I have been contacted by a number of psychiatry residents lately about this blog. Their comments are encouraging and remind me that practically everything that I post here is focused on practicing psychiatrists - especially people on the front lines being exploited by one government or healthcare corporation or the other. The comments also remind me that in retrospect residency and medical school was an exciting time and that there is really not much time between then and becoming a senior clinician. The vast majority of us negotiate that turf with very few problems but in some cases glaring mistakes are made that sidetrack careers or stop them in their tracks. There also seems to be an unnecessary amount of anxiety, typically due to a lack of clarity and plenty of situations without solutions. It seems to me that there is never enough guidance for psychiatrists in training. That situation is often made much worse by the fact that psychiatrists in most tertiary care centers are viewed as the physicians who take care of problems that do not neatly fit into other specialty areas. I thought I would post a few landmarks and tips that can lead to avoiding big problems and facilitate the transition to a practicing psychiatrist.
1. Boundaries, boundaries, and more boundaries...... - There is probably nothing more important in training and in the field than maintaining the appropriate boundaries of a professional. That means with your patients certainly but also with other professionals and medical staff, colleagues, and even people seemingly peripheral to the treatment process. There are many definitions of boundaries than invoke psychodynamic terms that are inaccessible to most. The most basic definition is that the psychiatrist is always aware of their special role in the treatment process and the fact that their behavior is dictated by a professional code that recognizes the physician must act in the interests of the patient. That certainly involves maintaining confidentiality but also subtleties such as determining why a certain patient evokes an emotional response or reaction that other patients do not. Most training programs discuss the issue of sexual involvement with patients and why that is absolutely forbidden. Boundary violations can be as subtle as being more available for one patient relative to the others and rationalizing this as the patient needing crisis intervention that only you can provide. To a certain extent residency is about picking up these subtleties, but in many cases it takes years of practice to recognize the most subtle boundary problems. Treating the family member of a friend or colleague is a case in point. Training staff should always be available for consultation on those issues. A good general rule is to always see the patient in a designated clinic at the appointed time, for the correct duration, and always document what occurred in the session using standard clinical documentation. Any unexpected thought or feeling on the part of the resident during the sessions should be considered for discussion with faculty supervisors. It is advantageous for faculty to describe what those scenarios might be in order to provide more active guidance. Many boundaries are more clearly delineated now than at any time in the past. For example, it was common practice in the past to be approached by somebody who was not your patient (usually a friend, relative or coworker) with a request for a prescribed medication. The usual rationale was it was more convenient to get it from you than their personal physician. Responding in many cases was problematic. Today it is quite easy to point out that most boards of medical practice take a negative view of prescribing to people where no physician-patient relationship and no documentation of an encounter exists.
2. Therapeutic neutrality - Figuring out why psychiatrists need to be neutral in their interactions with patients takes some doing. You may have just finished a rotation with a very demonstrative non-psychiatric physician and seen some interpersonal behaviors that you are not observing in your psychiatry staff. Asking them why they interact with people in a certain way and why they make specific comments to patients is an important part of the training. They should be able to explain themselves.
3. Pattern matching and other skills - The main advantage of physician training is the development of pattern recognition and pattern matching skills that covers a broad range of clinical experiences. The best way to differentiate between an acute pulmonary embolism, a myocardial infarction, and and a panic attack is to see every possible variation. That will make your chance of making the correct diagnosis much greater than a person who has read about it in a book. Some studies have looked at the number of recognizable patterns that can be detected by the human brain. For visual modalities alone that number approaches about 80,000 patterns.
4. Getting on top of the countertransference - During any training you will see a diverse number of clinicians with diverse theoretical backgrounds demonstrating their techniques. There may be some confusion about the benefits of therapeutic neutrality. Some people see it as being non-directive or even confusing to the patient. The equate neutrality with inaction. A much better way to look at it is that you will not interact with the patient at the emotional level that he or she expects. You will not interact with them in the same non-productive way that all of their friends and relatives have been interacting with them. Your goal is to complete your assessment or treatment intervention and demonstrate that they can interact in a productive way with you. I have seen some professionals get angry with patients and react emotionally and describe it to me as "reality therapy". I think that is reality insofar as the significant people in that person's life interact with them in the same way. I do not see that as providing much guidance on learning new and productive ways to interact.
5. Not getting rid of the stethoscope - Trainees are still responsible for a lot of medical work including admission histories and physicals, understanding the complex medical conditions encountered in tertiary care centers, and gathering and interpreting the medical tests and information necessary for acute psychiatric care. A big part of that is not missing an acute medical condition that needs immediate care or a medical condition that is causing the psychiatric symptoms. Some of that is learned in #3 above, but there is also an entirely different set of skills associated with medical diagnostics as it applies to psychiatry. At the minimum I would include Cardiology skills including the recognition of acute emergencies, common arrhythmias and how urgently they need to be assessed and treated, acute and ambulatory care of hypertension, and how to read electrocardiograms. All of that knowledge needs to be translated to patient care. The other areas include Neurology and the same recognition of emergencies, movement disorders especially tardive dyskinesia, but also drug induced problems. All psychiatrists should know when an electroencephalogram is useful and when to order MRI, CT, and PET imaging. I have been reading all of the imaging studies that I order throughout my career and with most electronic records systems - this seems like one of the functions that works well. As a resident you should find out where the Radiologists and Neuroradiologists hang out and ask them questions about images that seem confusing. Endocrinology and Renal Medicine knowledge has also served me well over the years. One of the most important aspects whether you are a resident or an attending is what you can learn from your colleagues. All of the consultants I have worked with have been very bright and highly motivated people. You acquire an unexpected amount of knowledge from them. To give one example, a Hematologist taught me a good way to treat sickle cell pain crises in patients with addiction to minimize their exposure to opioids. His method worked much better than the approach being used by a pain management clinic and stopped frequent admissions in inpatient units for pain crises.
6. Yes - you need to do talk therapy - I don't know how the myth started that you could be a psychiatrist and not talk to people in therapeutic ways. That is a completely unrealistic approach to the field. All of the superb psychiatrists I have known talk to their patients and have excellent skills whether that is in doing psychoanalysis or 10 or 15 minutes associated with a visit that is focused on a medication. Part of this myth seems to have originated on the inpatient side and the idea that you can't treat psychosis with psychotherapy. In fact, there are many situations in acute care where the patient may be refusing care or refusing medications and somebody needs to communicate with that person. Your life will be a lot easier as a psychiatrist if you are that person.
7. Study human consciousness - Even as a resident in the 1980s, the DSM technology had lost most of its luster when I realized that there were unrealistic categories and the application of diagnostic criteria could rarely be applied as easily as it seemed in the research. Over the years, it is even more obvious that people do not provide consistent histories over time. Some people will say that is a failing of the DSM, but it is clearly the real way that people think. You will certainly have to know the DSM and come up with DSM diagnoses in the foreseeable future, but do yourself a favor and focus at least some of your energy on how people really think. That includes knowing how human memory really works, being able to do a lot more cognitive screening than the Mini-Mental State Exam, and being able to immediately recognize the pattern of delirium from across the room. It includes knowing about complex decision making and the neurobiological substrate for those functions. It applies to how people typically think about whether or not they have any formal psychiatric diagnosis.
8. Neuroscience - This is the future of the field. There will be no demand for psychiatrists in the future who don't know brain science and how it can be applied diagnostically or therapeutically. It is the logical basis to study human consciousness, complex decision making and psychiatric disorders and contrary to what you might read on many blogs there has already been considerable progress in this area. There are many excellent psychiatrist-researchers in this area already and I encourage reading their research and some of their popular works as a starting point. There are any number of Luddites out there who seem to think that psychiatry needs to remain stagnated in the 1950s to provide any value. I don't think there is a shred of evidence to support that contention or that neuroscience will never be of value to psychiatrists. A good starting point would be to read Kandel's 1979 article on plasticity, his recent article on nicotine as as a gateway drug, and everything that he has written in between. If your department has a neuroscience section, asking them to compile a reading list of what they consider to be the top neuroscience papers that apply to the field would be an added bonus.
9. Don't be an overprescriber - When learning psychopharmacology it is tempting to consider patients to be constellations of biologically treatable syndromes. There are many problems with that approach. First and foremost is the inability to recognize the main problems in the context of a comprehensive formulation of the patient's temperament and personality. The other problems include not recognizing that a patient is unable to take a medication or tolerate it and the basic fact that in many if not most cases there is a psychosocial or psychotherapeutic approach that is on par with medications and it has fewer side effects. There are many other considerations for overprescribing and this diagram lists a few.
10. Keep yourself and everyone safe - Every resident is thrown into the breach with inadequate preparation for worst case scenarios. To prepare me, one of my attendings told me about his experience at the same hospital when he was a resident. He was called when a patient was discovered on the roof of the hospital and went sprinting up the stairway to intervene. He discovered a highly agitated patient in hospital clothing standing next to the edge of the roof. As he tried to calm him, the patient sprinted over and bit my attending on the bicep. It is hard to figure out how that breach of security could have resulted in a better outcome. The best way to be prepared is to learn to recognize warning signs and talk that over with the staff ahead of time. Work with the staff you have to come up with detailed plans to assure everyone's safety ahead of these incidents. In most training programs nobody ever discusses this problem.
