Another clip that goes a long way toward explaining why we watch sports, go to concerts, read good books:
https://www.youtube.com/watch?v=TZeaZ3rZumg
In this clip Louden Swain, a high school wrestler preparing for the match of his career goes to see why Elmo the cook who he works with took the evening off of work to go to his wrestling match. Elmo's soliloquy here about sports still strikes me as the best single reason why I watch sports.
I have never seen it studied, but it seems that there are several reason for why sports play a central role in society. The social elements are apparent and many people see themselves as a larger community tied to a particular team. I used to be New York Yankee fan, despite the fact that I did not set foot in New York City (or the state of New York) until I was about 26 years old. My father was a Yankee fan and so was I, so identification is important. Somewhere in my late 20's I realized that a certain team winning was no longer important. I started watching "This Week in Baseball" just to watch all of the best plays. I tuned in to see Nolan Ryan pitch. I watched the Tour de France and the Olympics to see the best athletes in the world compete. I can still remember my excitement as I watched Johann Olav Koss in the 1,500, 5,000, and 10,000 meter events at Lillehammer. It was the first time that they had a motorized camera following the speedskaters. We learned that he had some last minute technical problems with the blade angle on his skates but Koss's form was perfect. I was ecstatic. I had become Elmo.
I have never seen a study that looked at the percentages of people who watch sports for the purposes of seeing a certain team win versus those who are looking for the best possible human performances. But for the later - there is no better explanation than Elmo's soliloquy in this clip.
George Dawson, MD. DFAPA
Saturday, May 5, 2012
Wednesday, May 2, 2012
A Consciousness Based Model
One of the criticisms of psychiatric treatment in particular
drug therapies is that essentially nothing is known about psychopathology,
neurobiology, or human genetics and therefore claiming that drug therapy is
treating a pathological state is erroneous (1). "Chemical imbalance" can
be used as a red herring along the way and I will try to address that in a
later post. In that post, I also hope to
address the issue of disease states and whether or not they need to be strictly
measurable.
For now, I want to discuss a model that I have used in
clinical practice for the past decade that addresses both the issues of
recovery and whether or not the drug altered state or treating an underlying
pathological state is really the issue. Let me start by saying I think it is
irrelevant for the purposes of treatment. I am first and foremost a clinical
psychiatrist and not a researcher and my priority is at all times patient care.
My
goal is to treat alterations in a person’s conscious state and restore their
level of functioning with medications and/or psychotherapy that have been shown to work. My goal is also not to introduce any new
problems such as sedation, mood changes, rage, perceptual problems, ataxia, false
memories, vertigo, or any number of subjective changes commonly seen as
"side effects".
I found that the best way to proceed is to have an explicit
discussion of the person’s conscious state and whether it has undergone any
transformation associated with the reasons why they are seeing me. I focus on the typical stream of consciousness
that occurs each and every day and how it may have changed over the previous
weeks or months or years. I ask about
whether or not getting back to that conscious state is a reasonable goal. I point out that the phenomenology associated
with a person's cognitive and emotional changes (2) can be followed in at least two
dimensions at once - the psychopathological and the normal.
There are obviously problems with my approach. The
subjective assessment of a psychopathological state and the subjective
assessment of the baseline conscious state are difficult to do and they take
time. There are a large number of
markers of psychopathological states but not so many for normal conscious
states. I often end up discussing broad
outlines that include the typical stream of consciousness, fantasies,
daydreams, defense mechanisms, distracting thoughts and typical thought patterns in certain situations such as driving
into work each day. I also ask about
a global assessment and whether at any point during treatment the person feels
like their original conscious state has been restored. It adds
another goal to treatment that is focused on restoring the self rather than
just treating symptoms.
George Dawson, MD, DFAPA
1: Moncrieff J, Cohen D. How do
psychiatric drugs work? BMJ. 2009
May 29;338:b1963.
2: Andreasen NC. DSM and the death
of phenomenology in america: an example of unintended consequences.
Schizophr Bull. 2007 Jan;33(1):108-12. Epub 2006 Dec 7.
