I received an e-mail first thing this morning from a person who identified himself as Peter C. Gøtzsche, MD. It looked official, but if this was not sent by Dr. Gøtzsche, all he has to do is send me an e-mail and I will delete this post. For those unfamiliar with why he might be sending me e-mails he is the author of the "Psychiatry Gone Astray" post that I critiqued. The body of the message was straightforward and said:
" Incidentally, I found out that some one has written about you and the way you treated my paper about the 10 myths in psychiatry. See attached"
The attachment read: "Asshole of the Day - George Dawson, MD" The proud author of that post made this statement after a completely respectful response to him on this blog.
Anyone who has been around the Internet and knows about malicious code would have to be a fool to click on an abusive attachment like this and put their data and identity at risk. Although this is a very simple message it says a lot about the way people expect to treat psychiatrists and get away with it. Dr. Gøtzsche had sent me an earlier e-mail saying he had responded to my criticism of his criticism of psychiatry. At this point I have not read it for various reasons including the low volume of web traffic from the Healy web site, the fact that I have been physically ill and exhausted, and my focus on other areas such as the recent series I am attempting to post on the reality of dangerous drugs.
Implicit in the e-mail is that his original "paper" had been treated poorly. I put "paper" in quotes here because as far as I am concerned it is a blog post. Where I come from a paper is published in a referred, peer reviewed journal. It is certainly possible to get rhetorical criticism against psychiatry published in that format, but even then it would not be beyond criticism. I also disagree with any implication that his opinions were treated poorly. It is called arguing and as every scientist, philosopher, and rhetorician knows there are at least two sides to every story. Practically all of the psychiatry critics don't seem to understand that these arguments can be done without taking things personally and using emotional invective. What many people don't seem to grasp is that it is also part of the scientific method. Arguments, theories, speculation, conjectures, etc. all have to withstand scrutiny over time. Even though every top scientist and mathematician expects these challenges, apparently only the critics of psychiatry consider themselves to be above criticism.
There is an asymmetry to the position that psychiatrists should not object to being criticized no matter how irrational, unscientific, or personal the criticism is. The implicit contention here is that the blog post was "treated" poorly but what about the way psychiatrists are treated and their work with people who have conditions that are treated by nobody else? And as I pointed out in my original criticisms, why do none of these critics ever look at closely at their own fields and the huge problems that exist there?
These dynamics are why there is such a blizzard of unscientific and unreliable criticism of psychiatry on the Internet and in the popular press. This is what happens if you are a psychiatrist who dares to speak out against it and not get into the usual patterns of silence or taking the position that you are somehow better than your colleagues.
My message to these people, no matter who they are is quite simple. If I have not been deterred by 35 years of irrational and mean spirited criticism - name calling is certainly not going to stop me now.
So to all of the proud critics of psychiatry - flame away! But don't expect me to engage you in a "debate". Anyone with an ounce of self respect knows that is not what is going on here.
George Dawson, MD, DFAPA
Supplementary 1: The other important disclosure that I have relative to the critics is that I have no conflict of interest or appearance of conflict of interest. I have no book to sell. I am not invested in pharmaceutical or medical device makers apart from mutual funds where I have no control over the investment decisions. I have never been paid for my commentary or writing and don't see that ever happening. I am not a paid spokesman for any commercial or professional organization. This is a completely noncommercial blog with no advertising. If I post copyrighted material here I have to pay for those rights out of my own pocket. I have no relationships with any pharmaceutical companies. I do not consider myself to be a celebrity and I am therefore not trying to enhance my celebrity status and in fact will be he first to admit that hardly anybody reads this blog. This entire blog is written in my spare time and yes I have a day job. I encourage a similar analysis of any critic of psychiatry you might be listening to.
Showing posts with label antipsychiatry rhetoric. Show all posts
Showing posts with label antipsychiatry rhetoric. Show all posts
Thursday, February 20, 2014
Friday, February 14, 2014
Heat Map of Psychiatric Criticism
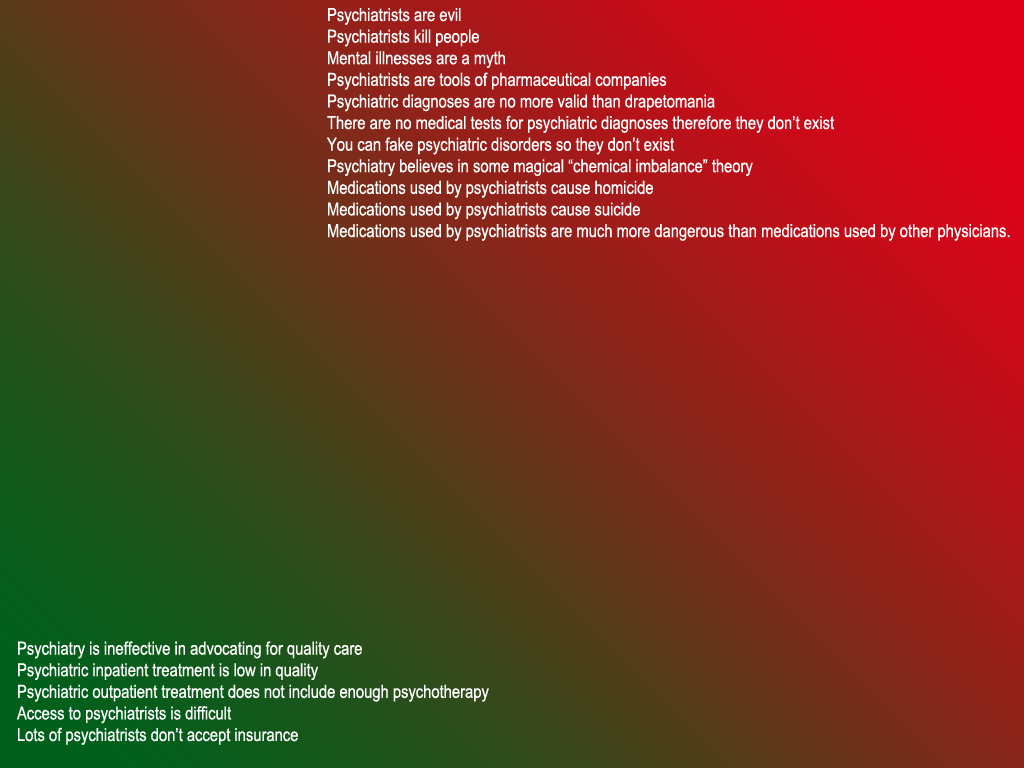
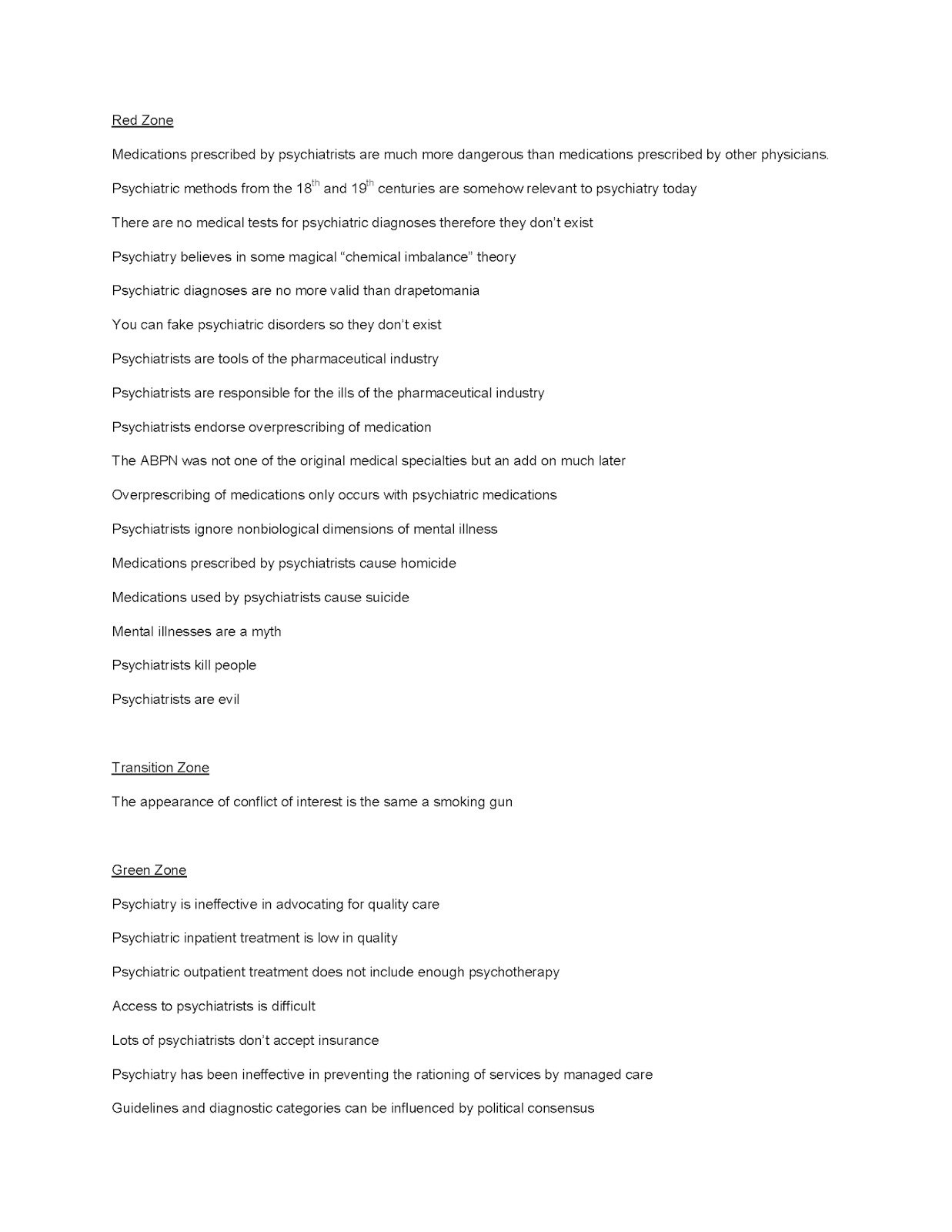
