After a protracted discussion on the previous post, I thought I would go down to the University of Minnesota Biomed library today and look at the drug ads in psychiatric journals at about the time Prozac came out in 1987. I was interested in the trends before and after so I picked the years 1985 to 1995. I also picked the journals the American Journal of Psychiatry, Archives of General Psychiatry (currently JAMA Psychiatry), and the Journal of Clinical Psychiatry. I was going to include JAMA and the New England Journal of Medicine. They had about the same number of ads but none of them in that year contained ads for psychiatric medications.
This kind of search is labor intensive these days. There was a time on the early days of the Internet when entire journals with all of the ads were scanned in. As a subscriber I could have run that search from home. These days, all of the ads are gone and the references are saved as text files only. In order to see historical ads - the hard copy of the original journal needs to be examined. Even then there are some problems. I encountered some bound volumes where the ads were physically removed. There were two to three bound volumes per year and additional copies of the NEJM and JAMA - I may have looked at 75 bound volumes over 4 hours.
In many ways it was a walk down memory lane. Clozaril and Haldol Decanoate ads were especially heavy in the early 1990s. There were ads for medications that I prescribed all of the time like Navane and Pamelor and ads for drugs that I seldom prescribed like Stelazine, Serzone and Luvox. There were ads for new drugs that I would prescribe once like Paxil. It was a reminder that despite all of the advertising - a lot of drugs end up never being prescribed by physicians. My reason for being there was to look for the origins of the term "chemical imbalance" in this advertising.
I decided to embark on this project because of all of the inaccuracy about the term, especially the tendency to blame psychiatrists for it. In my previous post, I attempted to point out that it is a fairly straightforward process to conclude that the human brain does not run on chemical imbalances - just based on the average scientific knowledge of physicians. On the advertising side, I was there for the first National Depression Screening Day in 1990 and that was the first time I heard the term. The event has been criticized as a venue for allowing a pharmaceutical company to showcase their product. I participated in the event for 3 years and the advertising involved was much more subtle than is found today at NAMI walks for example. But the question is whether the advertising meme "chemical imbalance" was introduced at that time. Any event that happened 30 years ago is very hard to track. As the Public Affairs Rep for my District Branch of the APA, I had a lot of files about it that I subsequently trashed. I am guessing there were also some files on disk drives that would have been helpful. This is a reconstruction without that data.
I successfully located the first Prozac ad in AJP from 1988. The graphics are all iPhone photos so there is some distortion. Chemistry is emphasized on page one as in the chemical structure, chemically unrelated to other antidepressants, distinctive chemistry, and the first highly specific and highly potent blocker of serotonin reuptake.
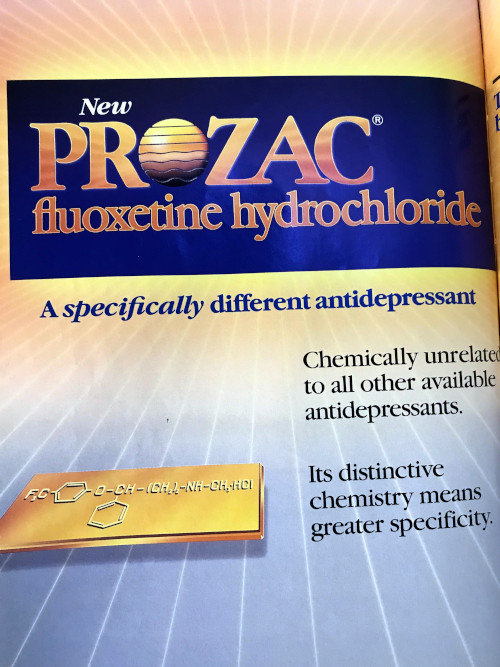

Why is this important? At the time most of the antidepressants being used were tricyclic antidepressants. They could not claim any specificity and in subsequent ads manufacturers start to compare possible side effects based on transporter monoamine protein and receptor affinities. The Prozac molecule was being hyped as being chemically unique and with a better side effect profile. As Prozac started to sell more it became a blockbuster drug for Eli Lilly and at that point the manufacturers of other new antidepressants noted and the competition heated up. There were some direct references to Prozac in the ads from competitors.