Sunday, April 29, 2012
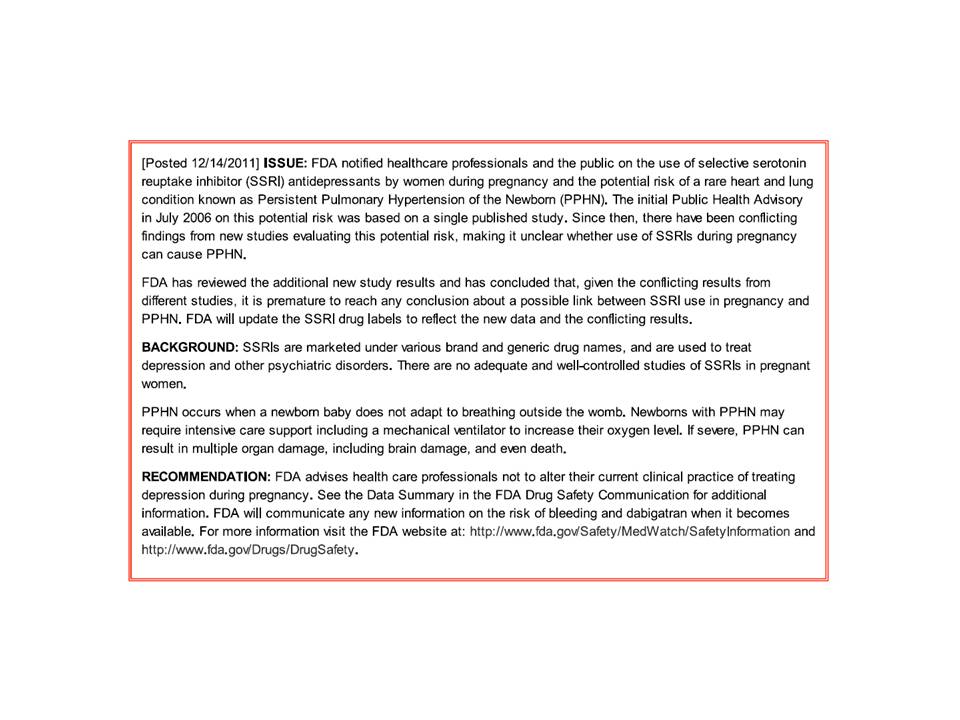
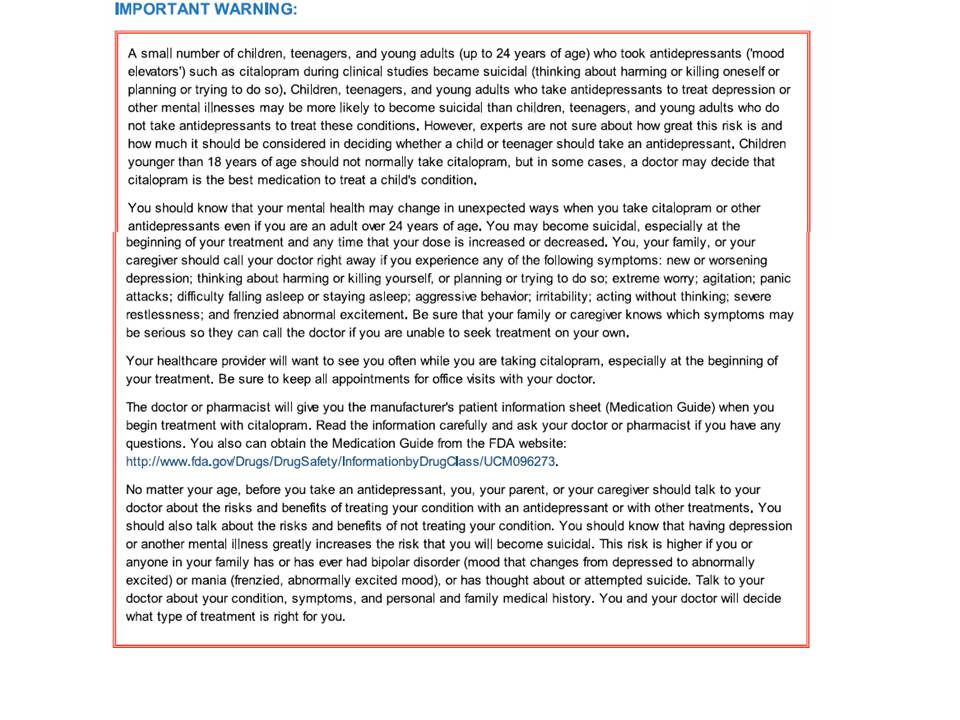
Does the FDA discriminate against antidepressants?