On my drive home today I got the idea of a heat map of psychiatric criticism based on the principles outlined in my previous post. I have started one as shown in the diagram below. The heat zones on the map are general areas corresponding to the parameters outlined in the previous post on rhetoric. In other words red and redder would correspond with more irrational and rhetorical criticism. Green and greener would be more rational criticism and less rhetorical. See the previous post for supporting arguments.
I have started out with a few examples in each zone. I would like to be exhaustive here so send me your favorite one liners about the profession or your most hated psychiatrist and I will try to place it on the heat map. Just a heads up, no personal attacks or identifiers will be tolerated. It may be hard to believe but this is nothing personal. I hope to provide a simple graphical solution to the question of what is and what is not appropriate psychiatric criticism.
I also thought about a couple of reasons why this is important. Several years ago a friend of mine called me up and asked me a question about the American Board of Psychiatry and Neurology. He wanted to know what year it was incorporated. I told him I thought it was on my certificate and I would call him later. When I got home I looked at the certificate and sure enough it read: "Incorporated 1934". I called him with the information and asked him why that was important. He is a social worker and told me that he was at a major DSM training course attended by social workers and the speaker (who was not a psychiatrist) suggested that psychiatry was such an illegitimate field that they were not even one of the original specialties and decided to form the ABPN later in order to seem more legitimate. And this was a guy who was teaching a DSM course! In another similar session, the presenter (also not a psychiatrist) compared the validity of psychiatric diagnoses referring to the Robins and Guze criteria to the validity of drapetomania. For anyone not familiar with this definition, it refers to the idea by a 19th century quack that a slave running away is somehow a mental illness. It really has no connection at all to the idea that there are valid mental illnesses that can be diagnosed and treated. And yet here we have a professional making this comparison. The term was also used in a periodical that is valued for its intellectual appeal, but the interview is embarrassing to read especially the tortured attempt to connect it to DSM-5. My speculation is that the people who use this term have an additional agenda. It is clear that there are are many uses of the loose application of this rhetoric and gaining political advantage is often an overlooked one.
As I look at my initial attempt, I am realizing that I need to figure out a way to group all of the statements at the top firmly in the red zone so that none of them touch the transition area to the green zone.
George Dawson, MD, DFAPA
Supplementary 1:
Here is a working list to consider (click to enlarge all graphics on this page). This is the second version and as of today (2/16/2014) no outside suggestions. The image below is formatted to print or store as a single 8.5 x 11 inch page:
I have started out with a few examples in each zone. I would like to be exhaustive here so send me your favorite one liners about the profession or your most hated psychiatrist and I will try to place it on the heat map. Just a heads up, no personal attacks or identifiers will be tolerated. It may be hard to believe but this is nothing personal. I hope to provide a simple graphical solution to the question of what is and what is not appropriate psychiatric criticism.
I also thought about a couple of reasons why this is important. Several years ago a friend of mine called me up and asked me a question about the American Board of Psychiatry and Neurology. He wanted to know what year it was incorporated. I told him I thought it was on my certificate and I would call him later. When I got home I looked at the certificate and sure enough it read: "Incorporated 1934". I called him with the information and asked him why that was important. He is a social worker and told me that he was at a major DSM training course attended by social workers and the speaker (who was not a psychiatrist) suggested that psychiatry was such an illegitimate field that they were not even one of the original specialties and decided to form the ABPN later in order to seem more legitimate. And this was a guy who was teaching a DSM course! In another similar session, the presenter (also not a psychiatrist) compared the validity of psychiatric diagnoses referring to the Robins and Guze criteria to the validity of drapetomania. For anyone not familiar with this definition, it refers to the idea by a 19th century quack that a slave running away is somehow a mental illness. It really has no connection at all to the idea that there are valid mental illnesses that can be diagnosed and treated. And yet here we have a professional making this comparison. The term was also used in a periodical that is valued for its intellectual appeal, but the interview is embarrassing to read especially the tortured attempt to connect it to DSM-5. My speculation is that the people who use this term have an additional agenda. It is clear that there are are many uses of the loose application of this rhetoric and gaining political advantage is often an overlooked one.

