
A copy of Minnesota Medicine, the journal of the Minnesota Medical Association (MMA) was delivered to my office this morning. I stopped paying dues to the MMA about 20 years ago. My rationale was that I was already paying significant dues to two professional organizations that were doing nothing to protect me from the repeated abuses of the managed care industry - why pay a third to do an equally poor job? I was probably more steamed at the MMA at the time because I realized that managed care in Minnesota was more than just an annoying business practice, it was institutionalized in both the statutes and administrative practices of the state government. I sent the President of the MMA a letter to that effect. I don't have his response but it did not persuade me to send them another check. I can only guess that this is a marketing idea to persuade the disaffected that the MMA is now a vital organization that appreciates medical practice in the state in many cases has come perilously close to being a living hell. That living hell is courtesy of managed care and the various heads of that hydra.
Despite those reservations, on the front page just below the journal title was this headline: The Prior Authorization Burden and just below that the subtitle: The process is frustrating, time-consuming and costly. No kidding. Any casual reader of this blog may recognize that this is probably one of the only sites where you can count on rigorous criticism and aggressive opposition to all managed care techniques. At the top of that list is prior authorization. I have gone as far as coming up with a "no-Rx" logo that I use to symbolize the problem. That symbol is at the top of this post. It means that a managed care company (MCO) or pharmaceutical benefit manager (PBM) can deny prescriptions and therefore medication to the patient. That denial is also a denial of the prescription of the physician and everything that involves. State and federal governments have granted these organizations this power based on some loose idea that it would save patients and the governments money. These governments are still enamored with that idea despite the overwhelming evidence that money is not really saved, it is merely redirected to the bottom line of MCOs and PBMs. The only people who pay the price are patients and physicians.
So my first and primary question was "Does the medical society finally get it?" They certainly missed the boat on utilization review and as a result managed care organizations in Minnesota generally make the discharge decisions on patients. Will they also continue to make decisions about what medications can be prescribed based on their profit margins rather than what a physician in a treatment relationship with the patient decides? The initial example seemed hopeful. It was the story about a primary care physician trying to prescribe a rescue inhaler for his asthmatic patient. He had taken a specific brand of generic albuterol for years. The prescription was rejected. He wrote subsequent decisions for identical medications in the same category Proventil and that was rejected. He sent in a script for ProAir and that was rejected. He was told to choose another inhaler but not given a name to choose. He picked Xopenex or levalbuterol rather than albuterol and that was accepted. What is the rationale for a PBM having a doctor guess about which inhaler will be approved for days while a patient with severe asthma goes through the weekend without a rescue inhaler? In a word money, the only rationale for picking a newer and (usually) more expensive inhaler is that the PBM has some kind of financial deal with that manufacturer.
The article does go on to explore that theme and references a study of six Minnesota Health Plans. The researcher Barbara Daiker, RN, PhD found that there were 1,036 drugs that required prior authorization but only 6 were on the prior authorization list of all 6 health plans. Only 26 more were on 5 of the 6 lists. This level of variability suggests that the decisions are not based on scientific evidence or quality concerns but financial models. It would have been very useful to know if any of these lists included generic drugs. Without a scientific or quality basis for these lists, the obvious model is a purely financial one. That is also consistent with the tactics used by these companies that I have documented in this blog such as refusing to cover generic antidepressants that can be purchased for as little as $4.00 per month.
One of the facts about prior authorization is that like most managed care tactics, the burden has fallen disproportionately on psychiatric practice and patients with mental illness. One of the first articles demonstrating the adverse effects of prior authorization was published in the New England Journal of Medicine in 1994 (2) showing that when prescription limits were imposed on patients with severe chronic mental illness it resulted in increased health care costs that exceeded the savings in medication by a factor of 17. In a more recent study, Driscoll and Fleeter (3), estimated the adverse effects (hospitalization, lost wages, homelessness, incarceration, higher medical costs) of prior authorization applied to the population of Ohio residents with schizophrenia and bipolar disorder. They used conservative estimates of the population at risk and treatment discontinuity as a result of prior authorization programs. They determined associated indirect costs with these treatment discontinuities and summarized his results in the following table.
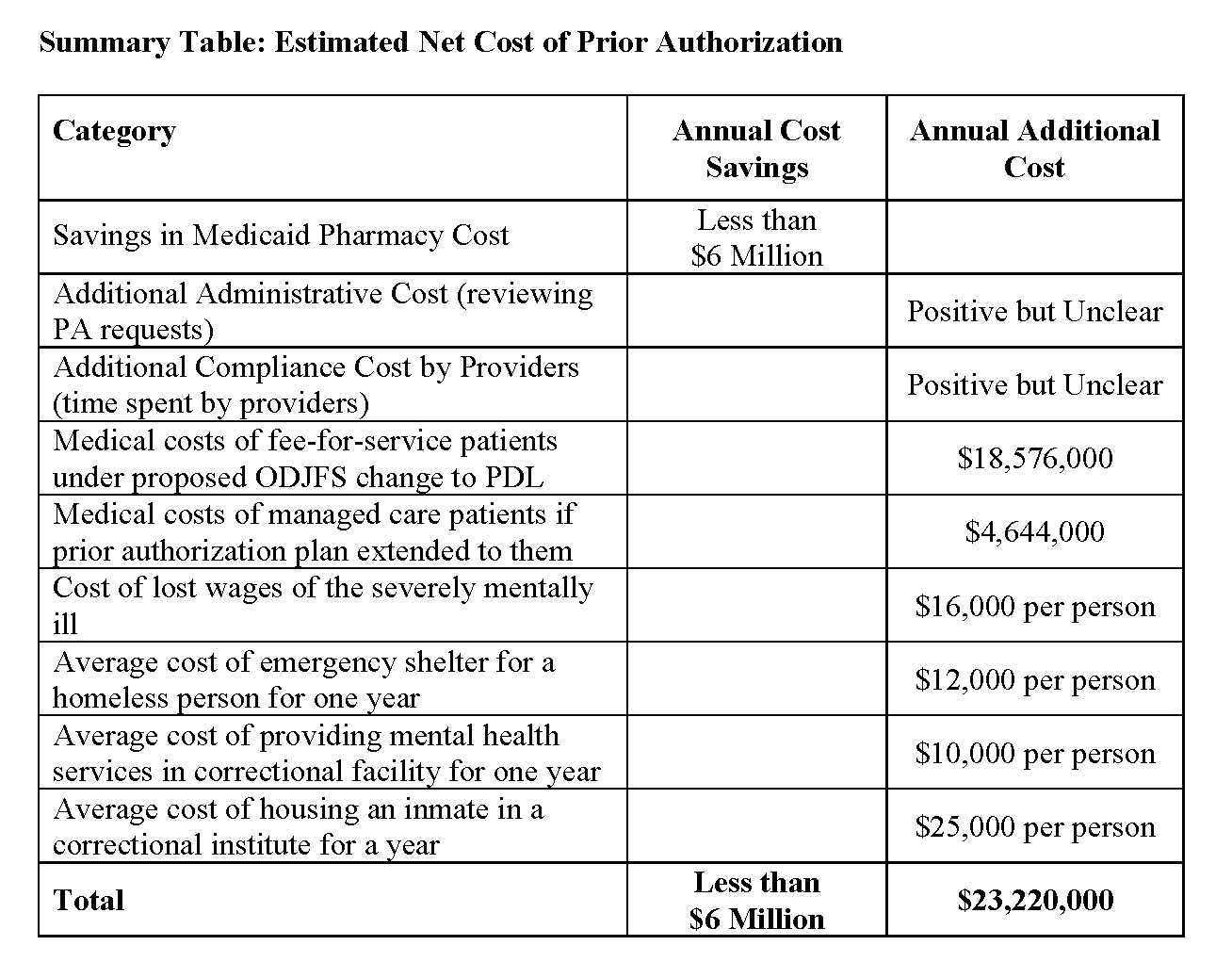
These studies all demonstrate that "savings" from prior authorization is savings to a health care company and it does not benefit the patient involved. The costs to the providers in the case of the above table were not even used but per my previous reference are considerable. I would also add that since this study came out most of the original second generation antipsychotics are now generic drugs and that reduces the Annual Cost Savings considerably. The estimates for Annual Additional Cost are much higher and don't include the paperwork costs for physicians. In other words the net added cost of prior authorization for psychiatry is considerable higher in 2014 than it was in 2008.
With all of these considerations it is good to see the state medical society finally paying attention. That doesn't mean anything will be done and the evidence for that is contained in this quote from Janet Silversmith, Policy Director of the MMA: "We are not trying to eliminate drug prior authorization. We are just trying to add some sanity to the process. As it's practiced now we believe drug prior authorization is an onerous, inefficient process that sometimes harms patients."
Why wouldn't any medical society want to kill that kind of process?
George Dawson, MD, DFAPA
Refs:
1: Howard Bell. The prior authorization burden. Minnesota Medicine. November/December 2014: 18-25. PDF
2: Soumerai SB, McLaughlin TJ, Ross-Degnan D, Casteris CS, Bollini P. Effects of a limit on Medicaid drug-reimbursement benefits on the use of psychotropic agents and acute mental health services by patients with schizophrenia. N Engl J Med. 1994 Sep 8;331(10):650-5. PubMed PMID: 8052275.
3: Howard Fleeter, PhD. Estimate of the Net Cost of A Prior Authorization Requirement for Certain Mental Health Medications. Prepared by Driscoll and Fleeter for National Alliance on Mental Illness Ohio. August 2008. (Table used with permission).
Supplementary 1: The "No - Rx" logo simultaneously symbolizes no prescription for the patient, no acceptance of a prescription from a trained and licensed physician, cost savings for the insurance entity that contracts with the patient to cover their prescription medications, and increased costs for all of the providers, employers, governments and correctional systems that need to address discontinuities in care.