11. Be a team player - On both the inpatient and outpatient side you can delude yourself into thinking that you are functioning independently and that you and your patients are in a separate parallel universe. Nothing could be further from the truth. Other staff talking about you and your behavior can have a profound effect on the kind of care that you can provide to your patients. It can also impact on your relationship with the patient directly and also on your personal safety. Think about your relationship with everyone in the treatment environment and how to keep interpersonal conflicts to the minimum. On the inpatient side, the relationships with nursing staff are critical. The worst possible scenario is a resident who develops a contentious relationship with nurses and views them as creating extra work for him or her. Part of any psychiatrists' role on the inpatient side is to make sure that no splitting occurs and that highly problematic dynamics involving staff and patients are avoided. It is good to keep in mind that the only reason patients are in a hospital setting is that they need 24 hour nursing care. They are not there to see a psychiatrist once or twice a day.
12. Know addiction inside and out - It is very tempting to take the same approach to addiction that some people take to medicine and that is: "I only practice psychiatry. This is my psychiatric diagnosis and you will have to get your addiction diagnosis and treatment plan from your addiction psychiatrist or addictionologist." This is less tenable than bailing out on medicine or psychotherapy. The reasons are fairly clear cut. Substance use disorders are major sources of differential diagnoses for primary psychiatric conditions. Substance use disorders also put people at greater risk for developing psychiatric disorders and in many cases the neurobiology of those changes is clear. Addiction and craving is also another unique conscious state with the opportunity to look at the neurobiology of complex decision making from another perspective. Most residents are also in training environments where they are responsible for the acute care and detoxification of patients with substance use problems. In many medical centers that responsibility falls to the psychiatry service.
13. See as many patients as you can see in a number of training settings - When you listen to some of the griping that happens as people complain about the number of admissions, the number of inappropriate admissions, conflicts with other medical and surgical services or just the overwhelming amount of work that accumulates it is easy to miss the big picture. The more patients you see, with more problems, the better doctor you will be in the future. At some point you will be out in practice and somebody will ask you to evaluate an acute disturbance in a patient and you will remember that immunocompromised patient you saw in a transplant unit as a resident. You may be the only one able to make that diagnosis - not based on what you read in a book but by being there as a resident.
14. Organize your study and reading around patient care and dig deep - It is easy to get lost analyzing a single case when you think about everything that involves. The pharmacology, drug interactions, drug-disease interactions, side effects, unique patient characteristics, phenomenology of the patient's symptoms and what that involves, what the patient is trying to communicate and how you can signal that you not only understand but you can suggest techniques to approach these problems are independent of medications. You are as comfortable quoting the latest treatment guidelines as the spectrum of medication side effects. A set approach to that process is useful. I typically start with Medline, add to existing collections I keep catalogued there, and read through my favorite journals. For the latest info on medical conditions I subscribe to UpToDate and keep up to date on the medical conditions that my patients have. I have a good 30 years of reference books in my library and information flagged in those books that I can't find anywhere else. My prized possession is a copy of Encephalitis Lethargica by Constantin Von Economo. That interest was based on my exposure to surviving patients with complex neuropsychiatric and movement disorders while I was still a medical student.
15. Recognize that there a lot of people out here who hate psychiatrists and that is not your problem - Any casual read through this blog illustrates the problem. The haters are deep, in multiple settings, and paying attention to them can be draining. One of the reasons this blog exists is to point out their fallacious arguments and to point out that you can do very well by not paying any attention to them. In some cases departments of psychiatry have been fooled into bringing in some of these people to give Grand Rounds as though it is a legitimate academic exercise. That is typically a mistake and it seems so unreasonable to me that I would conclude that people in that department are either incapable of critiquing them or have just run out of things to say and need speakers. Engaging most of these people is a waste of time. They have a number of fallacious arguments and the most telling factors include the fact that psychiatrists readily critique the field and do a better job. Many of the arguments provided by these groups have an obvious lack of scholarship and in some cases are over the top.
16. Recognize that conflicts of interest are everywhere - Pharmaceutical company pizza has vanished but it is no worse to me than a blogger claiming that he or she knows what is best for all psychiatrists. The critical part of residency training is to learn to critique research that impacts your patient care. I agree with Ioannidis(1) observation that almost all published research is false. I base that on my reading of medical and psychiatric research for the past 30 years. That does not mean that you don't have to know that research and how to possibly apply it. There are also critical delineations in the research literature between basic science and clinical research that nobody seems to talk about. Practically all of the focus is on imperfect clinical trials, frequently with the implication that somebody is doing something wrong. Know the difference between the appearance of conflict of interest and conflict of interest. Reviews and meta-analyses by researchers with clear agendas who are reanalyzing collections of studies are not the same as large clinical trials and generating research findings. Some of the sites that promote the review methodology do not provide much useful information for clinicians. At some point in your career you will be treating many more cases than are published in the largest clinical trials so pay attention to what you are doing. Finally know the political implications of conflict of interest including the new laws about how physicians are reported for the appearance of conflict of interest and the implications that may have for your transition into psychiatric practice. Get the opinions of your training staff on those issues.
These are a few anchor points that come to mind as I sit here typing on a Friday night. I hope that they are useful to residents. Sometimes the most basic idea takes on a great deal of importance. That is especially true when you are in a hospital at night by yourself and trying to keep the place together until sunrise. There are very few people who know what it is like to be up all night trying to figure out solutions to problems where no clear solutions exist. Make sure that you don't isolate yourself when faculty backup is available.
I can remember seeing the sun come up after many of those nights and the tremendous feeling of relief that I had made it through another night of call.
These are some of my ideas. I would appreciate the opinion of any other training staff about gems that they found most helpful in making the transition to practicing psychiatrists and avoiding land mines along the way.
George Dawson, MD, DFAPA
References:
1: Ioannidis JPA (2005) Why Most Published Research Findings Are False. PLoS Med 2(8): e124. doi:10.1371/journal.pmed.0020124
Supplementary:
1. Additional points on Advice To Residents can be found here.
Saturday, January 31, 2015
Thursday, January 22, 2015
Welcome To 1974
A colleague forwarded me a link to a newspaper article today about the latest Twin Cities managed care innovations for treating people with severe mental illnesses. It had nothing to do with managed care companies trying to save money or avoid penalties. Like most of these stories in the press there is a heavy human interest focus. The treatment details are given of a man with schizophrenia and depression who is benefitting "from a fundamental shift in the way hospitals and health plans treat people with severe mental illnesses." The author goes on to explain how social services including housing, transportation, and job training are being implemented prior to discharge and coordinated by social workers. The article suggests that the reasons for this are two fold - to prevent the "revolving door" of readmissions to the hospital and a new Medicare penalty for readmissions during the first 30 days of discharge from a hospital. The programs at a number of Twin cities hospitals are described. The Minnesota law requiring admission to a psychiatric hospital from a jail within 48 hours of commitment is also cited as a complicating factor in the large group of patients that have no stable housing, no medical or psychiatric care, substance use problems and who continue to rotate in and out of psychiatric hospitals. One of the managed care administrators describes it as a "sea change".
It turns out the "sea change" occurred in 1974. It occurred in Wisconsin and not Minnesota. That was the year that Len Stein, MD and a group of dedicated clinicians came up with the idea that patient with severe mental illnesses could be maintained outside of hospitals as long as they were provided with appropriate housing, support, and in some cases vocational services. I know because I trained under Dr. Stein. He was a personal supervisor and I did a training rotation at the Dane County Mental Health Center. I can still remember the slide from his community psychiatry presentation that showed the overcrowded conditions at the state hospital - one of the reasons behind the community psychiatry movement. My training occurred about a decade later and at that time there were three different models of care that all involved community support. The most well-known of those models is Assertive Community Treatment or ACT. I was well versed in these models and providing the necessary care and for the first three years out of training I was the medical director at a community mental health center and spent have of my time working with the community support team. That team provided crisis services and support on a 24/7 basis to patients with severe mental illnesses. That was 30 years ago.
After the community mental health center, I moved to the Twin Cities where I spent the next 23 years working in a metropolitan hospital primarily running an inpatient unit. My focus for the first 10 years was trying to get people interested in community support services for patient we were discharging to the community. At first, there was a patchwork of public health nursing and large housing units with nursing supervision for our discharged patients. But eventually there was nothing. I was told point blank by various administrators that they really were not interested in hearing how things worked in Wisconsin. They did things differently in Minnesota. When I could no longer ask public health nurses to check on discharged patients - there was no help for them at all, except for an appointment to see a psychiatrist if they did not forget it.