As I look at my initial attempt, I am realizing that I need to figure out a way to group all of the statements at the top firmly in the red zone so that none of them touch the transition area to the green zone.
George Dawson, MD, DFAPA
Supplementary 1:
Here is a working list to consider (click to enlarge all graphics on this page). This is the second version and as of today (2/16/2014) no outside suggestions. The image below is formatted to print or store as a single 8.5 x 11 inch page:

Wednesday, February 12, 2014
The Jerk Store Called
In response to a number of posts to my last post, I decided to take an idea posted by Dr. Steven Reidbord and run with it - but at his request I used a different descriptor than the one he suggested. From my early days as a psychiatrist the general idea in our culture is that you basically listen to all of the criticism of psychiatry no matter how nonsensical it is and put up with it. Act as though it is true. In fact, go ahead and make public policy based on it!
One of the most frequent rationalizations for that passive behavior is that there are always some imperfections and therefore just about any criticism is justified - shut up and take it. At some point it becomes obvious that line of logic excludes most reality. When Dr. Reidbord requested that I not use his brilliant metaphor, the only other thing I could think of was the term "jerk". That reminded me of the Seinfeld episode "The Comeback" and George Costanza's failed retort about the Jerk Store so I thought I would include it here. The following post has otherwise been vetted by a philosophy professor and it looked good to him.
So here goes:
4. It is possible to distinguish jerks from psychiatrists and treat each class accordingly.
So if the basis of your psychiatry bashing lies in arguments 1 - > 3.
The jerk store called and ...........
One of the most frequent rationalizations for that passive behavior is that there are always some imperfections and therefore just about any criticism is justified - shut up and take it. At some point it becomes obvious that line of logic excludes most reality. When Dr. Reidbord requested that I not use his brilliant metaphor, the only other thing I could think of was the term "jerk". That reminded me of the Seinfeld episode "The Comeback" and George Costanza's failed retort about the Jerk Store so I thought I would include it here. The following post has otherwise been vetted by a philosophy professor and it looked good to him.
So here goes:
The Jerk Argument
It is a given that the the class of psychiatrists like all major subgroups of people and workers contains some jerks. In this case a jerk can be defined as whatever a hater of psychiatry likes it to be.
Possible conclusions:
1. All psychiatrists
are jerks.
2. Psychiatrists are inherently
evil whether they are jerks or not, jerks are not really any worse.
3. All psychiatrists
should be treated like jerks whether they are jerks or not.
4. It is possible to distinguish jerks from psychiatrists and treat each class accordingly.
5. It is inaccurate
at best to generalize to the entire class of psychiatrists what is observed in
the jerks.
1-> 3 are positions of the various psychiatry bashers
whether they are antipsychiatrists or not, or formal antipsychiatry
philosophies or not. That encompasses a
full range of cults, lone critics with an axe to grind, academics, competing professionals, critics with a book or column to sell, and scandal
mongers. It may even contain some
critics with a legitimate criticism but they end up including these additional
invalid arguments in the body of their work.
These positions contain various logical fallacies and are unsupported at
that level. It is also interesting to
contemplate that these initial conclusions are never applied to any other medical specialty and ideally are not applied to any group of people. Think about substituting any other societal group in those sentences as see what you come up with. Since they are illogical arguments the only
possible conclusion is that psychiatrists as a group are clearly discriminated
against and the basis for that discrimination is irrational.
Jerk logic also has implications for the way that the
government and healthcare organizations treat psychiatrists. The government and managed care attitude toward
psychiatrists is probably most accurately captured in 3. Every regulation
and interaction with a managed care company reinforces that idea. It could also be argued that the managed care
industry is in the business of converting psychiatrists into jerks. That is true if they are employed by the managed
care companies directly or indirectly working on the "medication management" assembly line.
My positions are best represented by 4 and 5. That is the evidence I focus on in this
blog. I have debated with myself about
whether I should fight the bashers head on, but they generally not really
interested in debating logic, scientific evidence, or any evidence contrary to
their argument. Per my previous post they are engaged in sophistry and will post endless fallacious arguments and say that ain't so. So fighting them by definition
is futile and they can aggregate to any number of psychiatry bashing sites on
the Internet where they can revel in their rhetoric.
So if the basis of your psychiatry bashing lies in arguments 1 - > 3.
The jerk store called and ...........
George Dawson, MD, DFAPA
Supplementary 1: As I was preparing this post I noticed this post popped up on the Shrink Rap blog entitled Are Psychiatrists Evil? and that dovetails nicely with my small study in rhetoric. There are several previous posts here that examine this rhetoric in different ways like The Myth of the Psychiatrist as Bogeyman and Why Do They Hate Us?
Supplementary 2: Per this previous post - the antipsychiatry philosophies follow per the reference below. It is also a good example of a potential critic with something useful to say but using invalid arguments of the form given in the body of the above post. A standard tactic is falsely claiming that psychiatrists hold a certain position and then attacking that position as though it is true.
Fulford KWM, Thornton T, Graham G. Oxford Textbook of Philosophy and Psychiatry. Oxford University Press, Oxford, 2006: 17.
"Some of the main models advanced by antipsychiatrists, mainly in the 1960s and 1970s, can be summarized thus:
1. The psychological model...
2. The labeling model...
3. Hidden meaning models...
4. Unconscious mind models...
5. Political control models..." <-Foucault is located here. (p. 17)
Supplementary 3: Of course it is always important to recognize the bullshitters - Is Bullshit A Better Term Than Antipsychiatry?
Supplementary 1: As I was preparing this post I noticed this post popped up on the Shrink Rap blog entitled Are Psychiatrists Evil? and that dovetails nicely with my small study in rhetoric. There are several previous posts here that examine this rhetoric in different ways like The Myth of the Psychiatrist as Bogeyman and Why Do They Hate Us?
Supplementary 2: Per this previous post - the antipsychiatry philosophies follow per the reference below. It is also a good example of a potential critic with something useful to say but using invalid arguments of the form given in the body of the above post. A standard tactic is falsely claiming that psychiatrists hold a certain position and then attacking that position as though it is true.
Fulford KWM, Thornton T, Graham G. Oxford Textbook of Philosophy and Psychiatry. Oxford University Press, Oxford, 2006: 17.
"Some of the main models advanced by antipsychiatrists, mainly in the 1960s and 1970s, can be summarized thus:
1. The psychological model...
2. The labeling model...
3. Hidden meaning models...
4. Unconscious mind models...
5. Political control models..." <-Foucault is located here. (p. 17)
Supplementary 3: Of course it is always important to recognize the bullshitters - Is Bullshit A Better Term Than Antipsychiatry?