The FDA came out with a new warning on citalopram on 3/28/2012. The main point of the warning is that citalopram may lead to electrocardiogram changes that can be associated with an abnormal heart rhythm or arrhythmia that is potentially fatal. The specific change is prolongation of the QTc interval or the interval that correlates with the total duration of ventricular activation and recovery.
Citalopram is a widely used antidepressant medication and it widely used for three reasons. It is not likely to have a lot of interactions with other drugs. Citalopram figured prominently in the STAR*D algorithm from the largest study done on enhancing antidepressant effectiveness. A third reason is that it is a generic medication and it is very inexpensive. Psychiatrists have broad experience with the drug and the general experience is that it is well tolerated with little toxicity.
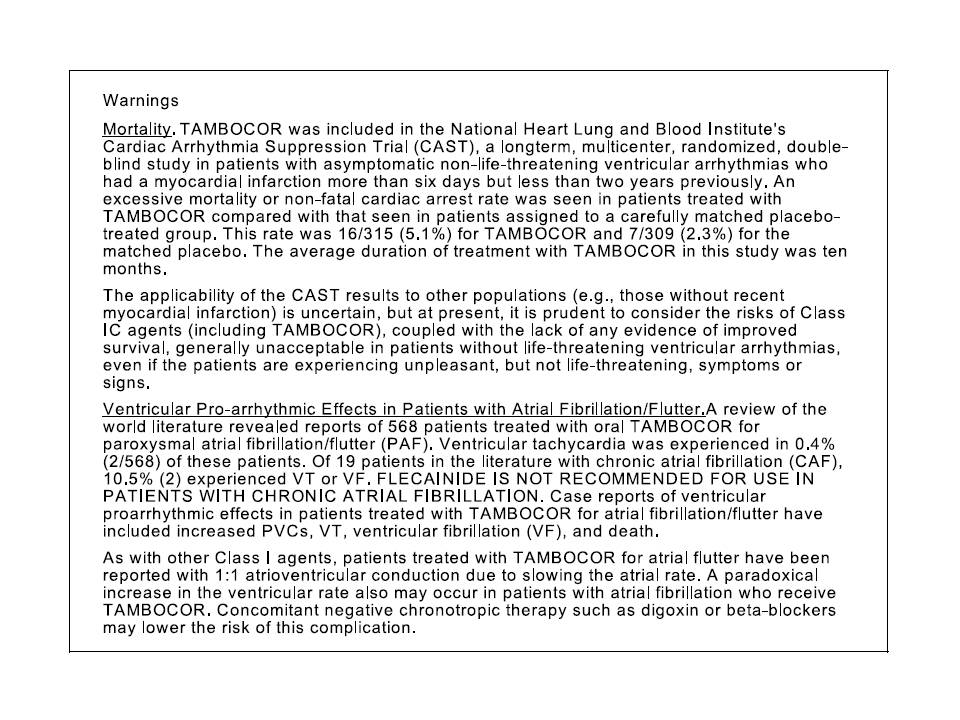
Flecainide is a Type IC antiarrhythmic agent indicated for the prevention of paroxysmal atrial fibrillation (AF), paroxysmal supraventricular tachycardia (PSVT), and the prevention of life-threatening ventricular arrhythmias like sustained ventricular tachycardia. The FDA warnings on the drug include proarrhytmic effects and excess mortality. The excess mortality was directly observed in a clinical trial done to suppress ventricular arrhythmias.
The black box warnings for each drug listed below are directly from Medline:
Looking at the safety concerns for both medications - important differences emerge. First, the FDA recommends maximum doses for the citalopram not just for the a maximum dose for adults but in specific conditions including aging. Searching the FDA web site shows exactly 25 references for safety concerns of flecainide and none of them contain that level of information. Second, the citalopram warning shows a table of QTc interval changes by dose for both citalopram and escitalopram. There is no information in FDA documents (that I could find) for flecainide even though it is widely accepted that flecainide causes dose related changes in not just the QTc interval but also the QRS and PR intervals along with a host of additional effects on cardiac pacemakers and conduction. The overall tone of the release is that citalopram is a potentially cardiotoxic drug. Third, the ECG monitoring recommendations are not internally consistent. The absolute cut off of a QTc interval of 500 ms is highly unlikely - even in cases where the patient is taking 60 mg per day or more of citalopram. It is also unlikely that the QTc intervals in the citalopram warning will lead to a QTc interval of greater than 500 ms. This will result in tens of thousands of ECGs done because that is the only way that the QTc interval can be determined.