That changed slightly when the state decided to shut down state hospital bed capacity and one of the psychiatrists there was able to get funding for ACT teams. The rationale by the state was that some of the money to maintain state hospital beds would be diverted to the ACT teams. Eventually that initiative increased but there was still not enough capacity. There was still a large patient population without adequate housing or assistance. The economic plight of many of these people was worsened by "spend down" provisions implemented by the state. That meant that even though their income was 100% disability payments, they could be expected to pay up to 60% of it for medications. That typically meant that the person went from poverty status to worse in order to continue recommended medications for their psychiatric disability.
Another problem was the bed situation and approaches that were being used to manage those beds. That last half of my inpatient career, there was a continuous large pool of patients flooding Twin Cities emergency departments. That resulted in initiatives to admit and discharge as soon as possible. The entire focus of admissions and discharges was on "imminent dangerousness" even though there is no such legal standard. It was a business standard of care. Many people seeking admission because they were miserable realized this and said they were suicidal in order to get admitted. Conversely, many people who still had significant problems and no good way to resolve them were discharge because they no longer met the "imminent dangerousness" criteria. There were no quality approaches to care only a focus on rapid discharges of very ill people.
So I have to shake my head when I read about the "new" approach to treating mental illness and helping people to maintain themselves in the community. There is really nothing here that was not done in Wisconsin nearly 40 years ago. In the meantime there is a severely deteriorated infrastructure with fewer beds in both designated hospitals but also supportive housing. I have significant doubts about the funding of these services since we know that managed care companies don't do community support services. Who is paying for these social workers and psychologists? Will they have to submit billing documents that are not practical to complete? Even if they are being paid for by the state, that doesn't necessarily guarantee future funding. At one point all of the public health nurses I was working with in the 1980s were told they could no longer see patients with psychiatric problems. And what about the continued rationing by managed care companies now being made to look like it is innovation?
Welcome to 1974.
George Dawson, MD, DFAPA
Chris Serres. Strategies shift for treating mental illnesses. Star Tribune January 19, 2016.
Tuesday, January 20, 2015
Stakeholders? I Don't Think So.
 |
| Stakeholder Relationships |
I don't know when I first heard the term. My guess is that it was about 15-20 years ago. I am sure that it came up during a meeting about "productivity expectations" and contract negotiations. In case you missed it productivity is a grand concept courtesy of the US Government and managed care industry. It was designed to get doctors to work a lot more for lot less. Increased regulatory leverage against physicians was an added bonus. If you happen to be a psychiatrist the reimbursement as indicated in some of my early posts can be trivial. That is all before a managed care company or the government steps in and makes a totally subjective determination based on documentation that enough bullet points may not have been covered to justify a particular billing code. In that case the penalties range from incarceration in federal prison (yes I was in a seminar where that was the message) to a managed care company deciding that you need to pay them back by adjusting your codes to lower levels and demanding reimbursement. Say what you want about physicians, the natural question is how a group of fairly bright people end up in such a hapless position? I have had lawyers confide in me that they would never accept the kind of harassment and financial manipulations that have been forced on physicians. I suppose arguments have been made by politicians that it should be an accepted condition by physicians, especially those who sign on for government programs for the most needy. Practicing medicine is after all a privilege right?
A lot of it comes down to boundaries. I tried to illustrate these boundaries in the diagrams at the top of this post. In the diagram at the top, the boundaries are fairly porous. Looking back at how the important medical organizations sold some of these concepts to their members and continue to sell them today, it usually involves somebody hitting the panic button and someone suggesting that the solution is the next great idea from a business consultant or politician. History illustrates that we have followed a long road of nonsolutions for the past 30 years. The reason for that has been obvious to me. Professional organizations frequently allow the government and the industry and their ideas direct access to the highest levels of governance in our organizations and the solutions from these special interest groups follow. The special interests are often in the form of a person or persons who happen to be true believers and may coincidentally have some employment arrangement or guru role with business or government. The entire scheme of rationing medical and psychiatric services to improve the bottom line of insurance companies is the best case in point. After all, what comes out of the intersection of the three spheres in the top diagram? The "cost effective" rhetoric for one. Every President of the American Psychiatric Association (APA) or the American Medical Association (AMA) at some point utters these words and these words are included in documents of most APA District Branches. We are living in a time when we have the worst infrastructure and systems of treatment for psychiatric and substance use problems in the last 30 years. People are no longer adequately treated in psychiatric hospitals. State hospital systems are in shambles. County jails and state prisons have become places to house people with severe mental illnesses. Outpatient clinics are placing more people than ever on generic antidepressants based on a rating scale score. Medications are both over and under prescribed based on the lack of expertise and the lack of infrastructure necessary for detoxification, social interventions and psychological treatments. The term cost effective should no longer be used by any psychiatrist or professional organization. We should have started spending more money on treating severe mental illnesses about 20 years ago.
What happens if we remove the term cost-effective from the top diagram of muddled boundaries where the administrators in all organizations essentially say the same thing? In the lower diagram we can actually hear the people in each sphere saying different things. It is possible for physicians to say for example that across the board cost cutting is the tool of incompetent administrators. It is possible for psychiatrists to say that over time various incentives seem to have been in place that favored all specialties over time except psychiatry. It is possible for physicians to say that there is a huge gap between the care that governments are funding and what professional standards really are. It is possible for psychiatrists to say that the way state hospitals are managed by government bureaucrats is hideous and that somebody with knowledge of staff dynamics and patient safety needs to be administering these places - not somebody with no training. All of these things are possible if there is an actual boundary between the professional organization and the government and their friends in the business community.
I know that there are plenty of skeptics out there in the physician community. I am not even interested in what the business people or politicians/regulators have to say because of conflict of interest considerations. I also left out the professional boards including the American Board of Medical Specialities (ABMS) and the American Board of Psychiatry and Neurology for the same reasons - no boundaries and plenty of conflicts of interest. The skeptics out there who I would like to address are the physicians just like me. We go to work every day and know it is a hard job made a lot harder by all of the other so-called stakeholders.
If a clearer example is needed, allow me to direct you to what appears to be a cooperative effort between the professional organizations and Medicare involving their pay-for-performance initiative (see paragraphs 6 and 7). That initiative is based on Physician Quality reporting System (PQRS) that requires physicians to report on a number of measure beginning in 2015 in order to avoid penalties. The reporting is for the obvious convenience of fulfilling the political promise of being able to "compare" physicians on a series of unvalidated measures. This page on the APA web site is off-putting enough for anyone who has actually read it. The APA has deactivated a link that would bring the reader to a 50+ page document written by psychiatrists on quality markers for major depression. The links to that document are currently gone and a comprehensive list of the 2015 PQRS individual measures are not yet available. The APA and AMA have clearly been cooperative with these efforts. The message to individual clinicians is the same - we will waste as much of your time on unreimbursed paperwork to satisfy our collective political arrogance as we want. These measures are an insult to any working person. Instead of paying physicians to generate this data, the government's approach is to penalize physicians if the data is not collected and that penalty increases from 1.5% this year to 2% next year on the worst reimbursement source for physicians. It should not be surprising that psychiatrists are rapidly shifting to different methods of reimbursement.
When I got home tonight, I was greeted by a letter from the AMA notifying me that my membership had expired. It proceeded to tell me what I was missing if I did not renew:
"Full access to online toolkits for working with Physician Transparency Reports (Sunshine Act) and managing HIPPA requirements for your practice.
Our detailed guides to help you navigate employment contract negotiations with hospitals and groups ($149 each, free to members)"
There are probably no better reasons to not renew the membership. In all three cases, the boundary-less relationships with the federal government and the managed care industry have created these unnecessary burdens. Like most organizations without boundaries the AMA has found a way to cash in on the new regulatory landscape that they failed to protect their members from in the first place. Their expired membership notification is an insult to any dedicated member of the profession.
It is time to rewrite the relationship between medical professional organizations and the other so-called stakeholders. Nobody should have a stake in a profession except those who have paid their dues in time, energy, personal sacrifice and finances and the people who seek their services. It is time to realize that there are no benefits to a "place at the table" especially when political fees paid by physicians are basically mocked in Washington compared with the businesses who continue to exploit us.
George Dawson, MD, DFAPA
Monday, January 19, 2015
How Should APA Guidelines Work?

The guidelines of the American Psychiatric Association (APA) are an interesting story in how guidelines are important if used correctly by professional organizations. The whole idea behind a profession is that the practitioners in that area have special expertise and that the expertise is standardized to some degree. Standardization is useful in the case of physicians to assure the safety of the practitioners and so that people have some idea of what to expect in terms of safe and effective care. Over a decade ago the APA began producing guidelines for practice in various areas of the field. I thought it was an exciting development. The guidelines were initially sent along with the monthly copy of the Journal of the American Psychiatric Association. All of the guidelines are available publicly on this web site, but hardly anyone knows about them. I make this statement because one of the many red herrings that the critics of psychiatry use is that psychiatry has no standards of care. They seem quite shocked to find that these guidelines exist and address their complaints directly.
