. So in this case we have a drug with limited applications that has been repackaged in a riskier dosage form. That seems like several steps in the wrong direction. The details about the pharmacokinetics are available in the package insert. Looking at this data, the main advantage appears to be the short time is takes to reach maximum plasma concentration (1-2 minutes). A useful study here would have looked at a subgroup of patients taking parenteral loxapine and similar pharmacokinetic measures. In the study I alluded to from the 1980s loxapine was compared directly to haloperidol for acute agitation in schizophrenia or bipolar disorder.
With this medication released into practice, if I was still working on an acute inpatient unit I would be very skeptical of using this medication for acute agitation. Use is limited to a single dose in a 24 hour period. The people who need this medication are generally medically complex, may still have street drugs in their system, are generally cigarette smokers and their pulmonary and in many cases their cardiac status may be unknown. If the initial dose is not effective, the question becomes - now what? Patient preference may be an issue since some patients request a fast acting medication but they do not want parenteral injections. Patients with an addiction history may have used drugs by insufflation, inhalation, and intravenous injection and that may be a factor in their decision making. All other factors considered there have been studies of patient preference for specific medications to treat acute agitation and of the antipsychotic class of medications only olanzapine is highly rated. Besides the degree of acceptance, post marketing surveillance will be important in terms of medication side effects. The current approval was based on pooled data from three studies looking at a total of 259 patients getting the active medication and 263 patient receiving placebo. That is not many doses of this medication.
Zohydro probably requires less discussion. Zohydro is advertised as the only acetaminophen free, extended release form of hydrocodone available in the United States. It is available in dosage forms ranging from 10 mg to 50 mg intended as a twice-a-day dose schedule. Zohydro comes with the following black box warning:

The interesting part of this approval process was that the scientific advisory panel, for the FDA voted overwhelmingly against approving this medication, but it was approved anyway. We are currently in the midst of an opioid epidemic based on a number of metrics including emergency department visits for complications, deaths from accidental overdose, per capita consumption of opioids relative to the rest of the world, and the increasing number of people addicted to opioids. We are also entering a period of increased policing of physicians by numerous agencies for opioid prescribing practices. There is fairly good evidence that the "opioid epidemic" started with a pain treatment initiative suggesting that physicians were not treating pain aggressively enough. The pendulum has swung to the point where there will be clear blame for at least some physicians who are using opioids to treat chronic pain.
There are a couple of additional problems with the FDA approved package insert for Zohydro. The first is the Indication or reason the FDA approved this drug in the first place. The indication for Zohydro is: ".....the management of pain severe enough to require daily, around-the-clock, long-term opioid treatment for which alternative treatment options are inadequate." That is a shockingly inadequate description of a pain syndrome. In keeping with a medication as a tool model for regulatory approval this is acceptable. But any physician prescribing this medication should have a more specific pain diagnosis that specifically addresses the chronicity of the pain and why this might be an acceptable approach.
The second problem on my first read through of the package insert is the following graphic of the efficacy of this medication. It plots the results of an study of Zohydro versus placebo in 510 subjects who were already on chronic opioid therapy for chronic back pain.

From an addiction standpoint, hydrocodone and acetaminophen compounds are some of the most frequently diverted and abused compounds. It is not uncommon to get a history of people taking amounts that are the equivalent of chronic overdoses with the acetaminophen component. Many if not most of the people with this addiction are aware of the risks of the acetaminophen component but when the chronic phase of the addiction develops they will continue to use it and ignore that danger. Patient preferences can be a factor in the decision to prescribe an opioid. Hydrocodone combination medications are in high demand on the street indicating to me that is is a preferred product to many addicts. The package insert contains remarkably little useful practical information on abuse, dependence, and addiction. We are told that there is a REMS strategy and that the FDA is requiring manufacturers of newly approved long acting opioids to conduct long term follow up studies to look at the "serious risks of long term use."
I think it would be a lot easier if FDA regulators just looked at the current data on the CDC web site about the addiction risk of opioids and answer the question: "Why would Zohydro be any different?"
George Dawson, MD, DFAPA
FDA. Adasuve Full Prescribing Information. (Click on appropriate link).
European Medicines Agency. Adasuve EPAR (European Public Assessment Report).
Additional Clinical Note 1: On 1/14/2014 the FDA issued a recommendation that health professionals stop using combination products that contain more than 325 mg acetaminophen. That same page has a link to a letter that will be sent to manufacturers that these dose strengths be withdrawn over the next three years. Based on their rationale (no increased efficacy with acetaminophen and risk for hepatotoxicity), I don't know why 325 mg acetaminophen is the magic number. The addiction experience with combination products suggest that people will routinely use potentially toxic doses as part of their addiction, even when they know that there is a potential problem with the amount of acetaminophen. This new rule may increase increase the amount of opioids prescribed.
Monday, January 6, 2014
It Is Cold Outside
I was driving into work this AM. I drive a six year old Toyota Van. The thermometer on my rearview mirror hovered between - 20 and -21 Fahrenheit, but every bank I passed said -24. Before I left home this morning I added a layer of polyester, packed additional headgear, and wore my Sorel boots. This is serious weather even if you are born and raised here and you need to be prepared for the worst. Standing outside for even a few minutes without adequate cover can result in frostbite or worse. The Governor of Minnesota closed down all of the schools today to prevent frostbite injuries and so far there have been no arguments with that decision. The drive home at night was slightly warmer at -16 degrees. The sky was so clear it was like being in outer space. I had to stop for gas and the driver's side door froze open. I had to hold it shut for about 6 miles until it thawed to the point I could slam it.
Apart from the pragmatics of winter survival, the cold weather also triggers a lot of associative memories - starting with my Sorels. I got these boots originally in 1971 in order to do a Limnology experiment on Lake Superior.