The black box warnings and the recently issued warning all considered, serious questions are raised relative to drugs with known cardiotoxicity and the whole issue of QTc warnings in all psychiatric drugs. Certainly nobody wants a rare severe complication as a result of a prescription medication but can it really be avoided? What good would ECG screening do? There have not been any trials to address that issue of whether all patients taking citalopram need baseline ECGs. All the patients taking flecainide have probably had multiple ECGs done that indicate a possible need for treatment but there is little guidance on the ECG issue. In many patients taking flecainide, patients get serial ECGs and they do exercise stress tests to rule out proarrhythmic effects. Are the same precautions needed for patients on citalopram?
Are the thresholds for treatment different given the fact that flecainide caused increased mortality during clinical trials and citalopram did not? There would be an argument that flecainide is used to treat life-threatening arrhythmias, but the other indication is for prevention of atrial fibrillation and atrial fibrillation is not a life threatening arrhythmia. With regard to the seriousness of the diagnosis, major depression carries a lifetime mortality of 10%. Finally, where is the table on the relationship between flecainide dose and QTc prolongation like we see for both citalopram and escitalopram? Is it possible that flecainide has more of an effect throughout the dosage range than citalopram?
These are serious questions given that I have already established that there is a significant bias in the media against psychiatry, psychiatrists and psychiatric medications. The most recent FDA warning has created a lot of anxiety for psychiatrists and any patient taking citalopram. The majority of those patients are being seen by primary care physicians.
If citalopram is that cardiotoxic, let's see the evidence and let's see how it compares to a medication with known cardiotoxicity. Let's have the same level of warning for both medications and some concrete ideas about what needs to be done to manage that risk.
George Dawson, MD, DFAPA
Friday, April 20, 2012
The $40 Call
One of the local HMOs has been heavily advertising their nurse
practitioner diagnostic line. It caught my attention because the radio ad was
focused on wood tick season, and it suggested the diagnosis and treatment of Lyme disease could be rapidly made over the phone and that it could require
e-mailing in a picture of the rash or tick.
I used to teach a course in medical diagnostics and
diagnostic reasoning and one of the examples I used in that course involved
expert diagnosis of rashes from photographs.
An important part of medical diagnostics is pattern recognition. There
is probably no better example than the diagnosis of rashes and it should not
come as a surprise that experts in rashes or dermatologists do a much better than
physicians who are not experts. That is true both in terms of making the actual
diagnosis and in the total amount of time that it takes to arrive at that
diagnosis.
When I heard about this new service to diagnose Lyme disease
based on photographs I went to Medline to see if I could find anything written
about it. Managed care organizations and HMOs frequently advertise the fact
that they are evidence-based organizations. I really cannot find any studies
done on using the Internet or telephone consultation for the diagnosis of
rashes or Lyme disease.
I think that this new service has implications for how the
business models are impacting the practice of medicine. With all the talk about
transparency it would be useful for the public to know the false positive and
false negative rates for this diagnostic service. That certainly would be
consistent with the literature on the misdiagnosis of Lyme disease.
From a purely economic perspective, it is interesting that
the cash charge for this service is on par with the most common cash charge for
seeing a psychiatrist in person. As I have previously posted, there is a
wide range for the psychiatric charge and it is conceivable that this
telephone service generates considerably more cash than a psychiatrist does
sitting in a clinic, seeing patients, and doing all of the associated
administrative work.
The next logical step for this telephone service is to have
patient's complete a number of rating scales and be treated for depression.
Whether it is Lyme disease or depression the diagnosticians with the greatest
pattern matching and pattern completion capabilities are taken out of the loop.
George Dawson, MD, DFAPA
Saturday, April 14, 2012
Health Care Complexity, Politicians, and Judges
There is so much wrong with the Affordable Care Act it is
difficult to know where to start. According to a recent article in JAMA, I
learned that Accountable Care Organizations (ACOs) are charged with improving
the quality of care for Medicare patients at less cost. Any psychiatrist in the
country who has witnessed the decimation of mental health care justified by
that same rhetoric should be skeptical.