I was asked to critique one of the existing guidelines and suggest how these guidelines could be used more effectively. In looking at the guidelines web site, it is apparent that some of the guidelines have not been updated in quite a while. Publication dates range from 2000 - 2010. Given the pace of clinical research 5 years might be somewhat acceptable, but 10 - 15 is probably not. Another issue that the APA needs to grapple with is the diagnostic manual versus treatment approaches. There is widespread confusion about whether or not the DSM-5 is a guidebook for treatment as opposed to a guidebook for diagnoses. The APA actually two approaches to treatment guidance - the guidelines themselves and a text entitled Treatment of Psychiatric Disorders (TPD). TPD is currently in its 4th edition and it has gone from a series of two volume detailed text to a more basic single volume text. That text was published in 2007. Some of the chapters in the previous editions provide some of the most detailed information on the pathophysiology and treatment of certain disorders that could be found anywhere. At that level of analysis, the APA has gone from providing outstanding information on the pathophysiology and treatment of psychiatric disorders to a relative vacuum over the past 10 years.
For the purpose of a more detailed analysis I will consider the Practice Guidelines on Substance Use Disorders and the associated Quick Reference Guide and Guideline Watch - a 2007 update of the original 2006 guideline. I looked at the Guideline Watch first because it should reflect the latest literature reviews and treatment guidelines. The document reviews medication assisted treatment of tobacco and alcohol use disorders with varenicline, naltrexone and acamprosate. The document was a good summary of the literature at the time but it needs a serious update. Since then there have been more extensive studies of the genetics, combination therapies, re-analysis of existing studies and side effects of naltrexone, acamprosate, and varenicline including use in specific psychiatric populations. In at least one case, the current literature supports a course of action that is exactly the opposite of what is recommended in this document. That course of action is: " Given its high potency and partial agonist activity at central nicotinic acetylcholine receptors, varenicline should not be combined with alternate nicotine replacement therapies." An inspection of the references for varenicline notes that additional research has been done in this area and should be discussed.
The Quick Reference Guide contains extensive tables from the original guideline so I will go directly to that document. At first glance it looks like a significant document more than 200 pages long. But about 177 of the 276 pages of the document are relevant text. The rest are references and polls of various expert groups on what they consider necessary for a guideline. Looking at the Table of Contents, the first thing that is apparent is that only a subset of substance use disorders is being considered. Although it is likely that nicotine, alcohol, marijuana, cocaine and opioids represent the majority of abused substances psychiatrists treating addiction see a broader array of compounds being abused. The full gamut of abused compounds should probably be addressed in the guideline whether or not there is a consensus about treatment methods or not. The safety of users and treatment setting considerations will still need to be considered as well as the need for further assessments. A good example would be Hallucinogen Persisting Perceptual Disorder and what might be the best assessment and treatment. If the guidelines are supposed to apply to clinical practice then patterns encountered in clinical practice need to be addressed. If the APA does not address them - governments and managed care companies will, most frequently to the detriment of patients.
The guideline uses the following conventions for the treatment recommendations. They are conventions frequently see in professional guidelines:
[I] Recommended with substantial clinical confidence.
[II] Recommended with moderate clinical confidence.
[III] May be recommended on the basis of individual circumstances.
The introductory section does not suggest who the guidelines are written for. This is a critical aspect of the document. There is an implication that it is for psychiatrists based on the statement about a comprehensive psychiatric evaluation but I think that needs to be more explicit. It is not uncommon for managed care companies to send letters that deny care to psychiatrists. The letter often contains a list of guidelines that an insurance company reviewer used to deny the care. The APA needs to be explicit that these guidelines are intended for use by the psychiatrist who has personally assessed and is treating the patient and not by an insurance company employee or contractor who is sitting in an office reading through paperwork. Somewhere along the line professional organizations seem to have lost track of the concept that only direct assessment and treatment of the patient was considered the correct way to do things. Putting it in all guidelines is a critical first step.
The next thing I would change in terms of guidelines is breaking out the treatment setting recommendations into separate sections in table form. For example the Hospitalization guidelines are copied into the Supplementary section of this post. They are all very appropriate and I doubt that there are any reasonable clinicians that would have a problem with them. The problem is that these services are rationed to the point that it is difficult for any reasonable clinician to implement them. By that I mean that a psychiatrist cannot get a patient meeting these criteria into an inpatient detox or treatment setting based on these criteria. As an example, consider the patient who says they are drinking 1 liter to 1.75 liters of vodka per day for 6 months. They describe uncomplicated symptoms of alcohol withdrawal (shakes, sweats, hangover symptoms and drinking in the morning to suppress these symptoms). I think the person in this vignette meets criteria 2 for hospitalization and detox at least. A significant number of patients presenting to emergency departments with this pattern of findings are not hospitalized. Many are sent out with a supply of benzodiazepines to detoxify themselves. Many are sent to county detox facilities where there is no medical coverage or so-called social detoxification settings. None of these non-hospitalization options are realistic approaches to the problem. Giving a person with an alcohol use disorder a bottle of benzodiazepines for home detox ignores the uncontrolled use and cross addiction aspects of the primary disorder. It is highly likely that person will ingest the benzodiazepines all at once or use them to treat the morning withdrawal symptoms of the disorder. Social detoxification is an equally suboptimal approach. It depends on probabilities. It is more likely that the person transferred to that setting will leave due to the adverse environment and go back to drinking or undergo withdrawal and not experience delirium tremens or withdrawal seizures. Over the past 30 years, the managed care industry has refused to consider admissions in practically all of these situations often whether there was psychiatric comorbidity or not resulting in the rationing of care at the initial assessment in the Emergency Department. There must be an awareness that clinical guidelines don't operate in a vacuum. Having a guideline in place that nobody can use is not the best approach to providing quality care. Managed care companies can deny inpatient care on practically any of the 7 inpatient criteria simply by saying that they do not exist.
On the treatment side there are inconsistencies noted in the recommendations and editing problems. For example, there are 49 references to "12-step" and 2 references to 12 steps. One of the first statement one encounters is: "The efficacy of treatment is related to the amount of psychosocial treatment received. The 12-step programs, hypnosis, and inpatient therapy have not been proven effective." That characterization of 12-step recovery is inconsistent with just about every other reference in the document. Where it is suggested it is footnoted with a "I" designation or "substantial clinical confidence."
Rather than critique other sections based on data that was not available at the time that this guideline was posted, I thought I would end with a comment on the process and general philosophy of professional guidelines. Right at the top of this guideline is a section entitled "Statement of Intent". The crux of that argument is contained in the paragraph (p. 5):
"The American Psychiatric Association (APA) Practice Guidelines are not intended to be construed
or to serve as a standard of medical care. Standards of medical care are determined on
the basis of all clinical data available for an individual patient and are subject to change as scientific
knowledge and technology advance and practice patterns evolve. These parameters of
practice should be considered guidelines only. Adherence to them will not ensure a successful
outcome for every individual, nor should they be interpreted as including all proper methods
of care or excluding other acceptable methods of care aimed at the same results........"
I don't really agree with that approach. The concerns about saying that these are standards of care is a medico-legal one and I have rarely found that to be a sufficient basis to practice medicine. An example would be litigation against a psychiatrist for not following the stated standards of care in a malpractice suit. This may seem protective of psychiatrists for varying practice styles but it also has the more insidious effect of basically allowing any standard of care to apply. A walk down the street to a different hospital results in an admission for medical detoxification when the first hospital discharges the patient with a prescription of lorazepam and a promise to follow up with their primary care MD. The resulting business incentive practice creep results in a complete lack of detoxification and a lack of any standards of medical care. The default standard is whatever businesses decide to pay for. My observation is that results in an unacceptable level of medical care. And further:
"The ultimate judgment regarding a particular clinical procedure or treatment plan must be made by the psychiatrist in light of the clinical data presented by the patient and the diagnostic and treatment
options available....."
I agree with the statement but let's face it, the judgment of the psychiatrist frequently has very little to do with the judgment of the psychiatrist or what options are ultimately considered in the working alliance with the patient. Practically all inpatient and residential care these days is dictated by managed care companies and insurance companies irrespective of what a psychiatrist would recommend or a patient would accept. These are standards of care that are forced on psychiatrists and patients rather than the prospective quality based standards.
Stepping back from that fact medical standards play a peripheral role to what businesses want and that unacceptable standard has been present to one degree to another for the past 30 years, I don't think a new approach in guidelines is too much to ask for. I don't think it is too much to ask that APA guidelines be up to date, internally consistent, inclusive, actually apply as a standard of care as opposed to using business standards as the default, and be used to advocate for the best possible treatment settings for psychiatrists and their patients. There are a number of specific methods that can be used and I will discuss them when the draft version of the latest Practice Guidelines for the Psychiatric Evaluation of Adults comes out this year.
George Dawson, MD, DFAPA
References:
Work Group On Substance Use Disorder. Practice Guideline For TheTreatment of Patients WithSubstance Use Disorders, Second Edition. American Psychiatric Association. This practice guideline was approved in December 2005 and published in August 2006.
Supplementary 1: These are the hospitalization guidelines from the APA Substance Use Disorders Guideline.