Saturday, February 8, 2014
An Obvious Response to "Psychiatry Gone Astray"
David Healy has what I consider to be inconsistent viewpoints. I have previously critiqued his viewpoint on the "addictive" qualities of antidepressants (they clearly are not) and whole heartedly endorsed his position that pills don't treat depression - psychiatrists do. He recently posted what I would refer to as a screed written by a Danish internist on (what else?) all of the problems with psychiatry. The obvious lack of symmetry here is striking. You won't find a psychiatrist anywhere posting a similar piece about internal medicine, even though it could be easily done and would probably be more evidence based. In that regard this physician has slightly more credibility that the typical layperson screed against psychiatry - but not much more. What follows is my point by point refutation of the "myths". They are mythical in that they are from the mind of the author - I know of no psychiatrist who thinks this way.
Myth 1: Your disease is caused by a chemical imbalance in the brain -
Myth 2: It’s no problem to stop treatment with antidepressants -
Myth 3: Psychotropic Drugs for Mental Illness are like Insulin for Diabetes -
Myth 4: Psychotropic drugs reduce the number of chronically ill patients -
Myth 5: Happy pills do not cause suicide in children and adolescents -
Myth 7: Happy pills are not addictive -
Myth 8: The prevalence of depression has increased a lot -
Myth 9: The main problem is not overtreatment, but undertreatment -
Myth 10: Antipsychotics prevent brain damage -
Myth 1: Your disease is caused by a chemical imbalance in the brain -
This is a red herring that is frequently marched out in the media and often connected with a conspiracy theory that psychiatrists are tools of pharmaceutical companies who probably originated this idea. What are the facts? Psychiatry has at least a century old tradition of researching all possible etiologies for mental health problems. Psychiatrists were among the first people to look at the effects of social deprivation in orphanages, the effects of acute grief and loss, the effects of psychological trauma, the effects of a full gamut of psychotherapies, and the effects of family and environment. The biopsychosocial formulation of Engel in 1977 was an advance detailed in Science magazine. Any comprehensive psychiatric formulation covers all possible etiologies (as an obvious example see Systematic Psychiatric Evaluation by Chisolm and Lyketsos). In addition there are many clinical methods where the diagnostic formulation is essential for the treatment plan for psychotherapy based treatment. By definition that formulation would have few biological references. So the alleged myth fails at the clinical level.
It fails even worse at the neurobiological level. Chemical imbalance rhetoric always seems to ignore one huge fact and that is Eric Kandel's classic article on plasticity in 1979 in the New England Journal of Medicine. Certainly any psychiatrist who saw that article has never bought into a "chemical imbalance" idea and I can recall mocking the idea when pharmaceutical companies presented it to my colleagues and I in medical school. So why don't we hear: "Your disease is caused by plasticity?" Probably because they gave Eric Kandel the Nobel Prize for it.
Another red herring. I have trained psychiatrists, internists, family physicians and medical students and taught them psychopharmacology. A general principle of psychopharmacology is no abrupt changes in therapy and most drug prescribing information suggests that. I routinely address this issue as part of informed consent and advise people that there may be difficulty discontinuing antidepressants and describe the potential symptoms. This criticism from an internist has a certain degree of asymmetry to it. Certainly there are medications prescribed by internists that cause both acute withdrawal and discontinuation symptoms. My impression is that many adults who see internists are basically going along with life long therapy in many cases for conditions that could be treated by psychosocial measures. It is quite easy to criticize if you are never faced with the prospect of discontinuing therapy.
The author here conflates the certainty of insulin deficiency with pathophysiological certainty in medicine and how that correlates with prescribed treatment. Certainly that is not the case in diabetes mellitus Type II or the recent example I provided with an asthma exacerbation. In fact the pathophysiology in those heterogenous groups are about as accurate as endophenotypes in psychiatry. Am I getting prednisone for my asthma because I am deficient in prednisone? Am I getting it because of some specific pathophysiological mechanism rather than a shotgun approach to shut down all of my inflammatory signalling? Was predisone prescribed only based on the purported pathophysiological mechanisms? The answer to all three questions is - of course not. If the author is really concerned about medication side effects, I can't think of any psychiatric medication that is the equal of prednisone but I am certainly not going to suggest that it should not be prescribed.
I don't know of anyone who has actually suggested this and from an internal medicine perspective does it make sense? Here are a few additional comparison statistics on asthma and hypertension for example. There is a 10% prevalence of asthma in the developed world. Only 1 in 7 has their symptoms in good control. People continue to die of asthma possible as many as 1/250 deaths world wide. In the case of hypertension, 31% of Americans have it and another 30% have prehypertension. Only 47% have adequate blood pressure control. There is really not much evidence that medications prescribed by internists are much more effective than what he refers to as "psychotropic drugs" and that is borne out in a previous analysis and my own recent experience with the health care system.
I find this argument also demeaning to anyone with a severe psychiatric disorder who is interested in staying out of hospitals and being able to function or trying to avoid a suicide attempt. Being able to adhere to that kind of plan depends on multiple variables including taking medications. It is reckless to suggest otherwise and any psychiatrist knows about severe adverse outcomes that have occurred as a result of stopping a medication. The author conveniently plugs his book at this point.
The author reveals his antipathy to medication used by psychiatrists here by referring to antidepressants as "happy pills." I know of no psychiatrist who I have ever met who calls antidepressants "happy pills" and in fact most of us are engaged in trying to find an effective medication with minimal side effects. David Healy himself describes this as one of the primary functions of psychiatrists. On the actual suicide issue, psychiatrists goal is preventing suicide. Suicide is a possible outcome of all clinical encounters and psychiatrists follow this symptom closely.
Saying that happy pills are a cause of suicide is the equivalent of saying that "sugar medicine" (insulin) is a cause of hypoglycemia that harms children and therefore it should not be prescribed.
Myth 6: Happy pills have no side effects -
The author has one legitimate point in that depression screening is not a good idea but in his zeal to criticize everything psychiatric he has to whip that into "happy pills have no side effects". Of course they do and I have elaborated my clinical method on how to approach that in detail. He goes on to make an anecdotal argument about single study results versus "what the company says." In fact, companies have to rigorously record side effects in clinical trials and all of that is recorded in the FDA prescribing information. Looking at standard FDA reported data for sexual side effects (his example) the number for all SSRI antidepressants is 9-37% and not the 5% figure suggested by the author. (see page 1684 of Drugs Facts and Comparisons 2013).
This is interesting because of David Healy's confusion on this subject. It indicates a serious lack of knowledge about addiction because there are no behavioral features of antidepressant medications or animal models that describe these drugs as addictive. They have no street value and they will not make you high. The authors comparison to amphetamine is completely off the mark and consistent with his general lack of knowledge of addiction.
He has to attach epidemiological data on depression in order to attack the argument that increasing antidepressant use is not a problem because of the increasing prevalence. He offers a sarcastic comment as evidence and misses both the issue of why antidepressant prescriptions are increasing and the real data on the prevalence of depression. Even if his argument is correct, since 80% of antidepressants are prescribed by primary care physicians wouldn't this be "Primary care gone astray?"
