 |
from: Insel TR, Cuthbert BN. Medicine. Brain disorders? Precisely.
Science. 2015 May1;348(6234):499-500.
|
I caught this article about the RDoC criteria for classifying mental illnesses based on various non descriptive parameters and neuroscience in the journal Science a couple of weeks ago. As any reader of this blog can attest, there is no stronger advocate for the role of neuroscience in current psychiatric practice and the future of psychiatry than me. There has been media controversy on this subject and it is always difficult to determine how much real controversy exists and how much of it is just made up for the sake of media self promotion like much of the DSM-5 controversy was. Reading through the article by Thomas Insel and Bruce Cuthbert there are statements that can be taken at face value. I think these statements are consistent with the position that clinicians in general are not very scientific and are also outright clueless in some areas. This is a bias that I have certainly heard from other scientists and it does not serve the cause of science very well, especially if the goal is to advance neuroscience and bring everyone up to speed on that discipline. Dr. Insel has presented his view that all of the trainees in the clinical neurosciences of psychiatry, neurology, and neurosurgery should rotate through a year or two of a shared neuroscience. When I first heard him present it five years ago I thought it was a great idea. In the time since and especially after getting a response from him, I think it is less clear. It would be great if every department of psychiatry had neuroscientists on staff to teach neuroscience. But they don't and there is also the problem of neuroscientists being focused on research rather than teaching. On the other hand, there are plenty of bright people in those departments who know a lot about the brain. It is a question of reconciling these two points to come up with the necessary infrastructure yet in this article the authors make it seem as if large clinical problems are not addressed and that clinicians are fumbling around with very crude assessment methods.
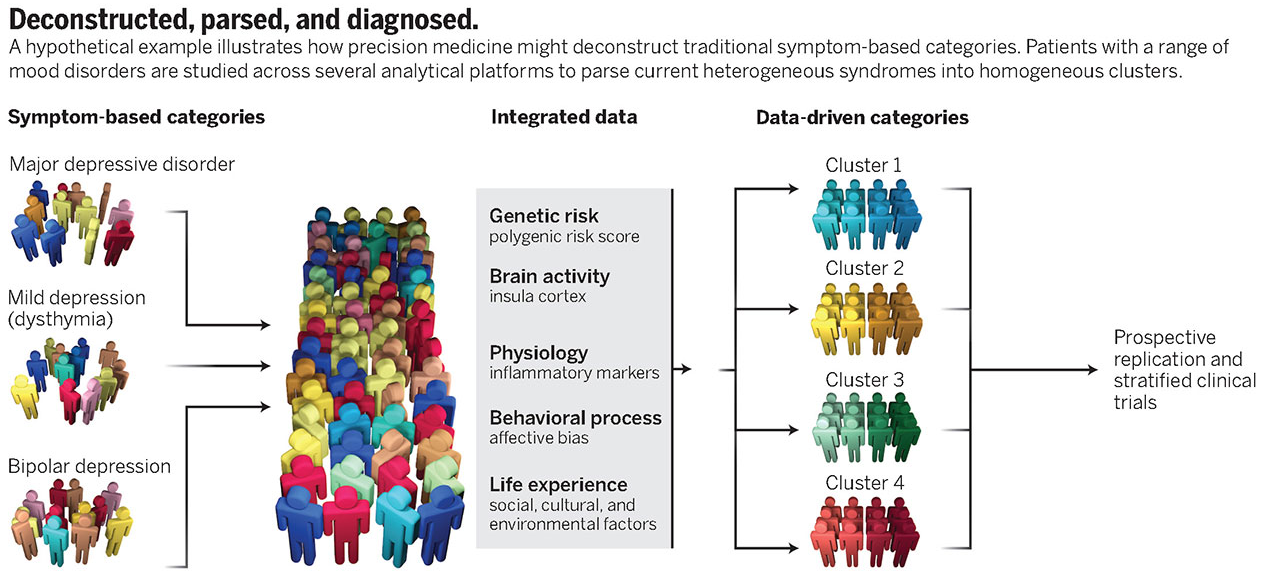
They list three articles as examples of the RDoC. The most interesting of these articles is one from the American Journal of Psychiatry that proposes that computer abstracted data from hospital notes that is converted to RDoC criteria are better predictors of hospital length of stay (LOS) than DSM criteria. Just considering that method my first impression was that there was a lot wrong with that picture. First of all, LOS data is tremendously skewed based on non-clinical practices. All it takes is hospital case managers with some success in intimidating physicians to skew the data in favor of business rather than actual medical or psychiatric discharge decisions. Second, the quality of data from inpatient settings is incredibly bad due to the toxic combination of electronic health records and government billing and coding regulations. As a reviewer, I have seen thousands of inpatient records, some of them hundreds of pages in length and I have found EHR records are notoriously poor in information content. And finally, I thought the RDoC was a new system designed to be dependent more on neuroscience than the DSM-5? How does methodology that looks at this DSM biased, sketchy clinical data result in a RDoC diagnosis? Looking at the graphic from the Science article at the top of this post, it is pretty clear that 3 out 5 data dimensions under "Integrated Data" are basically clinical data. There is a smugness displayed in the report similar to what might be seen in a rant by an antipsychiatrist: "For now clinicians might be best advised simply to be aware of the usefulness of dimensional models to capture psychopathology." and "This result should provide some reassurance to clinicians that their notes do contain relevant detail for deriving dimensional measures of illness; like Molière’s Bourgeois Gentlemen speaking prose without knowing it, clinicians may already speak some RDoC."
Really?