"Hospitalization is appropriate for patients who
1) have a substance overdose who cannot be safely treated in an outpatient or emergency department setting
2) are at risk for severe or medically complicated withdrawal syndromes (e.g., history of delirium tremens, documented history of very heavy alcohol use and high tolerance);
3) have co-occurring general medical conditions that make ambulatory detoxification unsafe;
4) have a documented history of not engaging in or benefiting from treatment in a less intensive setting (e.g., residential, outpatient);
5) have a level of psychiatric comorbidity that would markedly impair their ability to participate in, adhere to, or benefit from treatment or have a co-occurring disorder that by itself would require hospital level care (e.g., depression with suicidal thoughts, acute psychosis);
6) manifest substance use or other behaviors that constitute an acute danger to themselves or others;
or
7) have not responded to or were unable to adhere to less intensive treatment efforts and have a substance use disorder(s) that endangers others or poses an ongoing threat to their physical and mental health [I]." (p. 11).
Objectivity? A Role For Emotion In Decision Making
One of the reasons I like listening to Public Radio is that they provide a lot of clinicopathological case material that is usually quite illustrative, and frees me from the huge hurdle of being suspected of disclosing confidential patient information on this blog. Just a note on the historical context. When I started out, deidentified clinical information was a mainstay of teaching. It was presented at case conferences and in medical journals. At some point that became a lot less likely and in my opinion that adversely affects teaching in a way that could be dangerous to the health of patient. The best physicians depend on pattern matching to recognize diseases and many of those patterns are recalled not just from live patients but also pictures, images, and numbers that are remembered independent of any real contact with a live patient. When an administrator did not allow me to use deidentified MRI scan images for teaching residents, those residents end up knowing a little bit less, not in terms of book learning but in terms of the experiential aspects of medicine. The most unique technical skill that your physician has that nobody else does is access to a vast array of patterns that were experienced in medical school and post graduate training.
I was driving around today, listening to public radio when a show came on called Radiolab. I have heard it before and it is interesting because it tried to present science in interesting ways and in many cases that involves medicine. Today's show was all about choices and I happened to pick it up about 1/3 of the way in or roughly the 20 minute mark. At that point Antoine Bechara, MD, PhD began discussing the case of Elliot, a young accountant. Elliot was working for a corporation as a successful upper level manager. He was married and had children. He was considered to be smart, successful, and religious. One day a small tumor was discovered in his orbitofrontal cortex and it was successfully removed. Post surgical neuropsychological testing showed that was still in the 97th percentile in terms of IQ testing. He returned home and then went back to work.
What occurred following the successful neurosurgery was unexpected. He was no longer able to make even routine decisions. As an example, when he tried to decide what pen to use to sign a contract, it took him 30 minutes to decide whether to use a black pen or a blue pens. All possible permutations of the decision were explored and evenly considered. In the case where many more choices were available (the program used the example of a breakfast cereal aisle in the grocery store), the decisions became more impossible. He was so disabled by this problem that he lost his job and eventually his marriage and family. He got involved with a con man. He lost his savings and went back to live with his parents. Somewhere along the way he was seen by the behavioral neurologist Antonio Damasio, MD, PhD who tested him with visual stimuli designed to elicit strong emotional responses. These visual stimuli failed to elicit these responses in the patient. Damage to his orbitofrontal cortex had caused this disconnection. Disconnecting the emotional response resulted in an impairment in decision making rather than an expected improvement. Without the feeling state he was pathologically indecisive.
When I heard Dr. Bechara talking I remembered an excellent presentation that he gave on how people with addictions tend to respond to the Iowa Gambling Task (GT) and how some responses in that paradigm are consistent with increased risk for substance use. This test looks at subjects attempts to optimize a $100 bet on choices from 4 decks of cards (A, B, C, and D). The subject is to make 100 card selections in any order from any of the decks. A selection from deck A or B results in a $100 reward. There are unpredictable punishments so that the subject loses $1250 in every 10 cards selected from deck A or B. Selections from decks C and D result in a $100 reward with unpredictable punishments resulting in a loss of $250 in every 10 cards from decks C and D. The penalties are not fixed and some of them are substantial. Take a look at this video for an example of how it works (the initial sum used in the video is substantially higher than quoted in the research literature). Normal subjects eventually learned that they are more likely to get punished choosing from decks A and B and they will gravitate toward decks C and D. The Iowa group used this test paradigm and modifications to investigate aspects of decision making in the ventromedial prefrontal (VM) cortex (bilateral lesions to the gyrus rectus, mesial half of the orbital gyrus and the inferior half of the medial prefrontal surface).
Subjects with lesions in the VM do not reduce their selection of decks A or B or increase their selection of choices in decks C and D. The impairment in decision making can be replicated over time. In order to investigate whether any emotional process was involved, the investigators looked at skin conductance resistance (SCR) associated with the decisions. They looked at a window of +/- 5 seconds on either side of the decision to examine anticipatory, reward and punishment SCRs. Normal subjects develop anticipatory SCR and they are more pronounced before selections from the disadvantageous decks (A and B). Even the 20% of normal subjects who are self professed risk takers develop anticipatory SCRs but they are lower in magnitude when selecting for the disadvantageous versus advantageous decks. VM subjects had no anticipatory SCR suggesting that these patients had a compromised ability to change their somatic state (skin conductance) in anticipation of an imagined scenario in an uncertain condition.
The researchers also looked at the question about whether biases in this paradigm were conscious or not. The experiment in this case used the same decks A, B, C, and D but the task was broken up into 4 different zones. The subject was asked about their explicit knowledge of what was happening in the game after every 10 cards. The 4 periods included:
1. Pre-punishment period before encountering punishment.
2. Pre-hunch period as punishment was being encountered by the subjects till had no ideas about the game.
3. Hunch period where guesses about favorable decks begin to appear.
4. Conceptual period when they have a clear idea about the advantageous versus disadvantageous decks.
In normal subjects the SCRs were absent pre-punishment but began to build and was sustained. Although 30% of controls never got to the conceptual periods they all had SCRs and played the game correctly. 50% of VM subjects got to the conceptual stage in that they could explicitly state the deck types. That did not result in them correcting their choices. In real life this means the patient with frontal lobe damage has an awareness of what is right and what is wrong but the correct choice is not made. The authors use the example of a person with a substance use disorders balancing the choice between taking a drug as an immediate reward and the long term reward of a stable home, family and work life they choose the drug. The GT has been used to study the issue of substance users and impairment in decisions is noted.
The wiring and impact of various signaling systems on the vmPFC is complex. It is hard to imagine methods that would allow the isolation and correlation of any of these systems suggested in the clinical vignette about the patient with the brain tumor. The neuroanatomy is also complex. Many of us were taught to consider the supraorbital area of frontal cortex to be typical frontal cortex, It turns out that the most medial gyri that represent the vmPFC and are more appropriately considered limbic cortex. Looking at a recent post on the involvement of the nucleus accumbens in decision making now provides two avenues for advancing decisions - emotions and reward pushing these decisions forward.
Apart from psychiatric disorders and addictions, these brain systems have profound implications for everyday life and the illusion of free will. Many of the biases in everyday life that many of us would deny that we have, may be the product of the reward and/or emotional valence assigned to that string of associations through these mechanisms. Many of these biases are unconscious. I think there is widespread confusion that emotions compromise objectivity (as in rational decision making). One of the main outcomes of these studies is that emotions are necessary make a decision and do not necessarily compromise the rational aspects of that decision. The other approach I see written about is the idea that there is a reptilian brain lying deep inside the human brain and this has a characteristic response pattern (anger/rage). It was popular to talk about reptilian brains when I first learned neuroanatomy, but a lot less was known about the integration of the human brain at that time.
George Dawson, MD, DFAPA
References:
I was driving around today, listening to public radio when a show came on called Radiolab. I have heard it before and it is interesting because it tried to present science in interesting ways and in many cases that involves medicine. Today's show was all about choices and I happened to pick it up about 1/3 of the way in or roughly the 20 minute mark. At that point Antoine Bechara, MD, PhD began discussing the case of Elliot, a young accountant. Elliot was working for a corporation as a successful upper level manager. He was married and had children. He was considered to be smart, successful, and religious. One day a small tumor was discovered in his orbitofrontal cortex and it was successfully removed. Post surgical neuropsychological testing showed that was still in the 97th percentile in terms of IQ testing. He returned home and then went back to work.