So far the government has been again engaged in a highly
coordinated effort to get the ACO initiative up and running. On October 20,
2011 the final rules for ACOs were released and on that same day the Federal
Trade Commission and Department of Justice provided guidelines to address the
antitrust issues of ACOs. The JAMA
article discusses five major issues related to the creation of ACO's many of
which are unrealistic. As an example the antitrust guidelines suggest that ACOs
that have a less than 30% market share are "highly unlikely to raise
antitrust concerns". In that
landscape, the government expects that ACO's will develop and use quality
measures, avoid exclusive relationships with hospitals and specialists, avoid cost
shifting via the leverage of large physician groups to private payers, and be
monitored to avoid gaming the risk-adjustment scheme. All of these dimensions
are highly problematic.
The most problematic aspect of the Affordable Care Act is
the same problem that every major piece of legislation in the United States has
and that is that nobody reads it. I have seen quotes on how large the actual
bill is ranging from 1000 pages to 2700 pages.
I first became aware of the fact that hardly anyone in Congress reads
large bills in 2003. At that time I was following the progress of HR 1
(The Medicare Prescription Drug Bill). I
was watching C-SPAN and Sen. Harkin commented that the 1000 page bill was
delivered to members of Congress on Thursday morning so that they could debate
it on the weekend and vote on Monday morning. He was the first of many senators
to acknowledge the fact that nobody would ever read the bill.
At the time I thought that disclosure was astounding. Here
we have members of Congress whose full-time job is to design legislation and
they are not actually reading and debating a bill that regulates a huge part of
the economy and most people's healthcare. I won't even go into the fact that
the pharmaceutical lobby was so satisfied with the final result that most of
them left town on Friday.
The Affordable Care Act provides us with a new insight into
how our government operates. In this case the constitutionality of the bill is
also being debated and that was presented to the Supreme Court about two weeks
ago. In the Wall Street Journal article it is official that Supreme Court justices are no more
likely to read the bill than members of Congress. Justice Scalia is quoted: "You really want us to go through these 2,700 pages? And do you really expect the court to do that? Or do you expect us to give this function to our law clerks?" We have a check and balance
system set up where the check and balance is as defective as the original
process.
The overall process here illustrates why it was doomed from
the start. The Affordable Care Act is a highly experimental piece of
legislation at best. In order for it to function as advertised many unlikely
events will need to occur. That would seem obvious to any intelligent person
reading the bill but as we have determined there are no members of Congress and
no justices in the Supreme Court that will actually do that.
George Dawson, MD, DFAPA
Wall Street Journal. "Complexity is Bad for Your Health" April 8, 2012.
Dawson G. Medicare Drug Bill #1, #2, #3 Three real time posts on my observations on the Medicare Prescription Drug Bill in 2003.
Schleffer RM, Shortell SM, Wilensky GR. Accountable
Care Organizations and Antitrust: Restructuring the Health Care
Market. JAMA. 2012;307(14):1493-1494.
Monday, April 9, 2012
The Lancet has it about 40% right
The Critical Psychiatry blog listed a brief editorial in the Lancet commenting on the current state of affairs in psychiatry. The commentary describes psychiatry's current "identity crisis" as an international problem and cites recent comments by the American Psychiatric Association and the Royal College of Psychiatrists suggesting that psychiatry is not "scientific" enough, that it does not have a central role in medicine, that the image of psychiatry with other professionals is negative, and that the therapeutic interventions are weak. The conclusory statement is: “But more fundamental still, it is time for the specialty to stop devaluing itself because of its chequered history of mental asylums and pseudo-science, and to realign itself as a key biomedical specialty at the heart of mental health.”
The Lancet has it right in concluding that psychiatry has a long history of self-flagellation that continues right up until present times. The Lancet is also correct in concluding that the image of psychiatry is negative, and that was well-documented in the journal Psychiatric Treatment showing that press coverage for psychiatry is four times as negative as any other specialty. The remarks about the science of psychiatry, the lack of a central role in medicine, and weak therapeutic interventions miss the mark entirely. In fact, I think the only way an editor can lump all of those negatives together is the uncritical acceptance that all of the negatives about psychiatry must be true.
What the critics of psychiatry can never explain away is the fact that psychiatric treatment is effective. I have personally gone to work every day for over 20 years confident that I have been doing far more good than harm. When you are doing the same work for a span of decades rather than the time it takes someone to do a clinical trial and you are personally responsible to your patient and their family you need to realize that you are effective. If I did not think I was effective and doing a reasonable job for people I would have quit a long time ago. I also work with hundreds of competent psychiatrists in my home state where being competent is the rule not the exception.
