One of the best illustrations of a psychiatric concept is your own personal observation as a physician. This really happened to me quite a while ago but even that has implications....
When I was 22 years old I was playing in a football game. It was a city league touch football game. At that point I had probably been playing football in one form or another every day of the year for the previous 10 years. The typical game was passing 2 on 2 in the street. In this game, it was across the whole field and I think we had 8 men on the field. I knew everyone on the team. On defense, I was a cornerback and on offense - the quarterback. In the context of all being 20+ year old men we were all fairly intense. That probably explains why when a pass was thrown into our defense I ran and dove headlong for the ball.
That was just about the last thing I remember from that day. I can recall glimpses of the fact that I apparently stayed in the game. No recollection of getting my hands on the ball, the impact, breaking my nose, bleeding somewhat, how long I was on the ground, or other plays. During the dive for the ball, I smashed my face into the shoulder of our other cornerback and was knocked out. Later he told me his shoulder was sore from the impact. We were both running toward one another at full speed. A few flashes of standing in the huddle and not responding to questions very well is all that I can recall for the rest of that game. I made it home. I vaguely remember an argument where I was asked why I was so irritated. My memory and baseline conscious state didn't come back until until about 2PM the next afternoon in a physical chemistry class. That was about 18 hours after the game. At no point was I seen by a physician.
The first question that comes to mind is "Was this a concussion or a traumatic brain injury or both?" I ask every person I see about head injuries and try to figure out if there was an associated brain injury. It is one of the most important parts of the psychiatric assessment. I get a full spectrum of responses from people who say they were knocked out but did not have a concussion to people who had a concussion but were not knocked out to those were in a coma for 5 days or more.
For people of my generation there were two myths that actively interfered with the care of traumatic brain injuries and concussions. The first was that you could just return to the game. The number of people I have interviewed who were football or hockey players who tell me they were knocked out multiple times including several times in the same game is shocking. Returning to the game with a concussion injury or mild TBI is a horrifically bad idea because if another incident occurs it could lead to a devastating brain injury that could be life-threatening. The second myth is that some players cannot be easily replaced in high school or college. If your star player gets a concussion, the chances that the replacement will not do as good is the difference between winning and losing. The problem with that logic is that the performance of the impaired player has to be seriously deteriorated. On my team, I was certainly not the star but we had no replacements. That is not the best plan. To this day, I do not recall the second half of the game but it was not good. The risk of a life threatening injury is certainly not worth the potential reward of hoping to maintain expected performance to win a game.
What are the current definitions of traumatic brain injury and coma? I had the opportunity to attend a recent Door County Summer Institute program given by Sheldon Benjamin, MD. The program was entitled Practical Neuropsychiatry for Clinicians. The second day of the course was all about traumatic brain injuries that included the definitions, clinical syndromes, diagnosis, pathophysiology, and treatment. Traumatic brain injuries are very common in the US in terms of overall incidence and prevalence (2) and also by comparisons with other neurological and psychiatric diseases. 56,800 people died of TBIs in 2014 including 2.529 children. The common injuries leading to death include intentional self-harm (32.5%), falls (28.1%), and motor vehicle accidents (18.7%). Older patients are at highest risk. The overall prevalence as a percentage of the population at about 1.5% rivals major mental disorders.
The goal of this post is to describe my traumatic brain injury from long ago using modern criteria to suggest the best possible format to record this information. First off, was it a concussion or a traumatic brain injury (TBI)? The CDC definition of TBI is a disruption in the normal function of the brain that can be caused by a bump, blow, or jolt to the head or a penetrating head injury. The jolt to the head can include blast injuries or any sudden acceleration/deceleration movement to the head. Disrupted brain function must occur in proximity to the injury and can be observed by changes in level of consciousness, memory loss, focal neurological findings, or additional mental status changes. Once the mechanism of injury and clinical features have been determined further classification into mild, moderate and severe TBI can be made.