What occurred following the successful neurosurgery was unexpected. He was no longer able to make even routine decisions. As an example, when he tried to decide what pen to use to sign a contract, it took him 30 minutes to decide whether to use a black pen or a blue pens. All possible permutations of the decision were explored and evenly considered. In the case where many more choices were available (the program used the example of a breakfast cereal aisle in the grocery store), the decisions became more impossible. He was so disabled by this problem that he lost his job and eventually his marriage and family. He got involved with a con man. He lost his savings and went back to live with his parents. Somewhere along the way he was seen by the behavioral neurologist Antonio Damasio, MD, PhD who tested him with visual stimuli designed to elicit strong emotional responses. These visual stimuli failed to elicit these responses in the patient. Damage to his orbitofrontal cortex had caused this disconnection. Disconnecting the emotional response resulted in an impairment in decision making rather than an expected improvement. Without the feeling state he was pathologically indecisive.
 |
| Major Anatomical Connections of the Ventral Medial Prefrontal Cortex from: Euston DR, Gruber AJ, McNaughton BL. The role of medial prefrontal cortex in memory and decision making. Neuron. 2012, figure 3 with permission. |
When I heard Dr. Bechara talking I remembered an excellent presentation that he gave on how people with addictions tend to respond to the Iowa Gambling Task (GT) and how some responses in that paradigm are consistent with increased risk for substance use. This test looks at subjects attempts to optimize a $100 bet on choices from 4 decks of cards (A, B, C, and D). The subject is to make 100 card selections in any order from any of the decks. A selection from deck A or B results in a $100 reward. There are unpredictable punishments so that the subject loses $1250 in every 10 cards selected from deck A or B. Selections from decks C and D result in a $100 reward with unpredictable punishments resulting in a loss of $250 in every 10 cards from decks C and D. The penalties are not fixed and some of them are substantial. Take a look at this video for an example of how it works (the initial sum used in the video is substantially higher than quoted in the research literature). Normal subjects eventually learned that they are more likely to get punished choosing from decks A and B and they will gravitate toward decks C and D. The Iowa group used this test paradigm and modifications to investigate aspects of decision making in the ventromedial prefrontal (VM) cortex (bilateral lesions to the gyrus rectus, mesial half of the orbital gyrus and the inferior half of the medial prefrontal surface).
Subjects with lesions in the VM do not reduce their selection of decks A or B or increase their selection of choices in decks C and D. The impairment in decision making can be replicated over time. In order to investigate whether any emotional process was involved, the investigators looked at skin conductance resistance (SCR) associated with the decisions. They looked at a window of +/- 5 seconds on either side of the decision to examine anticipatory, reward and punishment SCRs. Normal subjects develop anticipatory SCR and they are more pronounced before selections from the disadvantageous decks (A and B). Even the 20% of normal subjects who are self professed risk takers develop anticipatory SCRs but they are lower in magnitude when selecting for the disadvantageous versus advantageous decks. VM subjects had no anticipatory SCR suggesting that these patients had a compromised ability to change their somatic state (skin conductance) in anticipation of an imagined scenario in an uncertain condition.
The researchers also looked at the question about whether biases in this paradigm were conscious or not. The experiment in this case used the same decks A, B, C, and D but the task was broken up into 4 different zones. The subject was asked about their explicit knowledge of what was happening in the game after every 10 cards. The 4 periods included:
1. Pre-punishment period before encountering punishment.
2. Pre-hunch period as punishment was being encountered by the subjects till had no ideas about the game.
3. Hunch period where guesses about favorable decks begin to appear.
4. Conceptual period when they have a clear idea about the advantageous versus disadvantageous decks.
In normal subjects the SCRs were absent pre-punishment but began to build and was sustained. Although 30% of controls never got to the conceptual periods they all had SCRs and played the game correctly. 50% of VM subjects got to the conceptual stage in that they could explicitly state the deck types. That did not result in them correcting their choices. In real life this means the patient with frontal lobe damage has an awareness of what is right and what is wrong but the correct choice is not made. The authors use the example of a person with a substance use disorders balancing the choice between taking a drug as an immediate reward and the long term reward of a stable home, family and work life they choose the drug. The GT has been used to study the issue of substance users and impairment in decisions is noted.
The wiring and impact of various signaling systems on the vmPFC is complex. It is hard to imagine methods that would allow the isolation and correlation of any of these systems suggested in the clinical vignette about the patient with the brain tumor. The neuroanatomy is also complex. Many of us were taught to consider the supraorbital area of frontal cortex to be typical frontal cortex, It turns out that the most medial gyri that represent the vmPFC and are more appropriately considered limbic cortex. Looking at a recent post on the involvement of the nucleus accumbens in decision making now provides two avenues for advancing decisions - emotions and reward pushing these decisions forward.
Apart from psychiatric disorders and addictions, these brain systems have profound implications for everyday life and the illusion of free will. Many of the biases in everyday life that many of us would deny that we have, may be the product of the reward and/or emotional valence assigned to that string of associations through these mechanisms. Many of these biases are unconscious. I think there is widespread confusion that emotions compromise objectivity (as in rational decision making). One of the main outcomes of these studies is that emotions are necessary make a decision and do not necessarily compromise the rational aspects of that decision. The other approach I see written about is the idea that there is a reptilian brain lying deep inside the human brain and this has a characteristic response pattern (anger/rage). It was popular to talk about reptilian brains when I first learned neuroanatomy, but a lot less was known about the integration of the human brain at that time.
George Dawson, MD, DFAPA
References:
1: Radiolab: Choice
2: Bechara A, Damasio H, Damasio AR. Role of the amygdala in decision-making. Ann N Y Acad Sci. 2003 Apr;985:356-69. Review. PubMed PMID: 12724171. From a special ediction of the journal called: THE AMYGDALA IN BRAIN FUNCTION: Basic and Clinical Approaches
2: Bechara A, Damasio H, Damasio AR. Role of the amygdala in decision-making. Ann N Y Acad Sci. 2003 Apr;985:356-69. Review. PubMed PMID: 12724171. From a special ediction of the journal called: THE AMYGDALA IN BRAIN FUNCTION: Basic and Clinical Approaches
3: Bechara A, Damasio H, Damasio AR. Emotion, decision making and the
orbitofrontal cortex. Cereb Cortex. 2000 Mar;10(3):295-307. Review. PubMed PMID:
10731224. This is from a special edition of this journal called: The Mysterious Orbitofrontal Cortex
4: Euston DR, Gruber AJ, McNaughton BL. The role of medial prefrontal cortex in memory and decision making. Neuron. 2012 Dec 20;76(6):1057-70. doi: 10.1016/j.neuron.2012.12.002. Review. PubMed PMID: 23259943; PubMed Central PMCID: PMC3562704.
Supplementary 1:
Figure 3 above was reprinted from Neuron, Vol. 76 edition number 6, Euston DR, Gruber AJ, McNaughton BL. The role of medial prefrontal cortex in memory and decision making, Copyright (2012), with permission from Elsevier. License # 3542200221086 License date Jan 04, 2015 per the Copyright Clearance Center.
Supplementary 2:
I use the following human neuroanatomy text by Paxinos and Mai with the accompanying Atlas of the Human Brain by Jürgen K. Mai, Joseph Assheuer, and George Paxinos. It was recommended to me by Lennart Heimer after I took one of his courses in brain dissection at Washington University. I requested permission from the publisher to use some of these figures for teaching purposes and the fees were astronomical. So the text and atlas are primarily useful to clarify your own thinking rather than preparing presentations.

4: Euston DR, Gruber AJ, McNaughton BL. The role of medial prefrontal cortex in memory and decision making. Neuron. 2012 Dec 20;76(6):1057-70. doi: 10.1016/j.neuron.2012.12.002. Review. PubMed PMID: 23259943; PubMed Central PMCID: PMC3562704.
Supplementary 1:
Figure 3 above was reprinted from Neuron, Vol. 76 edition number 6, Euston DR, Gruber AJ, McNaughton BL. The role of medial prefrontal cortex in memory and decision making, Copyright (2012), with permission from Elsevier. License # 3542200221086 License date Jan 04, 2015 per the Copyright Clearance Center.
Supplementary 2:
I use the following human neuroanatomy text by Paxinos and Mai with the accompanying Atlas of the Human Brain by Jürgen K. Mai, Joseph Assheuer, and George Paxinos. It was recommended to me by Lennart Heimer after I took one of his courses in brain dissection at Washington University. I requested permission from the publisher to use some of these figures for teaching purposes and the fees were astronomical. So the text and atlas are primarily useful to clarify your own thinking rather than preparing presentations.

Tuesday, January 13, 2015
JAMA Psychiatry Suicide Article, Statistics and AI
 |
Suicide Rates - Selected OECD Countries |
Suicide is a very important problem for psychiatrists. Even though it is a rare event, it seems like most of our time is focused on preventing suicide. There are many days where many high risk patients and patients with chronic suicidal ideation are seen in clinics and hospitals. Most of them are treated in outpatient settings and very few are treated on an involuntary basis in hospital settings. Since suicide is diametrically opposed to self preservation it is assumed that any rational person would want to get help with those thoughts and impulses. Like most things in psychiatric practice it is almost never than simple. Psychiatrists encounter a wide range of of reasons for suicidal thinking. At times, the suicidal thinking was not obvious until it was declared after a suicide attempt. Many people decide to see psychiatrists after a first suicide attempt. Even at that point it is common to find a person who is disappointed that they did not succeed. It is more common to find a person greatly relieved that they survived but even then that does not assure the cooperation necessary to prevent another attempt.