On the epidemiology issue I would encourage a quick look at an actual text on the issue like Textbook of Psychiatric Epidemiology, 3rd Edition.(p 292) The authors look at 30 national and international studies and do not conclude that there is an increasing prevalence of depression, but that variation is likely due to methodological differences and sociocultural factors.
On the epidemiology issue I would encourage a quick look at an actual text on the issue like Textbook of Psychiatric Epidemiology, 3rd Edition.(p 292) The authors look at 30 national and international studies and do not conclude that there is an increasing prevalence of depression, but that variation is likely due to methodological differences and sociocultural factors.
More sarcasm as evidence here. I debunked the arithmetic used in this argument in an earlier Washington Post piece. This is also a huge disservice to people with severe mental illness and addictions in this country who have been thrown out of treatment, received useless hospital treatments, and restricted from medications by managed care. The primary prescribers of antidepressants (by far) are primary care physicians and it is certainly possible that they are prescribing too many antidepressants. But don't blame psychiatrists for that.
More rhetoric. In this case he is using a research hypothesis and suggesting that this has something to do with clinical psychiatry. Despite significant obstacles, psychiatric research at the neurobiological level continues and studies on imaging are a large part of that process. One of the major areas has to do with brain volumes and their implications. The author presumes he knows what the outcome of that research will be. He also talks about antipsychotic medication with the arrogance of a person who does not have to treat acutely psychotic people and incredibly talks about these drugs killing people. In fact, the number one killer of people with severe mental illnesses is tobacco smoke and there is ample evidence that they get suboptimal primary care.
At the end of this refutation what have we learned? I am more skeptical than ever of David Healy and his web site. I thought he did good work with his investigation of SSRIs and his analysis of the role of psychiatrists as opposed to medications was accurate. But I can't ignore the fact that he places this screed on his web site. He also lists himself as a "scientist" and this screed contains surprisingly little science. It is essentially all rhetoric and politics.
It is one thing to ridicule psychiatrists but the obvious concern here is that it stigmatizes people who need treatment especially treatment with medication who are actively denied treatment in the U.S. on an ongoing basis. The author here uses a familiar dynamic that I have described in the past. He suggests that internists (like the author here) have clearly superior methods or pathophysiological mechanisms than psychiatrists but they don't. In terms of the accusation of overprescribing, it is well know in the US that the 20 year CDC initiative to control antibiotic overprescribing is a failure. Some authors believe that this heralds a new "post antibiotic era" where untreatable infections will become the rule.
It is one thing to ridicule psychiatrists but the obvious concern here is that it stigmatizes people who need treatment especially treatment with medication who are actively denied treatment in the U.S. on an ongoing basis. The author here uses a familiar dynamic that I have described in the past. He suggests that internists (like the author here) have clearly superior methods or pathophysiological mechanisms than psychiatrists but they don't. In terms of the accusation of overprescribing, it is well know in the US that the 20 year CDC initiative to control antibiotic overprescribing is a failure. Some authors believe that this heralds a new "post antibiotic era" where untreatable infections will become the rule.
It seems to me that internists have enough to focus on in their own specialty before criticizing an area that they obviously know so little about. It also seems that if you claim your web site is scientific, you should probably put a little science on it. The author here also states that he is affiliated with the Nordic Cochrane Center and I think that anyone who considers the output of that Institute should consider what he has written here and the relevant conflict of interest issues.
George Dawson, MD, DFAPA
Supplementary 1: About a month after this post was completed Ronald Pies, MD came out with an article in the Psychiatric Times entitled Nuances, Narratives, and the “Chemical Imbalance” Debate. He presents very similar arguments to the ones presented here and concludes that it is time for the critics using this false argument to give it up. I also like his characterization of "a recent online polemic posing as investigative journalism" and how the "chemical imbalance hypothesis" is used to mischaracterize psychiatry. He also provides a link to a 2011 article that he wrote that contain the following quote:
"I am not one who easily loses his temper, but I confess to experiencing markedly increased limbic activity whenever I hear someone proclaim, “Psychiatrists think all mental disorders are due to a chemical imbalance!” In the past 30 years, I don’t believe I have ever heard a knowledgeable, well-trained psychiatrist make such a preposterous claim, except perhaps to mock it. "
Supplementary 1: About a month after this post was completed Ronald Pies, MD came out with an article in the Psychiatric Times entitled Nuances, Narratives, and the “Chemical Imbalance” Debate. He presents very similar arguments to the ones presented here and concludes that it is time for the critics using this false argument to give it up. I also like his characterization of "a recent online polemic posing as investigative journalism" and how the "chemical imbalance hypothesis" is used to mischaracterize psychiatry. He also provides a link to a 2011 article that he wrote that contain the following quote:
"I am not one who easily loses his temper, but I confess to experiencing markedly increased limbic activity whenever I hear someone proclaim, “Psychiatrists think all mental disorders are due to a chemical imbalance!” In the past 30 years, I don’t believe I have ever heard a knowledgeable, well-trained psychiatrist make such a preposterous claim, except perhaps to mock it. "
Readers of this blog have heard seen me say this many times before. It is good to see these opinions being offered in the more mainstream media. It is also good to see Dr. Pies taking calling a critic on what is rhetoric rather than reality. Well done.
Supplementary 2: I have an updated post on the issue of how medical syndromes and psychiatric syndromes are far more similar than different and how there is a complete lack of criticism relative to psychiatry. (added on September 3, 2015).
Supplementary 2: I have an updated post on the issue of how medical syndromes and psychiatric syndromes are far more similar than different and how there is a complete lack of criticism relative to psychiatry. (added on September 3, 2015).
Tuesday, January 28, 2014
Is Bullshit A Better Term Than Antipsychiatry?
I saw Professor Harry G. Frankfurt on David Letterman a few years ago. He was there to explain his recently released book entitled On Bullshit. He was joking with Dave about how somebody called him up one day and wanted to make one of his essays into a book. When asked how that happens he said "Bigger fonts and wider margins." I don't know if he was consciously trying to convey the idea that he was no bullshitter. In the book he is listed as a renowned moral philosopher and Professor of Philosophy Emeritus at Princeton University. The book is inexpensive and a quick read. Imagine an essay stretched into a book the size of an address book in 67 pages of 12 point font and 1 inch margins.
Despite the catchy title and obvious magic of marketing, I really like this book. First off, it is written by a professor of moral philosophy and I always like hearing from the experts. Secondly, Professor Frankfurt looks at the differences between lying and bullshitting and all points in between. The opening line is classic:
"One of the most salient features of our culture is that there is so much bullshit." (p. 1)
In the opening paragraph he goes on to explain that study of bullshit has not attracted much attention because most people take it for granted that they can recognize it and not get taken in. The result is a lack of theoretical understanding of bullshit. His stated goal is to articulate what it is and what it is not.