My personal sense of effectiveness is built on decades of watching people suffer. That happened before I was a psychiatrist. Many of those people were my own family members and neighbors with severe problems who did not have access to psychiatrists. They were treated by generalists and the treatment did not go well. In many cases it was worse than no treatment at all. When I was growing up, it was also a fairly common practice for counties to sequester people with mental illness at subpar facilities that were designed for containment. In some cases that meant that people were placed in facilities that were also tuberculosis sanatoriums or “poor farms” for the indigent. I think that many of us in the mental health field got into it to compensate for the deficiencies of the past. Much of that “chequered” past has nothing to do with psychiatry at all.
Although the Lancet associates psychiatry with asylums it leaves out the fact that psychiatry invented the paradigm to care for people with severe mental illnesses in the community. That was the direct product of psychiatrists and their collaborators realizing that state-funded institutional care was completely inadequate. Psychiatry moved people out of asylums on a massive scale and helps them stay out. At this time many of these programs have been in place for over 30 years. These same programs are actively working on the health problems of the people that they serve.
The scientific basis of psychiatry has exploded in the past two decades. The criticism of the “lack” of science in the field always astounds me. The criticism often seems to flow from the lack of understanding of the process of science and how the scientific accomplishments within psychiatry are on par with other fields of science. It also seems to ignore the fact that many prominent scientists like Kandel, Snyder and others are psychiatrists.
The idea that psychiatrists are ineffective seems to flow from the same biases. Details about the effectiveness of primary care physicians are usually left out of that argument. It is well known that 30-50% of complaints presenting to general medical and specialty outpatient clinics have no medical explanation even after extensive investigation. Other studies have shown that primary care physicians deliver error free care in uncomplicated situations 73% of the time and in complex situations 9% of the time. It is really not possible for psychiatry to be worse than that and yet there are no movements critical of other specialities and those are specialities that generally have far more toxic treatments.
So we are left with an abundance of critics. The critics all have various motivations but one thing is clear and that is at least part of their agenda is not to recognize the fact that psychiatrists are currently effective, care about their patients, and that their clinical practice really is not removed from the rest of medicine. In order to recruit more psychiatrists, the best thing to do is expose students to psychiatrists working with patients and to follow those patients while they recover. It might be useful to expose them to the biases against psychiatry and why a lot of the criticism does not match reality. The fundamental work for many psychiatrists is to stop devaluing themselves, but it also requires recognition that much of that devaluation occurs due to the uncritical internalization of criticism that is far from the reality of clinical practice.
George Dawson, MD, DFAPA
Friday, April 6, 2012
Let's get rid of worthless documentation
I just became aware of this article by Lucy Hornstein, MD on modifying the
current documentation process and found it to be quite exciting
because I have had very similar thoughts for some time:
I may be a fellow dinosaur, but I could not agree
more. The vast majority of documentation especially in the EMR is
worthless largely because of the proliferation of stereotypical documentation
to fit business and government requirements. The businesses wanted to
slow us down at least until they figured out that they could literally
reimburse us for whatever they wanted irrespective of the billing code or
note. The politicians want all the bullet points because of the erroneous
notion that coders can actually read a note and objectively decide on the correct code (they
can't) and therefore they can fight fraud.
In the meantime, vast areas of hard drive space
are occupied with worthless data because of these notes and the trees die
anyway because requesting the information results in an EMR driven
telephone book sized tome
with very little information (if any) on each page.
The only thing worse is the EMR driven initiative to
rapidly assemble a massive note from existing data using smart text and a few
key strokes. I was on a committee once where we reviewed 10-16 page daily
progress notes compiled in various fonts. The majority of each note was
already listed in the record.
I can recall working on a very busy neurosurgical
service where we saw 30 patients a day (6-10 in the NICU) and did all the
documentation in 2 - 3 hours before going to the OR. All of the progress
notes for the entire hospitalization generally fit on one page.
I have been thinking about Dr. Hornstein's approach
for some time and have come to the same conclusion. The current notes and
coding system is basically driven by paranoia and not patient care. Any
EMR system worth its salt should be able to display all of the daily relevant
data and provide a check box so there is documentation that the
attending reviewed it all and signed off instead of the physician doubling as
scribe and displaying it all (after a flurry of mouse clicks) in a massive note. The actual note needs to
reflect the fact that an intelligent life form visited the patient and there
is a thoughtful analysis and plan.
That doesn't happen by filling up templates in an electronic medical record.
That doesn't happen by filling up templates in an electronic medical record.
George Dawson, MD, DFAPA
Subscribe to:
Posts (Atom)