
I have been a member of the Movement Disorder Society since 1993. I decided to join after having nothing but positive experiences at the annual Aspen courses led by Stanley Fahn, C. David Marsden, and Joseph Jankcovic. Although Dr. Marsden has passed away, the course is still being given by two of the original lecturers with additional faculty. The level of scholarship and expertise in this conference is really not approached by many venues these days. Each conference provided participants with a 700 page textbook like syllabus on everything that you ever wanted to know about movement disorders. Once you attend a conference like this it is a life transforming event. Suddenly you are following the lecturers, you read what they write and you acquire some of their books. I changed my Neurology text to Neurology in Clinical Practice because both Jankcovic and Marsden were editors. I also received the video material and text of Movement Disorders, the official journal of the International Parkinson and Movement Disorder Society.
People often ask why I am member of what is predominantly a neurological society? In Minnesota there were only three psychiatrists who were members of the organization. Stan Fahn asked me that himself at one of the conferences. I don't remember exactly what I said, but he thought my answer at the time was acceptable. It comes down to clinical expertise and with the confluence of the dorsal and ventral striatum - neuroanatomy. Back in the days that I went to medical school, nobody talked about the ventral striatum only the dorsal striatum and even back then, the main clinicopathological correlate was movement disorders. As medical students we learned primarily about Huntington's Disease, Wilson's Disease, and Parkinson's Disease. Nothing at all about dystonias or other disabling movement disorders and their treatments. Nothing about the last members of the generation afflicted by what we called in those days post-encephalitic Parkinson's and all of the associated neuropsychiatric morbidity. In my rotations at Milwaukee County Hospital and affiliated institutions I saw all kinds of undiagnosed or poorly diagnosed movement disorders. There were no movement disorder specialists in those days and no treatments except for Parkinson's. The quality of care is slightly improved today in that referral to movement disorder specialists and an appropriate diagnosis can occur, but the total number of these specialists is very small.
That is where psychiatrists need to fill in the gap. My initial interest was tardive dyskinesia and describing the motor disorders of patients who in many cases had never been exposed to a medication. But it quickly became recognizing the early manifestations of idiopathic and iatrogenic movement disorders and using these diagnoses in a comprehensive diagnostic approach to the patient as well as the treatment plan. When you take that approach it is an eye opener. In my role as a consultant it is amazing how much undiagnosed movement disorder pathology is out there. A couple of examples will illustrate the problem. About 50% of young adults with childhood diagnoses of Attention Deficit-Hyperactivity Disorder (ADHD) who have been treated with stimulants have a movement disorder usually in the form of vocal tics, motor tics, or Tourettes. About 100% of those patients tell me that nobody has ever told them about those diagnoses before. Of course there is an exhaustive list of medication and environmental exposures that can lead to tic disorders, so there is a question of whether something occurred since childhood. In the same population there are a group of people with choreiform movements and predominately extensor muscle tone. They are not aware of the movement disorder and nobody has mentioned it before. It is as though clinicians consider these movements to be part of ADHD. One of my observations about tardive dyskinesia has been that the overall prevalence of the disorder has dropped off significantly with the advent of atypical antipsychotic medication. That does not mean that is has gone to zero and the augmentation of antidepressants with aripiprazole seems to be a new source of that disorder. Most significantly, the people who are at greater risk for the problem do not seem to have been carefully screened ahead of time. They are not routinely assessed for akathisia or other early motor symptoms like micrographia, diminished arm swing, or hypophonia.
The course was presented by three neurologists Cynthia Comella, MD; Rajesh Pahwa, MD; and Jerrold L. Vitek, MD, PhD. It was presented by the University of Kansas Medical Center and all of the brochures and specific courses are available on this web site. The course was unusual in its rapid presentation of topics and strict adherence to that schedule. There were ten presentations by the faculty varying in length from 20 to 55 minutes in duration. The morning presentations covered Parkinson's and Parkinsonism, Restless Leg Syndrome, Tremor Disorders, and Movement Disorders in Psychiatry. The afternoon covered Dystonia, Chorea, Tics, Neurotoxin and Deep Brain Stimulation for Neurological and Psychiatric Disorders. The entire set of PowerPoints (without the videos) was included in the course syllabus. The slides were all very readable in a standard format. The Psychiatric Aspects of Movement Disorders was a very interesting presentation because it covered a wide range of problems that acute care and geriatric psychiatrists come in contact with including Parkinson's Disease and the associated psychiatric comorbidity, Tardive Dyskinesia, Neuroleptic Malignant Syndrome, Serotonin Syndrome, and Psychogenic Movement Disorders. Interest in these topics may reflect exposure to the problem. In seeing patients with Parkinson's and psychosis for example one of the commonest problems is that antipsychotic medications will generally make their psychosis worse. The only exception to that is clozapine and that comes with a host of comorbidities and monitoring issues itself. One of the presenters suggested that quetiapine is a default choice in many cases even though it is not ideal and efficacy is low. A new medication for the treatment of psychosis in PD was mentioned called Pimavanserin. It is a selective serotonin 5-HT2A inverse agonist without significant activity at dopaminergic, histaminergic, muscarinic, or adrenergic receptors. Practical approaches to treating dementia, anxiety, and depression associated with PD were also discussed.