The standard of practice for assessing suicidal thinking or ideation and potential risk is risk factor analysis. This has been the standard of practice for as long as I have practiced over the past 30 years. To do this analysis, it requires making a diagnosis or a series of diagnoses and looking at associated factors and how the patient describes his/her mental state at the time. Major psychiatric diagnoses like major depression, schizophrenia, bipolar disorder, panic disorder, borderline personality disorder and chronic substance use disorders all have significant lifetime prevalences of suicide varying from 3 to 15%. Psychological autopsies of series of suicides find that nearly all of the patients who have suicided in these studies had a significant psychiatric disorder. There are also studies done from a social science perspective that emphasize the social risk factors for suicide including sex, martial and relationship status, economic factors and loss.
Suicide is a widely misunderstood problem sometimes even for the patients who are experiencing the thoughts. It is common for example to encounter people with suicidal thinking who say that their only deterrent to suicide is that they don't "have the guts" to do it. An associated worry might be that it is "too painful." They feel a need to explain why they cannot carry out an irrational act. I take this to mean that at some point in time, the suicidal person's conscious state has changed. They are no longer a rational person and that is why they must explain away the fact that they cannot carry out an irrational act. Another common observation that speaks to the conscious state is that many people will say "I never understood how a person could be suicidal until I finally felt that way." That suggests that the altered conscious state is associated with a mood state of depression or many times a mixture of depression, anger, and anxiety resulting in an agitated state that led to the understanding about suicidal thoughts. A final observation is one of the most stressful parts of psychiatric practice and that is: "Can I believe this person when they tell me they are not going to kill themselves?" Much of acute care psychiatry hinges on that ultimate question. The risk factor analysis is essentially nullified if the patient is in an emergency department and their diagnosis and past suicide attempts are known. The only thing left to go on are the standard questions about current state of mind, deterrents, safety plans and whether the person seems reliable and says they will not kill themselves. It is widely known that people kill themselves after leaving emergency departments and hospitals. People have killed themselves in hospitals while under direct observation.
Many of these assessments become adversarial. By the time a psychiatrist sees a patient in a hospital, a lot has already happened. In all of the hospitals where I have practiced, crisis teams, paramedics, and the police have assessed the person in the community and brought them in to the hospital. Very few people were under psychiatric care at the time of that intervention. Friends and family members of the patient were the people who called the first responders. The patient is usually there out of some concern for their welfare that they may not be aware of. The psychiatrist comes around sometime in the next 24 hours and the interaction unfolds. Very few people seem interested in the fact that they might kill themselves. Getting out of the hospital may be the priority. Their approach might be one of non-disclosure or denial: "I really did not say I was suicidal." or "I did not mean it", or "I was drunk or high at the time". Even those responses can vary from very unlikely (as in a patient with a serious self inflicted gunshot wound) to unlikely (a patient with delusional depression stopped in the midst or a suicide attempt) to possible (the intoxication history with no suicidal ideation while sober). The interview dynamic is also quite variable. A person may be sullen, irritated, and not wanting to discuss much information. They may express concerns about self incrimination: "I know what I can and cannot say to psychiatrists. I know if I say the wrong thing you will lock me up and throw away the key." They may blame their problems on the psychiatrist: "Look - I know you don't care about me. The only thing you care about is covering your ass. You are going to do whatever you want to do." They may be more hostile and sarcastic: "Look if I was really going to kill myself I wouldn't be sitting here talking to you. I'd be dead. I wouldn't be talking about it."
All of these statements ignore the fact that the person is sitting in front of the psychiatrist as the result of the actions of several other people including persons affiliated with them and having their best interests at heart. That situation is so intense and uncomfortable that it prevents physicians from going into psychiatry. I have had many physicians tell me they could not go into psychiatry because: "Guessing about whether or not a person will kill themselves is too stressful." There are many ways to reduce the guesswork involved but the point I am trying to make here is that all of these behaviors are consistent with the patient having undergone a change in their conscious state. They are no longer acting like a person interested in self preservation, but they are now a person who is contemplating self destruction and taking active measures to hide that thought pattern. That is the main reason why psychiatrists can't predict suicide over long periods of time with any degree of certainty. When a person's conscious state changes that completely, their actions are less predictable even to the point that they may be potentially self destructive and want to cover it up.
That is also why risk factor analysis is so imperfect. In the case of the diagnosis, a lot of clinicians are under the impression that if a person satisfies some written criteria for a diagnosis that provides a lot of critical information about the potential for suicide. Many clinicians seem to miss the point that a patient can have the exact same written criteria for major depression with psychotic features and the same chronic markers on a suicide risk assessment and suddenly be much more likely to attempt suicide. The only thing that has changed has been the patient's conscious state and their awareness that suicide is an unwanted state. The evidence that this happens is clinical and ample. Patients will report back to their psychiatrists that they were in this conscious state and the psychiatrist did or did not miss it. Either way, there is no clinician in this situation who could make the correct call. Without any clear markers, there is no way to figure out if this change in conscious state has occurred. The patient usually recognizes it only in retrospect.
This clinical information on the assessment of suicide is what makes this JAMA Psychiatry article interesting. In this article the authors attempt to determine predictors of suicide by soldiers in the year following psychiatric hospitalization within the Veteran's Administration hospital system over a 6 year period. That was a total of 40,820 hospitalizations or 0.9% of the total Army personnel in any 12 month period. During that time there were a total of 68 deaths by suicide. That is number is 12% of all US Army suicides. The authors consider a long list of potential risk factors that are largely demographic in nature to determine concentration of risk of suicide. That list includes a law enforcement data base that clinicians do not have access to. Their overall goal was to determine of it was practical identify high risk patients for post hospitalization intervention and whether that might be a cost effective way to prevent suicide. They were able to identify the highest risk group - the 5% of hospitalizations in which 52.9% of the suicides occurred. Like many similar studies the authors also comment on how their "actuarial" methods usually trump clinicians making the same predictions. I found very limited commentary on that fact that it is generally possible to illustrate what you want with enough variables or as we used to say "a large enough spreadsheet". In this case they looked at a large number of variables to come up with 421 predictors for further analysis. I have reviewed hospital records consisting of the printout of the electronic health record where there were scarcely 421 words and it was usually impossible to determine an admission or discharge date. Any information on even a short term assessment of suicide risk is scant and it frequently says basically that the patient told us he or she was not going to make a suicide attempt. In some cases a rating scale approach like the Columbia is used. Clinicians using these scales are often surprised about how few variables change after the initial rating and how the numerical risk does not necessarily reflect an inpatient versus and outpatient population.
As I read through the article, I was also impressed with the amount of alien statistics and fairly esoteric statistical terms. If JAMA Psychiatry wants to include these methods, I think an example of the calculations and a bibliography of additional reading would be a minimal requirement. The addition of statistical reviewers' comments or an independent statistical discussion of the pros and cons of these methods would only enhance the quality of the discussion. One of my concerns is that as the statistical methods get more abstract and vague notions about big data are more accepted, clinical complexity and wisdom are completely diluted down and out. I saw a headline the other day that Internet sellers know more about your "personality" than your spouse. It should be fairly obvious from all of the healthcare research done that is based on HEDIS (The Healthcare Effectiveness Data and Information Set) information, that demographic variables and product choices are not the same thing as clinical assessment and treatment.
If the headlines about artificial intelligence replacing doctors ever comes true, it will only happen if the machine can implement the required knowledge. The performance of computers sifting through text based findings and diagnostic criteria has been know for 20 years (reference 3). Those data points were generally far superior to demographics. I owned 2 of those programs and they don't bother to sell them anymore. In terms of the assessment and treatment of suicide a knowledge base included in the Harvard Medical School Guide To Suicide Assessment and Intervention might be a step in the right direction. A lot of that knowledge depends on the skill of a particular clinician and that includes the personality factors of clinicians who continue to do this impossible job day after day.
Trying to predict suicide and prevent it can't currently be done with an algorithm. If I see an algorithm I will consider why the high risk people aren't being seen in follow up from the hospital rather than who should get an intervention. And I would not mind errors on the false positive side.
George Dawson, MD, DFAPA
1: Kessler RC, Warner CH, Ivany C, Petukhova MV, Rose S, Bromet EJ, Brown M 3rd, Cai T, Colpe LJ, Cox KL, Fullerton CS, Gilman SE, Gruber MJ, Heeringa SG, Lewandowski-Romps L, Li J, Millikan-Bell AM, Naifeh JA, Nock MK, Rosellini AJ, Sampson NA, Schoenbaum M, Stein MB, Wessely S, Zaslavsky AM, Ursano RJ; Army STARRS Collaborators. Predicting Suicides After Psychiatric Hospitalization in US Army Soldiers: The Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS). JAMA Psychiatry. 2015 Jan 1;72(1):49-57. doi: 10.1001/jamapsychiatry.2014.1754. PubMed PMID: 25390793.
2: Douglas G. Jacobs, editor. Harvard Medical School Guide To Suicide Assessment and Intervention. Jossey-Bass Inc., San Francisco, CA, 1998.