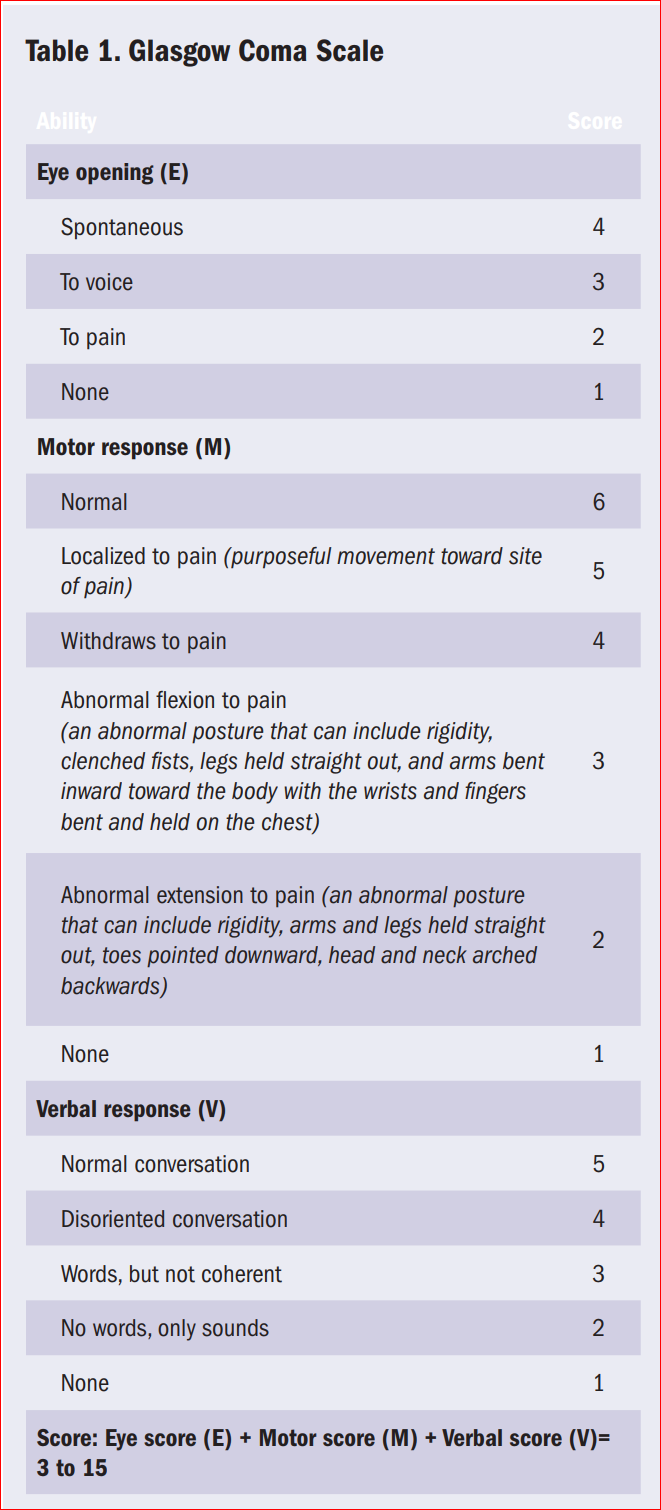
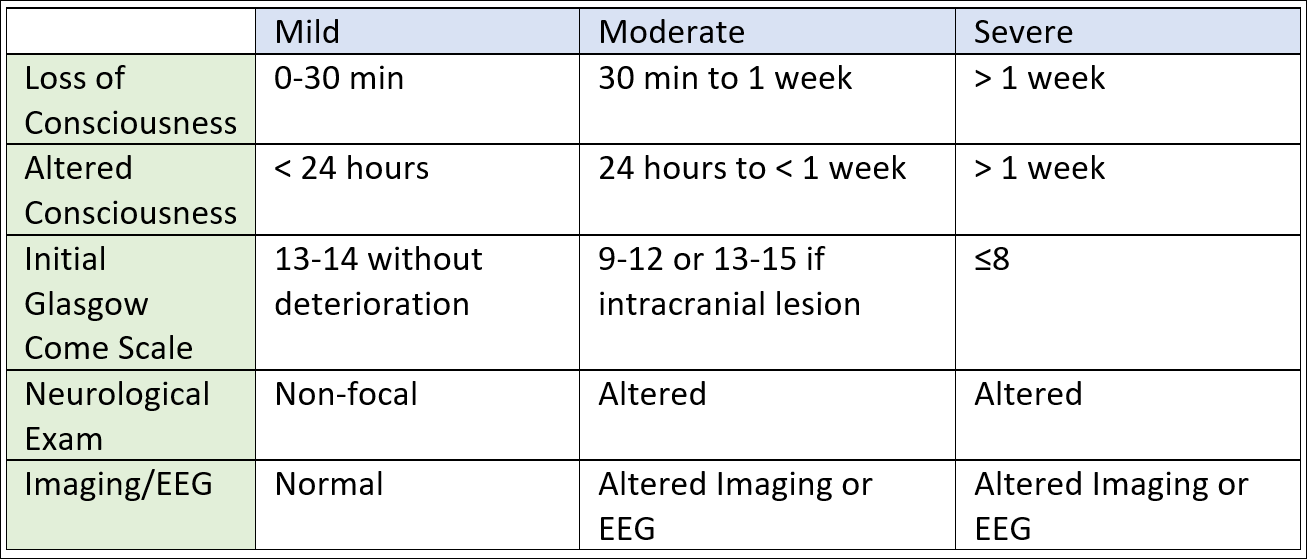
And what is the difference between a TBI and a concussion? Concussions are by definition with or without loss of consciousness but are described with a number of symptom complexes (headaches, irritability, insomnia, depression, etc) but there are no major neurological symptoms or imaging evidence of injury. The classification of mild, moderate and severe TBI is done on the basis of the time where consciousness was lost, Glasgow Coma Scale ratings at the time of presentation (see Supplement 1), presence of neurological findings, presence of imaging and EEG abnormalities. Using these definitions a concussion would be considered a mild TBI according to those categories.