The best example is this Wellbutrin ad from AJP in 1991. Prozac is directly mentioned in the ad and reasons are given for choosing Wellbutrin over Prozac. Being non-serotonergic is one of them and this is more of a counter to Prozac advertising as being a unique first highly selective serotonergic drug. It gives little or no weight gain as a reason, but at the time I was seeing obese patients who were taking 80 mg of Prozac because their primary care physicians told them they could lose weight taking it. Of the other bullet points it seems that lack of sexual dysfunction would be the most relevant. The marketing decision in this case was a conscious decision to go after the purported serotonergic effects of Prozac rather discuss the hypothetical mechanism of Wellbutrin. The side effect of Wellbutrin that most physicians are concerned about - seizures - is in the smaller print below the bullet points.

Effexor came up with similar ads. In the late 1980s and early 1990s, synaptosome technology was invented to look at binding affinities of central nervous system medications to specific receptor sites. The quantitative aspects of these studies were generally globalized in the psychiatric literature to qualitative ballpark effects. For example a plus or minus grading system could be used ranging from no effect at a receptor (-) to a robust effect (++++). Effexor advertising used this to compare side effect profiles among the competitive antidepressants at the time.

This ad emphasizes that Effexor is "a structurally novel antidepressant and is chemically unrelated to any other available antidepressant." It shows the table with comparisons to tricyclic antidepressants (TCAs) and selective serotonin reuptake inhibitors (SSRIs) and what might be predicted based on the in vitro synaptosome data with the qualifier that the clinical significance of that data is unknown. Clinically most people are able to tolerate all three classes of medication but some will not. The differences can't be predicted on the basis of the receptor binding studies because of receptor heterogeneity and differences in drug metabolism. For example, I still prescribe TCAs. It is nortriptyline and it is the only one I have ever prescribed. At the doses I prescribe and per the table in the ad - it is as well tolerated as SSRIs and SNRIs (Effexor). The ad appeared in the AJP in April of 1994. On that basis the argument could be made that it is an appeal to the technical expertise of psychiatrists and it should contain this information. That also points to a weakness in my informal advertising study and that is a lack of ads from the non-technical consumer literature from the same period. (see supplementary on a proposal).
I have 30 additional ads from the journals but the themes are roughly the same. An emphasis on medicinal chemistry and the suggestions that some chemistry is better than others. Interestingly, in my previous post the whole point was that this is the kind of argument that would not fly based on what the average physician knows about chemistry and molecular biology. Psychiatrists should know a lot more because the evidence for and against these theories had been reviewed in the psychiatric literature 20 years before these ads came out (1974-2002) (1). And they are engaged in clinical practice and need to be skeptical of newly introduced products and claims.
What I did find so far is unequivocal evidence that the chemical imbalance meme was used to directly market antidepressants to the public. The Zoloft ad embedded at the top of this page from 2001 is the first example. The second example is this Paxil ad from the same year.
That is what I have so far. See the Supplementary below to find out what you can do to complete the story. I don't have a problem with people telling me that their doctor told them that they have a chemical imbalance and their antidepressant is supposed to treat that. I don't have a problem with people saying that their psychiatrist told them that. I do have a problem with people saying that all or even most psychiatrists say this and that psychiatrists are behind this meme.
There is an exaggerated focus on the mechanism of action of medications used for psychiatric indications. I have never heard anyone say their doctor told them about the mechanism of action of antibiotics or even their blood pressure medications. In the case of antibiotics it is clear that people demand them and they don't care what the risks or mechanisms are. This advertising campaign may have something to do with the conversion of folk psychologists to folk psychopharmacologists. A friend of mine also brought up an important aspect of this campaign that is also addressed by these manufacturers and that is legitimacy. For decades people with depression and anxiety were viewed as weak people with a questionable problem. My friend told me that these ads confirmed that she had a serious problem that needed a serious solution and that it was finally acceptable to talk about it. Say whatever you want about Big Pharma advertising but it apparently carried the message that current "Let's Talk About Mental Health" programs do - but over 15 years ago.
The attribution of an advertising meme to psychiatry and psychiatrists despite the fact it has never appeared in 30 years of psychopharmacology texts is not a trivial fact. The advertising videos posted here were viewed by tens of millions of people. I hope to get more information and still have some people to contact. With any luck I will be able to fill in the additional data between the release date of Prozac in 1987 and the ads posted here from 2001.