A friend of mine helped me and we went out onto the ice for a about 5 hours and pumped about 200 gallons of lake water through a plankton net to look at the winter plankton population. It was about -5 degrees that day. A few years earlier he had a case of frostbite after walking about 10 blocks to school wearing nothing but a pea coat. Like a lot of people in the northern US and Canada, I have found that these boots absolutely protect your feet in subzero weather.
I lived in Duluth, Minnesota for a while and can recall trying to speedskate when it was -10 to -15 degrees. At that temperature, a skate blade cannot compress and liquefy the ice enough to support much glide so the skating motion and its mechanics are seriously disrupted. I was wearing two layers of polyester, a layer of Lycra, and a layer of fiber. Unlike Sorels - speedskates even with neoprene boot covers don't protect much against the cold. When I got home I had to lay on top of a radiator under a blanket for 30 minutes in order to warm up. The coldest I have ever been in the winter usually happens after falling through the ice. I can recall walking across a creek and just getting ready to step up onto the far bank when I fell through the ice up to my chest in icy water. The sensation that occurs when that happens is incredible. Your breathing stops for a while followed by rapid gasping as you struggle to get out of the water. That is followed by the desperate run home. In my case it was only about 7 blocks and by the time I got there my clothes were frozen solid. A friend of mine was skating on Lake Superior and fell through the ice catching himself only by his fingertips. He ran home about the same distance but he had been totally submerged.
My more recent memories are about how the cold has been a factor in my role as a psychiatrist. Most psychiatrists in the Midwest have first-hand experience with the complications of cold weather. We have seen people with frostbite injuries both on burn units and after they have been transferred. We know many of the people who are caught in the endless inpatient unit -> emergency department -> homeless cycle that seems like a permanent artifact of our managed care inpatient and county mental health systems. We have seen the human interest stories that tend to run in the papers when the potentially lethal cold weather hits and the temporary concern about whether or not there are enough shelter beds.
Weather this cold does not allow you to make a lot of mistakes. Sometimes all it takes is the idea that you can run out to the trash can without putting on a jacket and finding that you have locked yourself out of the house. People with memory problems and disorientation can wander off and get lost. People with drinking problems can pass out or just take too long to get home. All it takes is a decision that keeps you out in the subzero weather for minutes too long and you can be in serious trouble.
Potentially lethal cold weather is also an integral part of treatment decisions. You can't really watch people coming in to appointments wearing summer clothing in this weather without doing an assessment for cold weather safety. It becomes part of the discharge decision making. Exactly how stable is the person's housing and how likely are they to keep themselves safe? Can they walk 10 blocks from the hospital to their apartment wearing a sweat suit, basketball shoes, and no hat? Should they be discharged to the street, even if they want to be? Should they be discharged if a managed care reviewer says that they should be discharged? We are generally talking about people who have chronic problems with insight and judgment. What about people with suicidal ideation? What about the person with chronic drug problems who has a history of drug induced blackouts and waking up on park benches? What about the person with Alzheimer’s disease who does not have 24 hour supervision?
How do you make an unbiased decision in that context? I can say that you don’t. You don’t because as a psychiatrist you are aware of all of the adverse outcomes. The continuum of severe frostbite injuries to the hypothermic who could not be resuscitated to those who were found frozen to death. You don’t want to see that happen to anyone. You don’t care if somebody wants to call that paternalistic. You don’t really care if it costs a managed care company or (more likely) a hospital a few bucks. You have been there yourself and you know you cannot take any chances in subzero weather. It’s not about a fear of being sued, it’s about concern for a fellow human being.
There are implications for the imminent dangerousness standard that is commonly applied to involuntary holds. I have argued with enough county attorneys over the years to understand that the standard itself is purely subjective and arbitrary. No matter how it appears on paper you will hear ten different interpretations from 10 different county attorneys. There are a few states where a gravely disabled standard applies. That standard states that a person may have problematic judgment to the point that it potentially impacts their ability to secure adequate food, medical care, or housing. That standard probably generally applies in these situations, but if you happen to be in a state where there is no statute or the county courts ignore it for convenience or financial reasons it may not be available for use.
Those are the kinds of things I think about when it gets this cold. I do get the occasional lighthearted thoughts – making sure I recall the thermodynamic equations that show my car battery dependent on temperature and telling myself that I am going to call Columbia and ask them if they make some type of expedition wear that is warmer than my current Titanium coat. But mostly – I hope the most vulnerable among us get the help they need and nobody gets injured or killed. Hopefully someday people will think about the fact that some people have a hard time protecting themselves - irrespective of the air temperature.
George Dawson, MD, DFAPA
Andy Rathbun. Regions Hospital Sees "Record-Breaking" Number of Frostbite Cases. St. Paul Pioneer Press. January 6, 2013.
From the article:
"Most of the people that come in with severe frostbite are "in some way compromised," he said. A small number are physically or mentally disabled, but a majority are people who have consumed too much alcohol or were abusing drugs and didn't realize how cold it was outside, Edmonson said."
Subscribe to:
Posts (Atom)