My opening question to people is whether or not they have ever been knocked out. An affirmative response means a concussion or at the minimum mild TBI. If no LOC questions about associated post-concussion symptoms are relevant. On a clinical basis, using this scale retrospectively without access to the original record can be a problem, but patients often remember relevant parts of the records. For example, people often recall if they were told that their imaging study was abnormal or not. They can recall hearing that they had "blood in the brain" and in some cases that they were in a TBI rehab program for a while. A description of the approximate periods of retrograde and anterograde amnesia is also useful. For example, in the case of the TBI that I sustained - it would be mild. I could also say I had a concussion. Both are better specified with comments about the specific features. Actual loss of consciousness (LOC) was on the order of minutes. Altered consciousness was about 18 hours. My guess is that the GCS would have been a 15 if I had been taken to the emergency department and because I was not seen by a physician no imaging studies or EEGs were done. Subsequent to this injury I have had normal MRI scans and EEGs. If I was seeing myself as a patient based on that history I might document:
"There is a remote history of a mild TBI that occurred following a collision during a football game with several minutes of LOC, a minute or two of retrograde amnesia, and 18 hours of altered consciousness with patchy anterograde amnesia. There were no postconcussional symptoms past 18 hours. The patient has had subsequent MRI scans of the brain and EEGs both years later that were noted to be normal."
Other useful descriptions include what the ICD-10 describes as the disparate symptoms of postconcussional syndrome.
In the weeks ahead I hope to post more information on the pathophysiology of traumatic brain injuries and why that is important to psychiatrists. For now I will just be grateful that the poor judgment of my 22 year old self did not lead to significant disability or death. There is some epidemiological data to suggest patients with TBIs are more likely to get Alzheimer's disease so I may not be out of the woods yet. The good news is that this is an active area of research, that treatment approaches do work for people with deficits, but like all of medicine these days they are rationed by health care companies.
George Dawson, MD, DFAPA
References:
1: Centers for Disease Control and Prevention. (2015). Report to Congress on Traumatic Brain Injury in the United States: Epidemiology and Rehabilitation. National Center for Injury Prevention and Control; Division of Unintentional Injury Prevention. Atlanta, GA. Link
2: GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019 Jan;18(1):56-87. doi: 10.1016/S1474-4422(18)30415-0. Epub 2018 Nov 26. PubMed PMID: 30497965. Link
3: Brain Injury Awareness Month — March 2019. MMWR Morb Mortal Wkly Rep 2019;68:237. DOI: http://dx.doi.org/10.15585/mmwr.mm6810a1
4: Bellner J, Jensen S-M, Lexell J, Romner B. Diagnostic criteria and the use of ICD-10 codes to define and classify minor head injury. Journal of Neurology, Neurosurgery and Psychiatry 2003;74:351-2. Link
5: Defense and Veterans Brain Injury Center. ICD-10 Coding Guidance for Traumatic Brain Injury. Link
Additional Resource:
Neuropsychiatry Pocket Reference or Brain Card by Sheldon Benjamin, MD and Margo Lauterbach, MD is a booklet of 7 laminated reference cards that covers the neuropsychiatric exam and syndromes of interest to psychiatrists working in this field. It is an excellent inexpensive resource that connects the purchaser to a web site of extensive additional information. Available from braineducators.com

Supplementary 1: