 |
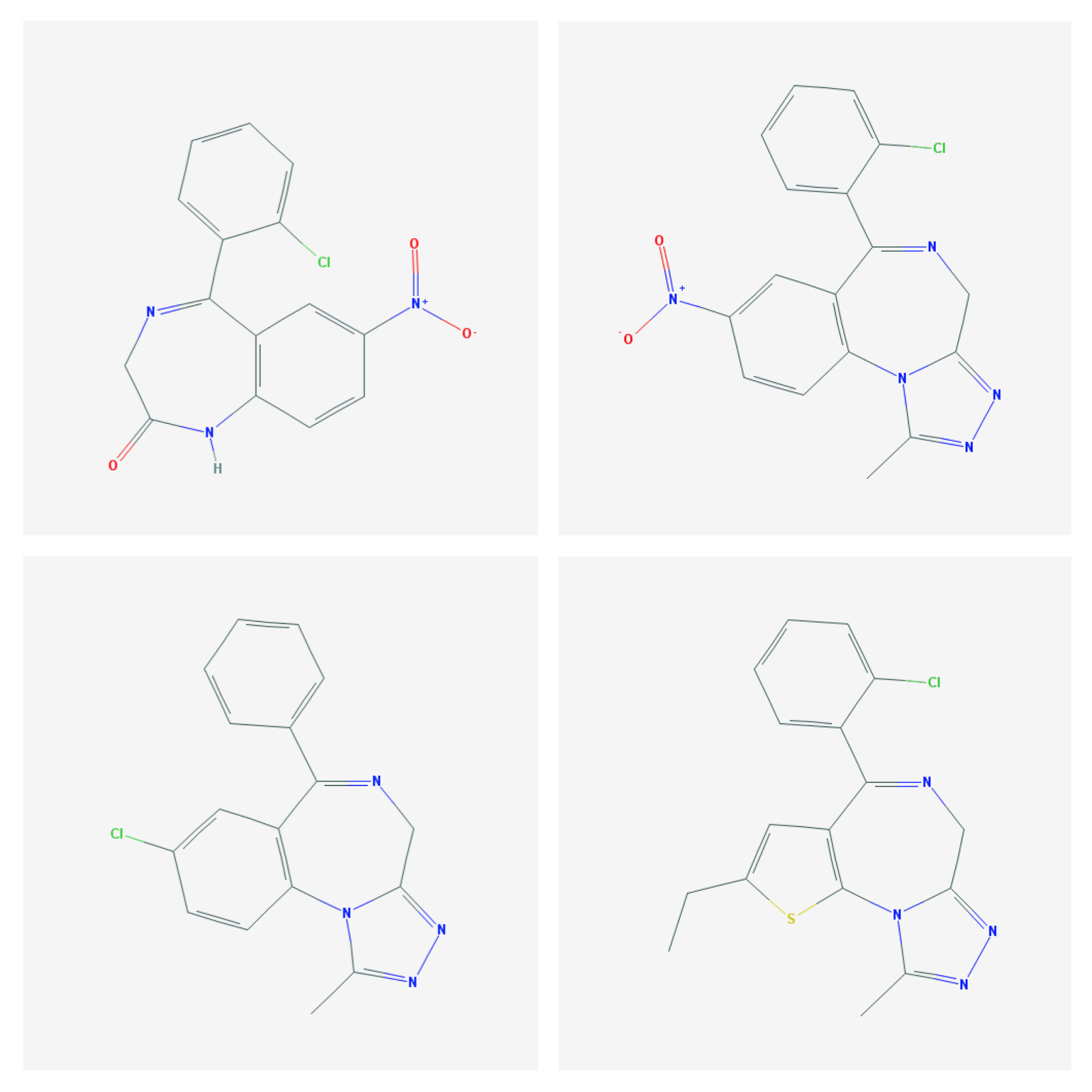
| Benzodiazepine structures clonazepam (upper left) and alprazolam (lower left) are both prescription benzodiazepines. Clonazolam (upper right) and etizolam (lower right) are not. |
Designer benzodiazepines are benzodiazepine class drugs that are not approved for therapeutic use in any country. They are analogues that were synthesized by drug companies, and in some cases went to clinical trials and published results but never made to to market. The name makes is seem like there are chemists out there synthesizing these drugs for a purpose, but there are not. They are all part of the original research for benzodiazepine class medications that has not really seen any innovation in decades. These drug are a current problem because there are online sources allow people to purchase them in tablet, capsule, powder, and blotter form. There are several online venues where users talk about their experience and which drug creates the "best" high. Medical staff need to realize that many of these drugs are undetectable as molecules. They show up as "false positives" in standard toxicology testing largely due to a lack of reference material. Drug users are often told that the drug is undetectable in standard toxicology assessments and that the drugs are also not listed as a standard prohibited substance and therefore it is a "legal" high. That is a fairly weak argument when users are overtly intoxicated and sustain all of the consequences of intoxication.
Just as a check I looked at a list of 13 designer benzodiazepines (1) (clonazolam, deschloroetizolam, diclazepam, estazolam, etizolam, flubromazepam, flubromazolam, flutazolam, 3-hydroxyphenazepam, meclonazepam, nifoxipam, phenazepam, and pyrazolam) and compared them to the most recent posted list of Controlled Substances from the DEA. Only one of those compounds (estazolam) is listed on the most current list dated 05-May-17. It is listed as a Schedule IV drug. I have no way of knowing which compounds are being considered for the list. Just being on the list does not deter the illegal sale of controlled substances, but the designer designation generally means that there is far less known about the drug in terms of safety. In some cases the toxicology lags behind exposures because the physicians treating intoxication, withdrawal, and overdoses with these compounds are uncertain about what they are treating. The patient or collateral contacts of the patient may not know what the drug is and that lag time creates additional danger for the patient.