I will let any interested reader acquire a copy of the book. With its brevity I run the risk of reciting all of the high points in this post. I will quote two more lines from the book because of the amount of information they convey:
"The realms of advertising and of public relations, and the nowadays closely related realm of politics are replete with instances of bullshit so unmitigated that they can serve among the most indisputable and classic paradigms of the concept." (p. 22)
Professor Frankfurt goes on to develop the idea that the bullshitter can be imprecise and that unlike a liar he has no prerequisite that he knows the truth. He is bluffing and faking his way through. Bullshitters don't reject the truth, they pay no attention to it. In the technical sense, bullshit is not false it is phony. And perhaps the essence as it applies to a professional field (I have to use a third quote):
"Bullshitting is unavoidable whenever circumstances require someone to talk without knowing what he is talking about." (p. 63).
The last requirement is interesting because there are conscious and unconscious components. The unconscious component is the innate ability that most people have to practice folk psychology. It is the equivalent of a social brain. We recognize certain patterns in people and how they behave that allow us to make predictions about their behavior. I am quite sure that many people mistake that ability for being trained as a psychiatrist. I base that a lot on what people tell me that they "observe" and "diagnose". For all of the concern about the "medicalization" of the population - the average folk psychologist has a much lower threshold than any psychiatrist I have ever met. For example, in various workplaces I have been warned by employee supervisors that three separate coworkers that I would be working with were "paranoid", "obsessive compulsive" and "borderline". I did not see any characteristics that the amateur diagnosticians warned me about and in all three cases, I found these co workers to be excellent and had absolutely no problems working with them. This is probably an extension of Dr. Frankfurt's work - the unconscious aspects of bullshitting but I expect that it correlates closely with some descriptions in a classic paper on prevarication.
But in the case of talking without expertise, I am afraid that the unconscious aspects cover a very small part of the bullshitting spectrum. You can go to any site where psychiatry is routinely criticized, attacked or vilified and you will see any number of posts by the anonymous posters who talk about their anecdotes and proclamations about psychiatry. Many are bombastic. None are challenged. It is the general tenor of many of these sites that psychiatrists are basically incompetent assholes (yeah I said it) and should be barred from practicing medicine. Psychiatrists only injure people and have never helped anyone. If they produce any coherent arguments they generally fit the psychiatrist as bogeyman dynamic that I previously described. Some people who have seen a psychiatrist may grudgingly admit it, but nobody ever seems to acknowledge that a psychiatrist did anything to help them. The more erudite approach may be to critique psychiatry without acknowledging that psychiatrists in fact are better critics and have critiqued their own field. If anyone is questioned they may produce the indignant response: "Are you calling me an antipsychiatrist?"
Some of what passes for criticism actually ignores what really happened and attempts to cast modern psychiatry in a light that is based more on historical spin than what is applicable today. Some of these efforts are actually considered to be "good" criticism, even though it is clear to any trained psychiatrist that the author knows little to nothing about the field. You would think that anyone interested in developing a negative narrative about psychiatry would do the basic research of picking up a copy of Shorter's A History of Psychiatry and reading about the ways things were before there was any psychiatry. In his text Shorter describes severe mental illness as a death sentence (p. 2) and the following historical observation: "In a world without psychiatry, rather than being tolerated or indulged, the mentally ill were treated with a savage lack of feeling. Before the advent of the therapeutic asylum, there was no golden era, no idyllic refuge for those deviant from the values of capitalism. To maintain otherwise is a fantasy." (p. 4). But the ignorance of psychiatry extends far beyond the historical. It is apparent that many of the critics have no knowledge of the current current psychiatric literature. They often reference the New York Times as though it is authoritative. They criticize highly technical subjects and it is apparent that they have not read a journal or a book from that field. Like Frankfurt's definition they pay no attention to the truth.
Based on Professor Frankfurt's essay, I conclude that bullshit is a much more appropriate characterization of many of the misrepresentations of psychiatry. I would also suggest it may be more politically correct than implying that the author is a member of a cult or a school of philosophy. (see the footnote at this link)
They are quite simply a bullshitter and bullshit remains as it always has been (even pre-Frankfurt) - bullshit.
George Dawson, MD, DFAPA
Harry G. Frankfurt. On Bullshit. Princeton University Press, Princeton, NJ, 2005.
Despite the catchy title and obvious magic of marketing, I really like this book. First off, it is written by a professor of moral philosophy and I always like hearing from the experts. Secondly, Professor Frankfurt looks at the differences between lying and bullshitting and all points in between. The opening line is classic:
"One of the most salient features of our culture is that there is so much bullshit." (p. 1)
In the opening paragraph he goes on to explain that study of bullshit has not attracted much attention because most people take it for granted that they can recognize it and not get taken in. The result is a lack of theoretical understanding of bullshit. His stated goal is to articulate what it is and what it is not.
I will let any interested reader acquire a copy of the book. With its brevity I run the risk of reciting all of the high points in this post. I will quote two more lines from the book because of the amount of information they convey:
"The realms of advertising and of public relations, and the nowadays closely related realm of politics are replete with instances of bullshit so unmitigated that they can serve among the most indisputable and classic paradigms of the concept." (p. 22)
Professor Frankfurt goes on to develop the idea that the bullshitter can be imprecise and that unlike a liar he has no prerequisite that he knows the truth. He is bluffing and faking his way through. Bullshitters don't reject the truth, they pay no attention to it. In the technical sense, bullshit is not false it is phony. And perhaps the essence as it applies to a professional field (I have to use a third quote):
"Bullshitting is unavoidable whenever circumstances require someone to talk without knowing what he is talking about." (p. 63).
The last requirement is interesting because there are conscious and unconscious components. The unconscious component is the innate ability that most people have to practice folk psychology. It is the equivalent of a social brain. We recognize certain patterns in people and how they behave that allow us to make predictions about their behavior. I am quite sure that many people mistake that ability for being trained as a psychiatrist. I base that a lot on what people tell me that they "observe" and "diagnose". For all of the concern about the "medicalization" of the population - the average folk psychologist has a much lower threshold than any psychiatrist I have ever met. For example, in various workplaces I have been warned by employee supervisors that three separate coworkers that I would be working with were "paranoid", "obsessive compulsive" and "borderline". I did not see any characteristics that the amateur diagnosticians warned me about and in all three cases, I found these co workers to be excellent and had absolutely no problems working with them. This is probably an extension of Dr. Frankfurt's work - the unconscious aspects of bullshitting but I expect that it correlates closely with some descriptions in a classic paper on prevarication.
But in the case of talking without expertise, I am afraid that the unconscious aspects cover a very small part of the bullshitting spectrum. You can go to any site where psychiatry is routinely criticized, attacked or vilified and you will see any number of posts by the anonymous posters who talk about their anecdotes and proclamations about psychiatry. Many are bombastic. None are challenged. It is the general tenor of many of these sites that psychiatrists are basically incompetent assholes (yeah I said it) and should be barred from practicing medicine. Psychiatrists only injure people and have never helped anyone. If they produce any coherent arguments they generally fit the psychiatrist as bogeyman dynamic that I previously described. Some people who have seen a psychiatrist may grudgingly admit it, but nobody ever seems to acknowledge that a psychiatrist did anything to help them. The more erudite approach may be to critique psychiatry without acknowledging that psychiatrists in fact are better critics and have critiqued their own field. If anyone is questioned they may produce the indignant response: "Are you calling me an antipsychiatrist?"