The average person I see has chronic insomnia and has had possible sleep terrors and nightmares in childhood along with social phobia. At some point they developed either severe anxiety or depression, but they can't recall the sequence of events and they currently have both. They typically think that they have had "manic episodes" and may have been diagnosed with bipolar disorder even though they don't know what a manic episode is. All they know is that their symptoms have persisted usually without remission for the past 10 to 15 years. Of course that is complicated by the fact that they have been using marijuana, alcohol, and opioids in excessive amounts since then, they may not have a significant family history of psychiatric and addiction problems, and they have the expected childhood adversity and adult markers of psychological trauma and abuse. Further, I know from talking to the same people in repeated initial evaluations over the years that they don't give the same history twice and rarely remember much about their medications or psychotherapy treatment. Should I use a "placeholder diagnosis" (pejorative term from reference 4) or should I assume that I am dealing with the social phobia that the patient may have had in childhood? The idea that an RDoC diagnosis is going to give me an answer to that question any better than a DSM-5 diagnosis is pure folly if you ask me. At least until we get the promised neuroscientific markers promised by the NIMH. In fact, the description of the RDoC in these articles is reminiscent of another technology that was supposed to diagnose mental illness and that was quantitative EEG or QEEG. I know quite a lot about QEEG, because I purchased a machine in the 1980s after a promising article on the technology came out in the journal Science. I researched it using highly skilled EEG techs and an expert in neurophysiology to run the protocols, and concluded the diagnoses that came from the computerized analysis of the tracing were no better than chance in terms of what patients presented with. Like RDoC diagnoses, the computerized analysis of QEEG data was highly dependent on the input of clinical data collected by the clinician. It allowed the clinician to add and subtract clinical variables and look at how the diagnosis varied.
The staff and researchers at the NIMH need to decide if a superior and critical attitude toward physicians who use current clinical approaches and are successful with them is the best one. It should be obvious from the above analysis that many of us are not as naive or as ignorant about science as they expect. My proposed solution would be a more collaborative approach including the following:
1. Recruit and train neuroscience teachers - most of them are already out there. For example much of what I teach to trainees interested in addiction and addiction medicine is neuroscience. It is also much more realistic than waiting for every department to have access to neuroscience researchers and then expecting those researchers to teach in addition to doing research. My guess is that every Psychiatry department already has faculty that teach neuroanatomy, pharmacology, brain science and neuroscience already and that most of them are not officially scientists.
2. Make the reading list available online - the article refers to over 1,000 published articles that focus on the RDoC criteria. These should be available though the National Library of Medicine web site along with other neuroscience articles of interest to psychiatrists. An added bonus would be CME activity available for self study.
3. Post a list of neuroscience modules and build on that list - In a previous post, I posted two links to neuroscience modules through the NIMH. I would put up two lists, one containing a growing list of modules and the second with a list of the neuroscience concepts that need to be illustrated. This would be useful for psychiatrists, psychiatrists in training, and medical school professors hoping to make their basic science lectures more relevant, since many clinicians still seem to have difficulty understanding how neuroscience is important in psychiatry.
4. Better graphics - make high resolution graphs that illustrate detailed brain anatomy and basic science available online for teachers. Pulling this material together is often the most difficult part of the teaching job and it requires an intensive effort to not run afoul of copyright laws. It would be easier to recruit neuroscience teachers if there are high quality teaching materials available.
5. A neuroscience teaching blog - In addition to the NIMH staff posting the references, concepts and modules, an open teaching blog should also be available. I would encourage it to be a platform for discussing concepts and how to present them to trainees. Ideally, it would be a place for active dialogue about the concepts and teaching them.
I think that all of these measures would be helpful in building an infrastructure of neuroscience teachers, neuroscience teaching, and a mechanism for the widespread dissemination of this material in residency programs and in educational programs for practicing psychiatrists. If the RDoC is in fact worthwhile, there is plenty of brainpower outside of the NIMH to figure that out.
It is the brainpower that is currently focused on coming up with solutions and resolving problems of incredible clinical complexity. And that happens every day.
I plan to send these recommendation to Director Insel and see what he thinks.
George Dawson, MD, DFAPA
1: Insel TR, Cuthbert BN. Medicine. Brain disorders? Precisely. Science. 2015 May
1;348(6234):499-500. doi: 10.1126/science.aab2358. PubMed PMID: 25931539.
2: Casey BJ, Craddock N, Cuthbert BN, Hyman SE, Lee FS, Ressler KJ. DSM-5 and RDoC: progress in psychiatry research? Nat Rev Neurosci. 2013 Nov;14(11):810-4. doi: 10.1038/nrn3621. Review. PubMed PMID: 24135697.
3: NIMH. Research Domain Criteria
4: McCoy TH, Castro VM, Rosenfield HR, Cagan A, Kohane IS, Perlis RH. A clinical perspective on the relevance of research domain criteria in electronic health records. Am J Psychiatry. 2015 Apr;172(4):316-20. doi: 10.1176/appi.ajp.2014.14091177. PubMed PMID: 25827030.
2: Casey BJ, Craddock N, Cuthbert BN, Hyman SE, Lee FS, Ressler KJ. DSM-5 and RDoC: progress in psychiatry research? Nat Rev Neurosci. 2013 Nov;14(11):810-4. doi: 10.1038/nrn3621. Review. PubMed PMID: 24135697.
3: NIMH. Research Domain Criteria
4: McCoy TH, Castro VM, Rosenfield HR, Cagan A, Kohane IS, Perlis RH. A clinical perspective on the relevance of research domain criteria in electronic health records. Am J Psychiatry. 2015 Apr;172(4):316-20. doi: 10.1176/appi.ajp.2014.14091177. PubMed PMID: 25827030.
Supplementary 1:
The above figure is licensed through the American Association for the Advancement of Science - license number 3637270124183.