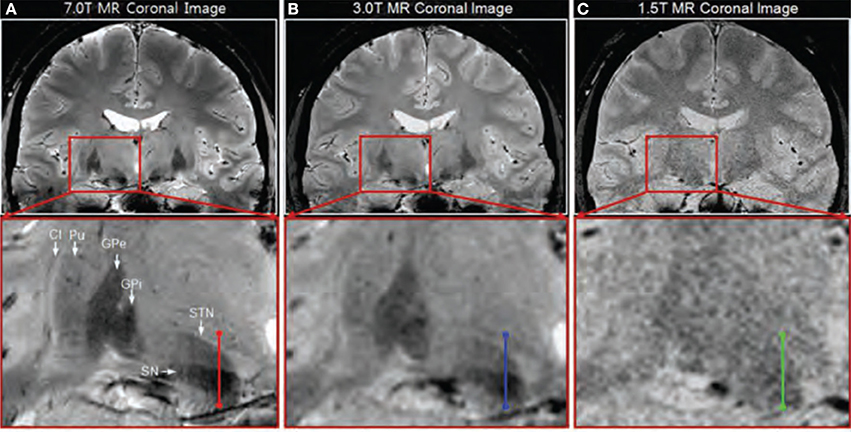
The most fascinating part of the course was the section on deep brain stimulation (DBS). A fairly detailed description of the procedure was given. Deep brain stimulation is currently FDA approved for Essential tremor and Parkinsonian Tremor and Parkinson's Disease with humanitarian device exceptions for Primary Dystonia and Obsessive Compulsive Disorder. This section was presented by Dr. Vitek who has a wide range of experience with this method. Before and after videos of children and adults with disabling movement disorders were presented and the results were striking. The general concept presented was that any "circuit disorder" was a potential candidate for DBS and that is consistent with the current literature on the subject. The other important concept is that with DBS there are no permanent changes in the brain apart from the low risk of placement complications. That is not true for neurosurgical techniques that have been used for the same neurological and psychiatric complications. In the case of DBS the stimulator can be reprogrammed, turned on or off in a number of configurations, and turned completely off. An unexpected benefit of the DBS presentation was a look at brain images from a 7 Tesla MRI scan. The resolution of these images was incredible arguably as good as artistic renderings of brain anatomy. Take a look at the side by side comparisons to what is currently clinically available.
Everything considered this was an excellent conference and I recommend it to anyone if it comes to your area. I think it could be used by practicing psychiatrists who want to get up to speed on movement disorders, residents wanting to do the same thing, and psychiatrists studying for their boards in geriatric psychiatry. It also raises a larger question of just what psychiatrists should be able to diagnose and treat? What should they know at a theoretical level? Based on my experience, psychiatrists seem to be the specialists that are most likely to be confronted with an undiagnosed movement disorder in patients who have seen primary care physicians or pediatricians. Psychiatrists are also specialists who should be the experts in how to recognize and prevent motor complications of medications used to treat psychiatric disorders. Psychiatrists have also been using the same interview and mental status exam technology for the past 50 years. Changes need to be incremental and the logical first change that seems in order is to be able to recognize, diagnose, and treat or refer movement disorders encountered in standard psychiatric practice. Psychiatrists interested in neuroscience with also find this a very interesting area for ongoing study. And subspecialists like geriatric psychiatrists are probably going to need to know the difference between tauopathies and synucleinopathies.
This course is a good one to get you on that road.
George Dawson, MD, DFAPA
Attribution: My own picture shot at the John Rose Oval in Roseville, Minnesota.






{kind=link}