Some of what passes for criticism actually ignores what really happened and attempts to cast modern psychiatry in a light that is based more on historical spin than what is applicable today. Some of these efforts are actually considered to be "good" criticism, even though it is clear to any trained psychiatrist that the author knows little to nothing about the field. You would think that anyone interested in developing a negative narrative about psychiatry would do the basic research of picking up a copy of Shorter's A History of Psychiatry and reading about the ways things were before there was any psychiatry. In his text Shorter describes severe mental illness as a death sentence (p. 2) and the following historical observation: "In a world without psychiatry, rather than being tolerated or indulged, the mentally ill were treated with a savage lack of feeling. Before the advent of the therapeutic asylum, there was no golden era, no idyllic refuge for those deviant from the values of capitalism. To maintain otherwise is a fantasy." (p. 4). But the ignorance of psychiatry extends far beyond the historical. It is apparent that many of the critics have no knowledge of the current current psychiatric literature. They often reference the New York Times as though it is authoritative. They criticize highly technical subjects and it is apparent that they have not read a journal or a book from that field. Like Frankfurt's definition they pay no attention to the truth.
Based on Professor Frankfurt's essay, I conclude that bullshit is a much more appropriate characterization of many of the misrepresentations of psychiatry. I would also suggest it may be more politically correct than implying that the author is a member of a cult or a school of philosophy. (see the footnote at this link)
They are quite simply a bullshitter and bullshit remains as it always has been (even pre-Frankfurt) - bullshit.
George Dawson, MD, DFAPA
Harry G. Frankfurt. On Bullshit. Princeton University Press, Princeton, NJ, 2005.
Saturday, May 25, 2013
The Real Role of Biological Tests in Psychiatry
The idea of a "biological test" in psychiatry has appeared on the internet recently, primarily as a way to deny that psychiatric disorders exist. The contention is that because there is no medical test for a psychiatric disorder - it must not exist. Time to add a balanced view.
As a backdrop, most people do not understand the concept of "tests" in medicine until they have a problem and realize that the problem is not reflected in the tests ordered by their doctor. That is a very common experience. Some studies show that up to 30% of patients presenting to a clinic for investigation of a symptom never find out what the cause of that symptom was. That is true even after they were given the usual panel of blood tests, imaging studies, and electrophysiological studies. The assumption that symptoms and disorders in medicine are all diagnosable by a "test" is incorrect.
The second problem occurs at the level of test interpretation. When a doctor orders a test they have to interpret it correctly and in many cases the idea of an "abnormal" test is blurred by biological variation. The evaluation of back pain using imaging studies like MRI scans is a good case in point. As people age there is a greater likelihood that an abnormal MRI scan of the spine is not necessarily the cause of their back pain. That has very important implications for treatment and the physician interpreting the test may will definitely be influenced by their specialty training, their own personal experience, their knowledge and examination of the patient, and possibly treatment guidelines that they may be mandated to follow. There is also the question of false positive and false negative testing. The recent controversy about the utility of prostate specific antigen (PSA) testing for prostate cancer is another good example. The current guideline says that this test has too many false positive results to use for treatment planning and further invasive procedures. Even in the case where the diagnosis is made by a specific number there is always the question of whether the test number is accurate or not. I have frequently repeated thyroid function tests that seemed to show hyperthyroidism only to see them in the normal range on repeat testing. It is obvious to physicians that the so-called biological tests in medicine have their limitations and always need to be interpreted in the context of a comprehensive evaluation of the patient.
How are biological tests currently used in psychiatry? It turns out that there are a lot of applications similar to the rest of medicine.
1. To detect a medical cause of a psychiatric disorder. The DSM classification has an entire set of disorders that are caused by underlying neurological illnesses, endocrine disorders, and infectious diseases that need to be recognized and treated. They often present as psychiatric disorders. In my experience of treating people with severe problems, up to 15% of the psychiatric presentations had an underlying medical illness that either was a direct cause of the "psychiatric" symptoms or it made a psychiatric disorder worse. In that case the psychiatrist has to be trained to order the appropriate tests, make the diagnosis and refer the patient for treatment of the underlying disorder.
2. To screen for medical illnesses that complicate the psychiatric disorder or its treatment. A good example here is screening blood tests and electrocardiograms based on the clinical assessment of the patient and the likelihood that a disease is present. At times patients present with significant problems that require urgent treatment that they are unaware of. A good example would be detecting complete heart block on an ECG because of a patient's responses to the cardiovascular review of systems and the fact that an antidepressant was going to be prescribed.
3. To monitor the safety of biological treatments. There is probably no better example than the FDA focus on cardiac conduction and how that can be affected by medications. The most recent warning occurred with citalopram. This antidepressant has been used for over a decade by psychiatrists and was widely considered to be a very safe medication. Both the FDA and the Mayo Clinic have guidelines about how this problem needs to be assessed and that is a combination of clinical assessment and electrocardiograms. In some cases electrocardiograms and referrals to electrophysiologists are required. In light of this information psychiatrists need to have access to these ECGs and a plan to address any abnormalities. As specialists, it is common to see patients who are referred taking doses of citalopram that exceed current FDA guidelines and that may involve testing and a plan to modify the dose of antidepressant.
4. To identify medical emergencies in patients who are being followed for a psychiatric disorder. Many patients who see psychiatrists either do not have primary care physicians or are very reluctant to see them. A psychiatrist in this position needs to make every effort possible to encourage the patient to establish primary care, but even then medical emergencies need to be recognized and appropriately triaged. That can happen more quickly if testing is available to facilitate the referral. If a patient presents with jaundice, medical consultants are more likely to see him quickly if some basic testing is done that can be discussed with the consultant.
5. To identify neurobiological correlates of psychiatric disorders. A common example is an abnormal brain imaging or electrophysiological study that was ordered because of an acute or progressive behavioral change.
6. For heuristic purposes. The classic example of a test done for heuristic purposes was the dexamethasone suppression test. At various times it was suggested as a test for various forms of severe depression and suicide risk. The test is rarely done today because of the false positive errors but it helped generate a couple of decades of research on the neuroendocrinology associated with psychiatric disorders.
Some of the articles currently out there on the internet deny the existence of psychiatric disorders because there is no biological test for these disorders like depression or schizophrenia. That really does not differentiate psychiatric disorders from neurological or rheumatic disorders that may have some supporting markers but that in general depend more on pattern recognition and less on a gold standard or pathognomonic test. From a paper that addresses that subject (1):
"Although the results are often useful, they can be misleading. Few tests yield results that are pathognomonic for particular diseases. For these reasons, test results for autoantibodies alone are insufficient to establish the diagnosis of a systemic rheumatic disease; they must always be interpreted in the clinical context. Positive results for tests such as the ANA test are seen quite commonly in patients with nonrheumatic diseases and even among normal, healthy persons..."
The key sentence here is: "Few tests yield results that are pathognomonic for particular diseases." That would mean that in fact there are few so-called gold standard medical tests that confirm or deny the existence of a diagnosis. Up to 30% of people presenting to a medical clinic for an evaluation of symptoms will never have a diagnosis to explain their symptoms no matter how many tests they have. People with real illnesses often are frustrated by the fact that the test results they get are often equivocal. Obvious conditions that have no biomarkers range from migraine headaches to Alzheimer's Disease. I don't think that any rational person would suggest that neither of these conditions exist. People who have first hand experience with severe mental disorders know that the profound emotional and cognitive changes that they see in their friend of family member is real - whether there is a biomarker or not.
George Dawson, MD, DFAPA
As a backdrop, most people do not understand the concept of "tests" in medicine until they have a problem and realize that the problem is not reflected in the tests ordered by their doctor. That is a very common experience. Some studies show that up to 30% of patients presenting to a clinic for investigation of a symptom never find out what the cause of that symptom was. That is true even after they were given the usual panel of blood tests, imaging studies, and electrophysiological studies. The assumption that symptoms and disorders in medicine are all diagnosable by a "test" is incorrect.
The second problem occurs at the level of test interpretation. When a doctor orders a test they have to interpret it correctly and in many cases the idea of an "abnormal" test is blurred by biological variation. The evaluation of back pain using imaging studies like MRI scans is a good case in point. As people age there is a greater likelihood that an abnormal MRI scan of the spine is not necessarily the cause of their back pain. That has very important implications for treatment and the physician interpreting the test may will definitely be influenced by their specialty training, their own personal experience, their knowledge and examination of the patient, and possibly treatment guidelines that they may be mandated to follow. There is also the question of false positive and false negative testing. The recent controversy about the utility of prostate specific antigen (PSA) testing for prostate cancer is another good example. The current guideline says that this test has too many false positive results to use for treatment planning and further invasive procedures. Even in the case where the diagnosis is made by a specific number there is always the question of whether the test number is accurate or not. I have frequently repeated thyroid function tests that seemed to show hyperthyroidism only to see them in the normal range on repeat testing. It is obvious to physicians that the so-called biological tests in medicine have their limitations and always need to be interpreted in the context of a comprehensive evaluation of the patient.
How are biological tests currently used in psychiatry? It turns out that there are a lot of applications similar to the rest of medicine.
1. To detect a medical cause of a psychiatric disorder. The DSM classification has an entire set of disorders that are caused by underlying neurological illnesses, endocrine disorders, and infectious diseases that need to be recognized and treated. They often present as psychiatric disorders. In my experience of treating people with severe problems, up to 15% of the psychiatric presentations had an underlying medical illness that either was a direct cause of the "psychiatric" symptoms or it made a psychiatric disorder worse. In that case the psychiatrist has to be trained to order the appropriate tests, make the diagnosis and refer the patient for treatment of the underlying disorder.
2. To screen for medical illnesses that complicate the psychiatric disorder or its treatment. A good example here is screening blood tests and electrocardiograms based on the clinical assessment of the patient and the likelihood that a disease is present. At times patients present with significant problems that require urgent treatment that they are unaware of. A good example would be detecting complete heart block on an ECG because of a patient's responses to the cardiovascular review of systems and the fact that an antidepressant was going to be prescribed.
3. To monitor the safety of biological treatments. There is probably no better example than the FDA focus on cardiac conduction and how that can be affected by medications. The most recent warning occurred with citalopram. This antidepressant has been used for over a decade by psychiatrists and was widely considered to be a very safe medication. Both the FDA and the Mayo Clinic have guidelines about how this problem needs to be assessed and that is a combination of clinical assessment and electrocardiograms. In some cases electrocardiograms and referrals to electrophysiologists are required. In light of this information psychiatrists need to have access to these ECGs and a plan to address any abnormalities. As specialists, it is common to see patients who are referred taking doses of citalopram that exceed current FDA guidelines and that may involve testing and a plan to modify the dose of antidepressant.
4. To identify medical emergencies in patients who are being followed for a psychiatric disorder. Many patients who see psychiatrists either do not have primary care physicians or are very reluctant to see them. A psychiatrist in this position needs to make every effort possible to encourage the patient to establish primary care, but even then medical emergencies need to be recognized and appropriately triaged. That can happen more quickly if testing is available to facilitate the referral. If a patient presents with jaundice, medical consultants are more likely to see him quickly if some basic testing is done that can be discussed with the consultant.
5. To identify neurobiological correlates of psychiatric disorders. A common example is an abnormal brain imaging or electrophysiological study that was ordered because of an acute or progressive behavioral change.
6. For heuristic purposes. The classic example of a test done for heuristic purposes was the dexamethasone suppression test. At various times it was suggested as a test for various forms of severe depression and suicide risk. The test is rarely done today because of the false positive errors but it helped generate a couple of decades of research on the neuroendocrinology associated with psychiatric disorders.
Some of the articles currently out there on the internet deny the existence of psychiatric disorders because there is no biological test for these disorders like depression or schizophrenia. That really does not differentiate psychiatric disorders from neurological or rheumatic disorders that may have some supporting markers but that in general depend more on pattern recognition and less on a gold standard or pathognomonic test. From a paper that addresses that subject (1):
"Although the results are often useful, they can be misleading. Few tests yield results that are pathognomonic for particular diseases. For these reasons, test results for autoantibodies alone are insufficient to establish the diagnosis of a systemic rheumatic disease; they must always be interpreted in the clinical context. Positive results for tests such as the ANA test are seen quite commonly in patients with nonrheumatic diseases and even among normal, healthy persons..."
The key sentence here is: "Few tests yield results that are pathognomonic for particular diseases." That would mean that in fact there are few so-called gold standard medical tests that confirm or deny the existence of a diagnosis. Up to 30% of people presenting to a medical clinic for an evaluation of symptoms will never have a diagnosis to explain their symptoms no matter how many tests they have. People with real illnesses often are frustrated by the fact that the test results they get are often equivocal. Obvious conditions that have no biomarkers range from migraine headaches to Alzheimer's Disease. I don't think that any rational person would suggest that neither of these conditions exist. People who have first hand experience with severe mental disorders know that the profound emotional and cognitive changes that they see in their friend of family member is real - whether there is a biomarker or not.
George Dawson, MD, DFAPA
Reference:
1: Arthur Kavanaugh, Russell Tomar, John Reveille, Daniel H. Solomon, Henry A. Homburger; Guidelines for Clinical Use of the Antinuclear Antibody Test and Tests for Specific Autoantibodies to Nuclear Antigens. Arch Pathol Lab Med 1 January 2000; 124 (1): 71–81. doi: https://doi.org/10.5858/2000-124-0071-GFCUOT
Subscribe to:
Posts (Atom)