Please send me anything you might have from those dates.
George Dawson, MD, DFAPA
References:
1. Nathan KI, Schatzberg AF. Mood disorders. in Review of Psychiatry, vol 13. American Psychiatric Press, Washington DC(1994): p.171-184
Supplementary 1:
From the information I posted above it is clear that chemical imbalance was an advertising meme introduced during the height of competition of blockbuster antidepressant drugs. The common Wall Street definition of a blockbuster pharmaceutical is a product that generates sales of a billion dollars a year. There are two important pieces of data that would be useful to complete the story.
The first is earlier ads with the term chemical imbalance. So far, I have two from 2001, but I am certain it appeared before that. I don't have time to search all of the popular literature. If you subscribe to a magazine that has pharmaceutical advertising and keep all of the old volumes - take a look at the editions from about 1987 to 1995. If you see the term chemical imbalance please send me the image with the name and date of the periodical. Let me know if you want credit for finding the image and I will give you full credit.
If you are a current or former pharmaceutical rep or marketing person and have access to any documents or videos with the chemical imbalance phrase please send it to me with the date it was being used. If you have recollections of how it was implemented and when I can also use that information but I am most interested in clear documentation like the videos I have posted. I have no interest in vilifying the pharmaceutical industry and understand the need for marketing and advertising. I am just interested in the origins of this term and how it was implemented.
If you are an APA member and you were involved in the original National Depression Screening Day in 1990 - you may also have some information about this. Please send it to me.
Thanks!
Supplementary 2:
All of the name brand drugs/medications mentioned in this post are currently generics or are no longer manufactured. I have no affiliation with the original manufacturers or the generic drug industry.
Supplementary 3:
There are various Internet sites that attribute the term chemical imbalance to Pfizer or Lilly but they do not appear to be reliable - many appear to be antipsychiatry sites. I would like to hear from people who were there at the time and can provide the necessary proof. In those days (1986-1996) it would have been an internal memo or presentation. Send me a copy if you have it.
Supplementary 4:
I had the opportunity to discuss this issue with a corporate attorney - especially the issue of available emails and memoranda dating back to 1987. He told me that corporations hold this data only as long as the law states they needs to. For example, if the law states the data must be held for 4 years it will be held exactly that long and then everything will be shredded. If this information exists it will probably be in private hands.
Supplementary 5:
I got the expected low level feedback from a Twitter poster who thought he was making some point about this link on the Royal College of Psychiatrists web site suggesting that at least one of the causes of schizoaffective disorder was "a chemical imbalance". I guess he really thought he had made me look foolish especially with the proclamation "You aren't psychiatry - they are."
https://www.rcpsych.ac.uk/mental-health/problems-disorders/schizoaffective-disorder
In fact, I can't tell who wrote this and whether or not it is a psychiatrist. I don't know what the RCP official position is. I was happy to see that they are much more flexible than the anti-psychiatry Twitter posters I encounter. There was a feedback form that I completed and advised them to lose the "chemical imbalance" and that replacing it with "unknown etiology" was preferable. What I would like to see is an exposition of the latest theories and a suggestion that the critics actually read psychiatric literature. They would be less likely to perseverate the same criticism they have used for year after year. This poster also seemed to ignore the fact that the RCP public information was posted in 2015 - that's 14 years after the television ad posted at the top of this page. Royal College of Psychiatrists - the ball is in your court.
Supplementary 6: (added on 1/11/2020): I just learned today from an advertising expert in antidepressants that there was also a Zoloft ad from 2004 that used the term:
"While the cause is unknown, Zoloft can help. It works to correct a chemical imbalance in the brain that may be related to these symptoms."

Reference:
Cristina Hanganu-Bresch. Treat Her with Prozac: Four Decades of Direct-to-Physician Antidepressant Advertising in Drugs Media: New Perspectives on Communication, Consumption, and Consciousness (Hardback) (1st Edition) by Robert C. Macdougall (Editor), Drugs &. Media-Pasta Dura, 340 Pages, Published 2011 ISBN-10: 1-4411-1988-4 / 1441119884 ISBN-13: 978-1-4411-1988-9 / 9781441119889:








