On September 4, I started to feel typical symptoms of a flu-like
illness. I have been a student of flu-like illnesses for at least the past 15
years. Some may say that I am obsessed with flu-like illnesses. By definition
these illnesses start out as acute upper respiratory infections but also lead
to systemic symptoms like malaise, weakness, and muscle pains or myalgias. In
some cases, the symptoms can build to a disabling intensity. About five years
ago I developed a flu-like illness after returning from Alaska that led to an
exacerbation of asthma. I had not taken any asthma medications for 20 years but
have been on those medications ever since. Researching that area suggested that
flu-like illness was probably a rhinovirus. Some researchers think that
rhinovirus is one of the main precipitants of asthma. Rhinovirus also happens
to be a common circulating respiratory virus along with about 20 others that
cause respiratory infections every year.
There are several non-COVID-19 coronaviruses in this group.
There were definite early signs even before the first
respiratory symptoms. I have a fairly set exercise routine that I do every week
and I noticed that my baseline heart rate (54 bpm) and blood pressure (105-110 mm
Hg systolic) were increased and my exercise capacity was decreased by about
40%. That occurred about 48 hours before the onset of symptoms. As the symptoms
increased my first thought was that I needed to get tested for coronavirus.
That took an additional four days. It wasn’t from a lack of trying, but more a lack
of resources going into the weekend. That delay highlights a significant
weakness in the American healthcare system. I self-quarantined during that time
but there are a lot of people who would need to see the test result before they
could. I did get positive test on day
seven, I canceled the rest of the day at work and have been home recovering
ever since.
The overall course of the illness has been very similar to
a moderate case of influenza with the exception that I did not get a fever. It
measured every day in the normal range. I also did not get shortness of
breath. Having the risk factors of
asthma and old age, I was fairly anxious about any shortness of breath as a
symptom. My symptoms are basically as graphed with a few exceptions of what I
would refer to as atypical symptoms. The first one would be feeling flushed
or like the skin temperature is elevated. That has been a fairly consistent
feature that I have not seen mentioned anywhere. My skin was always cool to the
touch and not moist. Another atypical symptom is laryngitis. I have observed that in several COVID-19
patients in the media. It can be fairly
limiting if you have to talk all day at work like I do. The third atypical
symptom was viscous mucus in the nose and throat. It was not abundant
but difficult to clear and never reached the volumes typically seen in
bronchitis.
One of the questions that I have been asked is: “How does a
guy as careful as you end up catching COVID-19?” It turns out that is an excellent question.
As noted elsewhere on this blog I have essentially self-quarantined at home
since the end of March or the start of the pandemic. I have had limited contact
with people. I do not go into stores, supermarkets, coffee shops, or any public
space. I pick up groceries ordered online and then collect them from a site
where a masked attendant loads them into the back of my SUV. All of my clinical work, continuing education,
and professional meetings are done online.
I prepared a timeline of all contacts in or around my home for the
previous 19 days (click to enlarge).

From the summary, of the 18 total contacts I had direct
contact with 6, only 4 of them about 6 days prior to the onset of
symptoms. All 4 of those contacts were
wearing masks and none have tested positive for COVID-19. My wife had contact with the other 12 and 9
of them were socially distanced or masked.
Only the electrician and three of the appliance repair/installers were
not but they were socially distanced. In
addition, we made an effort to air out the house when they were there and after
the left. There was a total of 5
tradesmen in the house. They were all there for an average of about 1
hour. I greeted one of them at a
distance of about 12 feet and he was not wearing a mask. According to a recent hierarchy
of transmission risk, I had no high-risk contacts for transmission (3).
My wife on the other hand was in a couple of higher risk
scenarios (but not much higher). As an
extrovert, she was also out talking with people every day and exercising with
several of her health club friends at their homes. She did however test
negative for COVID-19 on the exact same test that I took. There are various
estimates that 20-40% of COVID-19 infections result in asymptomatic carriers.
It may be possible that she was a carrier and subsequently cleared the virus so
that no viral RNA was detected on the nasal swab. We are both currently trying to get antibody
testing to COVID-19. It will confirm that I have short term immunity and
possibly that my wife was an asymptomatic carrier.
When I did find out that I tested positive, I
self-quarantined in the house pending my wife’s test and have been quarantined
ever since. The health plan
recommendation is to wait for day 14 and if asymptomatic at that point, the
self-quarantine can end. My wife is using the same date to end her quarantine
and remained asymptomatic. We have the
luxury of having a large enough house where we can occupy separate areas and
have separate bathrooms that are exhausted to the outside of the house. I also kept an electronic air filter with a
UVC germicidal light at the entrance to my office and between us in any public
areas. Several questions arise from this
experience including:
1. Why were my
symptoms so mild (relatively speaking)?
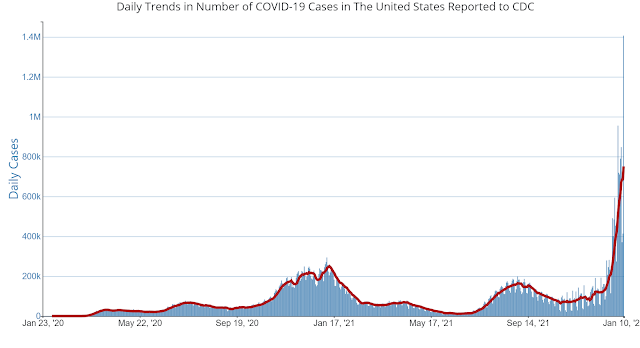
Considering the actual statistics of the pandemic in the
United States – my outcome is not that surprising. About 1 in 34 cases have died and that number
increases to 1 in 13 in my age range and 1 in 5 in the next highest age
decile. At the time of this posting there
have been 197,000 deaths and 6.7 million cases.
There is a lot of comparison with influenza, but at this time there
should be no mistake that while influenza typically generates more cases and
more hospitalizations – there has only been one
year where influenza mortality exceeded current SARS-CoV-2 mortality and
that was the pandemic of 1918.
The second consideration are the physical parameters of the
environment. Assuming that my wife is not an asymptomatic carrier, the only
time I was at a distance of less than 4 meters I was wearing a mask and so were
the people I was in proximity to. The
contact lasted less than 10 minutes. And not a lot was said. We know that
masks, distancing, and dilution in outdoor air probably works be reducing the
concentration of airborne viral particles.
With that reduced concentration, any inhaled inoculum will be less
resulting in a less severe infection. The estimated number of viral particles necessary to precipitate a case of COVID-19 is about 280 particles. That is 2-3 orders of magnitude higher than more virulent and lethal viruses like smallpox.
A few other lifestyle considerations. I eat a high-protein,
high fiber, high whole grain, and low fat/low sugar diet. I try to maintain a healthy weight. I drink a lot of fluids every day. I have been doing that for at least 30 years on
the advice of a rheumatologist in order to maximize uric acid secretion and
decrease the risk of gout attacks (I am an undersecretor of uric acid and had
my first gout attack in medical school). Anyone reading this should drink a lot
of fluid only based on their physician’s advice. The only relevant factor in this paragraph in
surviving the virus is probably maintaining a healthy weight and a good diet. I was able to maintain my usual fluid intake
during the course of this illness.
I take Vitamin D every day because my levels are typically
marginal. I take famotidine daily to
prevent anaphylactic reactions. I only take it because the original H-2 antagonist
recommended by my allergist (ranitidine) was taken off the market because of
contamination in the manufacturing process. There has been some suggestion that
famotidine is useful in the prevention or treatment of COVID-19 and for a while
it nearly disappeared off the generic market.
I am not aware of any randomized clinical trial (RCT) results of famotidine
and it has been demonstrated to not have any direct antiviral effect in vitro. There is current speculation that in
combination with H-1 antagonists that it may reduce histamine associated cytokine
effects (13). At this point I would not consider it to be too relevant.
Exercise is a big part of my life and has been for the past
30 years. I typically exercise vigorously for 90 to 120 minutes per day. Recent research (11,12) suggests that people
who exercise vigorously into old age have better acute adaptive immunity (T-cell
response) due to a better thymic environment.
One of the purported mechanisms is IL-7 production by skeletal muscle. IL-15 is also an exercise responsive
interleukin that enhances T-cell survival.
The net effect of these changes in the older person who exercises
vigorously has a greater input of thymocyte progenitor cells and an enhanced output
of CD4 and CD8 cells that are recent thymic emigrants (RTE). Both of these
cells populations are critical for the acute adaptive response to novel viruses. If I had to speculate about the lifestyle
factors that are important it would probably be the effects of exercise, diet,
not smoking and no alcohol intake on immunity and pulmonary function.
2. Why is there such
heterogeneity in responses?