The first time I searched for clonazolam on Medline, I was impressed with the fact that there were only 5 references in the medical literature including the analysis reference that listed 13 designer benzodiazepines. In fact, they all had to do with analysis but also described the complications of intoxicated driving (2) while taking them and the complications of life threatening intoxication (3). The minimal online information available suggests that it has very high potency. There are doses suggested in the range of high potency benzodiazepines but there are no clinical applications. As a result, there are no FDA package inserts or even reliable data from other agencies. It is not listed in the British National Formulary (bnf.org). Despite this lack of clinical information and application, it is immediately obvious that large quantities are available for purchase online. On these sites it is described as a research chemical with no clinical applications. It is also described as not for human consumption - a label I am familiar with from synthetic cannabinoids. The current problem is that as long as this chemical or its precursors are not listed as controlled substances anyone can purchase it for any purpose. The suggested prices quoted for this drug are far below the street price of diverted prescription benzodiazepines. That makes these compounds ideal for illegal trafficking.
Searching etizolam on Medline resulted in 96 references and 13 clinical trials. Some of the trials were as recent as 2009. The trials were for anxiety disorders and based on the abstracts the results sound equivocal ranging from improvement over 4 weeks to (4) to no improvement (5). The striking feature of the trials is the dose of etizolam being 0.5 mg BID indicating that it is a high potency benzodiazepine. The fact that several studies were done and the drug was never approved suggests either the lack of sufficiently powered studies or some side effect that was obvious only to the pharmaceutical company or regulators. In some cases the drug is also too difficult to use clinically. There are several examples of benzodiazepine class medications that were determined to be problematic after use and either banned at that point or an additional warning was issued.
One of the more disturbing trends recently in the number of benzodiazepine compounds that are involved in polypharmacy overdoses. In the most recent analysis of overdoses by the CDC - 2 of the top 10 compounds were alprazolam and diazepam - both prescription benzodiazepines. In both cases 95% of these overdoses involved concomitant drugs. In the US, 30% of fatal opioid overdoses involve benzodiazepines. Due to the current problems with analysis, it is highly likely that designer benzodiazepines involved in overdose deaths are not detected. This is a compelling reason to not use designer benzodiazepines.
Reading through some of the web sites that promote the use of these compounds, it is ironic that there are messages out that that these drugs can be used safely with adequate research by the user on the Internet. Prescription medications are understood to have qualified safety when they are approved by the FDA and prescribed by a qualified physician. There are still completely unanticipated reactions and these approved medications are not generally tested with other addictive compounds. There are reactions that can only be detected by pharmacosurveillance of a much larger database. In the case of these designer benzodiazepines, they are not approved, not prescribed, and highly potent drugs being sold by sources with no responsibility to the user.
Anyone seeking to get high in that context should be questioning the value of getting high.
George Dawson, MD, DFAPA
References:
1: Pettersson Bergstrand M, Helander A, Hansson T, Beck O. Detectability of designer benzodiazepines in CEDIA, EMIT II Plus, HEIA, and KIMS II immunochemical screening assays. Drug Test Anal. 2017 Apr;9(4):640-645. doi: 10.1002/dta.2003. Epub 2016 Jul 1. PubMed PMID: 27366870.
3: Łukasik-Głębocka M, Sommerfeld K, Teżyk A, Zielińska-Psuja B, Panieński P,Żaba C. Flubromazolam--A new life-threatening designer benzodiazepine. Clin
Toxicol (Phila). 2016;54(1):66-8. doi: 10.3109/15563650.2015.1112907. Epub 2015
Nov 20. PubMed PMID: 26585557.
4: Savoldi F, Somenzini G, Ecari U. Etizolam versus placebo in the treatment ofpanic disorder with agoraphobia: a double-blind study. Curr Med Res Opin. 1990;12(3):185-90. PubMed PMID: 2272192..
5: De Candia MP, Di Sciascio G, Durbano F, Mencacci C, Rubiera M, Aguglia E, Garavini A, Bersani G, Di Sotto A, Placidi G, Cesana BM. Effects of treatment with etizolam 0.5 mg BID on cognitive performance: a 3-week, multicenter, randomized, double-blind, placebo-controlled, two-treatment, three-period, noninferiority crossover study in patients with anxiety disorder. Clin Ther. 2009 Dec;31(12):2851-9. doi: 10.1016/j.clinthera.2009.12.010. PubMed PMID: 20110024.
4: Savoldi F, Somenzini G, Ecari U. Etizolam versus placebo in the treatment ofpanic disorder with agoraphobia: a double-blind study. Curr Med Res Opin. 1990;12(3):185-90. PubMed PMID: 2272192..
5: De Candia MP, Di Sciascio G, Durbano F, Mencacci C, Rubiera M, Aguglia E, Garavini A, Bersani G, Di Sotto A, Placidi G, Cesana BM. Effects of treatment with etizolam 0.5 mg BID on cognitive performance: a 3-week, multicenter, randomized, double-blind, placebo-controlled, two-treatment, three-period, noninferiority crossover study in patients with anxiety disorder. Clin Ther. 2009 Dec;31(12):2851-9. doi: 10.1016/j.clinthera.2009.12.010. PubMed PMID: 20110024.
No comments:
Post a Comment