The host determinants of response are not well
characterized at this point- other than the suggestion that previous exposure to
common circulating coronaviruses could possibly lead to an enhanced antibody
effect and either apparent asymptomatic carrier status or a less severe case as
an adult. Is it possible that the severe
respiratory infection that I got in January was a coronavirus that was not
SARS-CoV-2 and that it conferred some immunity?
This is one of the theories about why children are less affected by
COVID-19 than adults – they tend to get more respiratory virus infections per
year. Human coronaviruses and rhinoviruses are generally considered to cause up
to 50% of common cold infections per year (10).
The Minnesota Influenza Incidence Surveillance Project, (MIISP) 3 of the
4 normally circulating
human Coronaviruses – NL63, HKU1, and 229E (not OC43) since last September.
Although these coronaviruses are now considered all part of the collection of
common cold viruses they have been fairly recent discoveries with NL63
discovered in 2004 (7) and HKU1 discovered in 2005 (8). The common coronaviruses have considerable RNA
sequence homology with SARS-CoV-2 suggesting cross immunity can exist (9). For example, pre-existing T-cell immunity in
blood donors to SARS-CoV-2 is documented and is thought to be due to exposure
to beta-coronaviruses that are in circulation (4). But there is also evidence suggesting that pre-existing coronavirus immunity is not effective with SARS-CoV-2 (15).
One the genetic side, there are essentially no data at this
point about genetic factors that favor successful recovery from the pandemic
virus (click to enlarge).
3. Given the
exposures – is it possible that some other exposure (packaging, mail, aerosols
from washing packing or mail) is more important than suggested by conventional
wisdom?
Even though handwashing and washing of frequently touched
surfaces is a top recommendation the current opinion is that transmission is
unlikely from either groceries or mail based on studies that look at virus
survival on different materials over time.
To me that is somewhat inconsistent with the hand washing advice. The original theory was that a person could
touch a contaminated surface, touch their face, and then end up with the
infection through mucus membranes.
Groceries and the mail seem to be designated as infrequently touched
surfaces relatively free from contamination.
An additional question for consideration is whether aerosols generated
in washing the surfaces of groceries can transmit. SARS-CoV-2. I use a UV sanitizer for mail and any objects
the size of a large book or smaller. That method has limitations in terms of
how accessible the surfaces of any contaminated object are.
One final critical consideration is the person you are in
quarantine with. Do they share your goals and risk tolerance or not? In my particular case, I am not risk tolerant
at all if the risk is contracting a virus that has a 1 in 13 chance of killing
me. The prior probability of an adverse
outcome is higher due to me having asthma, but the exact numbers are probably
not known at this time. I would happily remain at home, not get a haircut (I
have not), and just go out for groceries and necessary medical care. My wife on the other hand is very social, and
has maintained an active schedule with her friends and associates over the
entire pandemic. She spends her days
exercising, socializing, and attending limited activities with friends. She is distanced and wears a mask when
necessary. Despite our ability to pick up groceries without having to enter a
store she will spontaneously stop at these stores, put a mask on, and pick up a
few items. This difference in approaches to the pandemic does create some
tension.
Whether our different approaches produced predictable
outcomes or not is up in the air at this point.
She was just approved for antibody testing and I still have to get
approval at an appointment next week. All we know is that I was positive for
SARS-CoV-2 on a PCR test and she was not. That leaves either airborne
transmission, contaminated surfaces, or aerosols from washing contaminated
services.
Getting through this does provide a sense of relief. Even though immunity to this virus does not
seem to be permanent at this point I am very grateful to have made it through
these two weeks. My boss sent me an
email and asked what that sense of relief was like and I told him:
“It feels like I dodged a bullet.”
And it does…..
George Dawson, MD, DFAPA
References:
1: Stephens DS, McElrath MJ. COVID-19 and the Path
to Immunity. JAMA. Published
online September 11, 2020. doi:10.1001/jama.2020.16656
2: Gandhi M, Beyrer C, Goosby E. Masks Do More
Than Protect Others During COVID-19: Reducing the Inoculum of SARS-CoV-2 to
Protect the Wearer [published online ahead of print, 2020 Jul 31]. J
Gen Intern Med. 2020;1-4. doi:10.1007/s11606-020-06067-8
3: Jones Nicholas
R, Qureshi Zeshan U, Temple Robert
J, Larwood Jessica P
J, Greenhalgh Trisha, Bourouiba Lydia et al. Two
metres or one: what is the evidence for physical distancing in COVID-19? BMJ 2020; 370 :m3223
Link
4: Stephens DS,
McElrath MJ. COVID-19 and the Path to Immunity. JAMA. Published
online September 11, 2020. doi:10.1001/jama.2020.16656 Link
5: Fischer EP,
Fischer MC, Grass D, Henrion I, Warren WS, Westman E. Low-cost measurement of
face mask efficacy for filtering expelled droplets during speech. Sci
Adv. 2020;6(36):eabd3083. Published 2020 Sep 2. doi:10.1126/sciadv.abd3083 Link
6: Bar-On YM,
Flamholz A, Phillips R, Milo R. SARS-CoV-2 (COVID-19) by the numbers. Elife.
2020 Apr 2;9:e57309. doi: 10.7554/eLife.57309. PMID: 32228860.
7: Fouchier RA,
Hartwig NG, Bestebroer TM, Niemeyer B, de Jong JC, Simon JH, Osterhaus AD. A
previously undescribed coronavirus associated with respiratory disease in
humans. Proc Natl Acad Sci U S A. 2004 Apr 20;101(16):6212-6. doi:
10.1073/pnas.0400762101. Epub 2004 Apr 8. PMID: 15073334; PMCID: PMC395948.
8: Woo PC, Lau SK,
Chu CM, Chan KH, Tsoi HW, Huang Y, Wong BH, Poon RW, Cai JJ, Luk WK, Poon LL,
Wong SS, Guan Y, Peiris JS, Yuen KY. Characterization and complete genome
sequence of a novel coronavirus, coronavirus HKU1, from patients with
pneumonia. J Virol. 2005 Jan;79(2):884-95. doi: 10.1128/JVI.79.2.884-895.2005.
PMID: 15613317; PMCID: PMC538593.
9: Yaqinuddin A.
Cross-immunity between respiratory coronaviruses may limit COVID-19 fatalities.
Med Hypotheses. 2020 Jun 30;144:110049. doi: 10.1016/j.mehy.2020.110049. Epub
ahead of print. PMID: 32758887; PMCID: PMC7326438.
10: Greenberg SB.
Update on Human Rhinovirus and Coronavirus Infections. Semin Respir Crit Care
Med. 2016 Aug;37(4):555-71. doi: 10.1055/s-0036-1584797. Epub 2016 Aug 3. PMID:
27486736; PMCID: PMC7171723.
11: Duggal NA,
Pollock RD, Lazarus NR, Harridge S, Lord JM. Major features of
immunesenescence, including reduced thymic output, are ameliorated by high
levels of physical activity in adulthood. Aging Cell.
2018;17(2):e12750. doi:10.1111/acel.12750
12: Lazarus NR, Lord
JM, Harridge SDR. The relationships and interactions between age, exercise and
physiological function. J Physiol. 2019;597(5):1299-1309.
doi:10.1113/JP277071
13: Hogan Ii RB,
Hogan Iii RB, Cannon T, et al. Dual-histamine receptor blockade with cetirizine
- famotidine reduces pulmonary symptoms in COVID-19 patients [published online
ahead of print, 2020 Aug 29]. Pulm Pharmacol Ther. 2020;63:101942.
doi:10.1016/j.pupt.2020.101942.
14: Minnesota
Influenza Incidence Surveillance Project, (MIISP). Minnesota Department of Health.
Correspondence on circulating common coronaviruses in Minnesota. Received
on 9/19/2020.
15: Loos C, Atyeo C, Fischinger S, Burke J,
Slein MD, Streeck H, Lauffenburger D, Ryan ET, Charles RC, Alter G. Evolution
of Early SARS-CoV-2 and Cross-Coronavirus Immunity. mSphere. 2020 Sep
2;5(5):e00622-20. doi: 10.1128/mSphere.00622-20. PMID: 32878931; PMCID:
PMC7471005.
Supplementary 1:
My wife tested negative for SARS-CoV-2 IgG antibodies today (9/22/2020) in addition to the negative nasal swab PCR tests - making her an unlikely source of infection.
Supplementary 2:
COVID-19 follow-up:
Saw my internist yesterday (9/25/2020).
My course of the illness was "average" for all of the patients he has seen. He agreed that PCR false positives are not likely but false neg are. He declined Ab testing. I applied to the Red Cross convalescent plasma program.
.jpg)