3: Berner ES, Webster GD, Shugerman AA, Jackson JR, Algina J, Baker AL, Ball EV,Cobbs CG, Dennis VW, Frenkel EP, et al. Performance of four computer-based diagnostic systems. N Engl J Med. 1994 Jun 23;330(25):1792-6. PubMed PMID: 8190157.
3: Berner ES, Webster GD, Shugerman AA, Jackson JR, Algina J, Baker AL, Ball EV,Cobbs CG, Dennis VW, Frenkel EP, et al. Performance of four computer-based diagnostic systems. N Engl J Med. 1994 Jun 23;330(25):1792-6. PubMed PMID: 8190157.
Sunday, January 11, 2015
Hand Washing
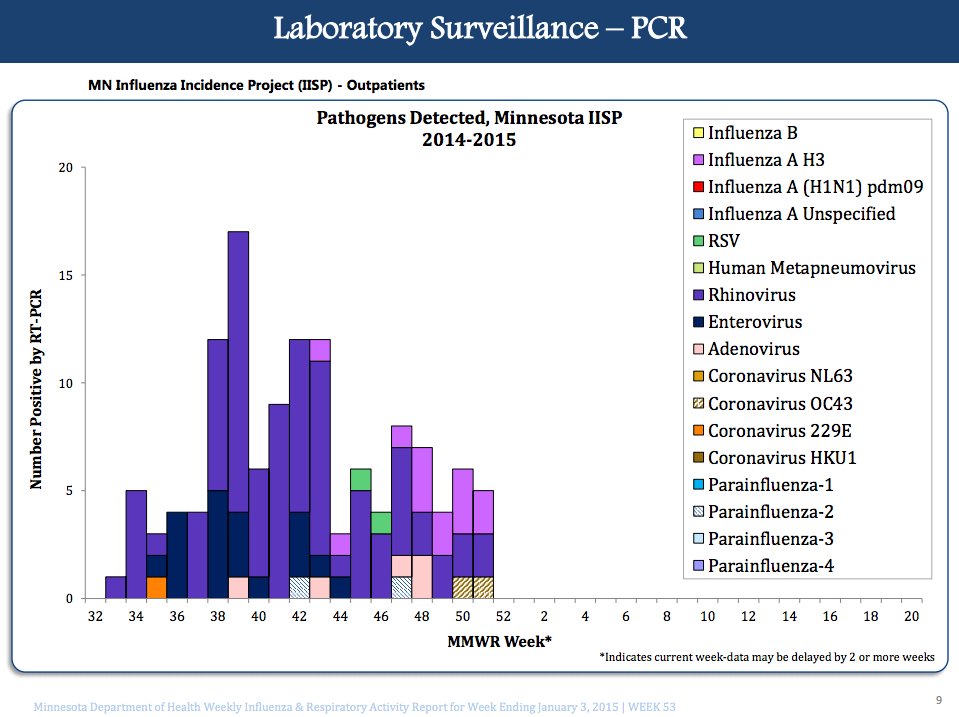
I washed my hands 40 times yesterday and used disinfectant hand cleaner at least 10 times when I did not have immediate access to water and soap. My hand washing technique was validated by an infection control nurse who was trained to monitor appropriate hand washing. I also wiped down the table in my office and the chair about 3 times with disinfectant wipes. I am careful not to touch my food or my face. I have an air cleaner running in that office from about 8AM to 6PM that has a UV lamp designed to kill viruses. Despite all of that I am in day #5 of a flu-like illness (cough, myalgias, fatigue, but no fever).
I don't have obsessive compulsive disorder. I live in Minnesota and it is peak season for the annual influenza epidemic. I actually take more precautions. During flu season, I avoid the public. I used to belong to a gym, but set up my basement so I could do my workout routine at home. Exercise equipment is a known reservoir of viruses and bacteria. I have also been in a gym when it sounded more like a hospital ward due to the hacking and coughing. I avoid movie theaters for the same reason. I have been doing these same rituals for the past twenty years, initially because I thought I was allergic to influenza vaccine and did not want to catch the flu. I have been fairly successful in avoiding the flu, but not so successful in avoiding practically every other respiratory virus. For twenty three years I worked in an old building that was designed to contain heat rather than clear respiratory viruses. In that environment, once a virus is introduced there is a predictable epidemic (sometimes within a few days) affecting the entire staff. Modern employment disincentives (the finite paid time off with no sick time system) keeps all of the ill people working. They would rather work than lose vacation time. That keeps the epidemic going.
Throughout the flu season people at risk are told the same things. Wash your hands, cough into your sleeve, stay at home if your are ill and get the flu shot. Unfortunately all of these measures is not enough to prevent infection by airborne viruses. Face masks help. A study of college dormitory dwellers showed that hand washing and wearing a mask only offered modest protection against influenza like illness relative to a control group. They used the term modest, but I would call about a 10% difference in infection rates weak at best. In their study they looked at three groups of students in college dormitories. The groups and the attack rates of flu-like illness (FLI) included controls (no intervention) 117/552, face mask only 99/378, and face mask and hand hygiene 92/367. The authors tried to control as many measures as possible but there are a lot of reasons why experimenting on college students is problematic. In terms of the basic methods hand washing or use of hand disinfectants is considered to have a small but significant effect on the transmission of respiratory viruses. The effectiveness of masks depends on the fit of the mask, the physical characteristics of the environment and the virus itself. One study (4) showed that a tightly sealed N95 respiratory mask would block 94.8% of influenza virus and a poorly fitting mask blocked only 56.6% of the virus.
The process of creating infectious droplets is an interesting physical process. There are current estimates that show normal breathing for 5 minutes creates a few droplets through the process of atomization. A single strong nasal expiration results in a few hundreds droplets with a few in the 1-2 µm in diameter. Counting loudly creates a few hundred droplets in the 1-2 µm range. A single cough produces a few thousand and a single sneeze produces a few hundred thousands to a few million 1-2 µm droplets that can contain viral particles. There is a a video of what happens to those millions of sneeze generated particle in an airplane. It might be a good place to wear a mask but that assumes that you have it on before the sneeze. Atomization can also occur from vomit (107 viral particles per ml) and feces (1012 viral particles per gram). Those routes of transmission have been important for SARS and Norwalk Like Viruses.
The most recent estimate of costs due to building influenced communicable respiratory infections was about $10 billion in direct treatment costs and indirect costs of $19 billion in lost productivity and $3 billion in performance losses. Asthma is significantly affected and possibly caused by airborne respiratory viruses and that is another $18 billion in costs ($10 billion direct and $8 billion indirect). My interest has been in trying to promote more attention to the problem especially at the environmental levels. Just altering airflow characteristics or making other changes in the humidity and air temperature can reduce the infectivity rates by as much as 50%. Apart from the cost, it has an immeasurable effect on employee morale. It is difficult for anyone to work knowing that at least one month out of the year they will have significant symptoms of a respiratory syndrome.
Why did I post this and in particular on a psychiatry blog? In my 23 years of inpatient experience, respiratory viruses plagued the staff and the patients we were treating. Any attempt I made to change that from a non-medical environmental perspective was met with no response. I think that is the standard response of our culture and most employers. Mental health settings tend to be located in older buildings and older parts of health care campuses and respiratory viruses is likely a bigger problem. Health care settings should be leaders in developing environments and infrastructure that is hardened for the airborne respiratory virus problem. It is imperative as a healthy environment for workers and patients and it provides reserve capacity in the event of a more widespread pandemic. I have also made some observations about the impact of FLI on psychiatric symptomatology - both improvements and worsening. There is a increasing literature on the effect of cytokine signaling on brain function and I suspect that is what I was seeing, but more research is needed.
In the meantime, keep washing your hands. Keep in mind that this post is only about airborne infections. Any physician with direct contact with patients needs to wash their hands after seeing a patient and before seeing the next patient. Most hospitals have a rule that hand washing needs to occur every time a physician enters or leaves a room. For airborne respiratory viruses, it is not enough but it decreases the risk of respiratory infections to a slight degree. My guess is that the more highly infectious airborne viruses are much less containable with hand washing and that environmental measures involving airflow, relative humidity, and possibly filtration and UV sterilization is what is required. Anyone planning new construction should focus on these measures and obtain appropriate heating and air conditioning consultation with an emphasis on reducing respiratory infections.
George Dawson, MD, DFAPA
References:
1: Aiello AE, Murray GF, Perez V, Coulborn RM, Davis BM, Uddin M, Shay DK,Waterman SH, Monto AS. Mask use, hand hygiene, and seasonal influenza-like illness among young adults: a randomized intervention trial. J Infect Dis. 2010 Feb 15;201(4):491-8. doi: 10.1086/650396. PubMed PMID: 20088690.
2: Verreault D, Moineau S, Duchaine C. Methods for sampling of airborne viruses. Microbiol Mol Biol Rev. 2008 Sep;72(3):413-44. doi: 10.1128/MMBR.00002-08. Review. PubMed PMID: 18772283; PubMed Central PMCID: PMC2546863.
4: Noti JD, Lindsley WG, Blachere FM, Cao G, Kashon ML, Thewlis RE, McMillen CM, King WP, Szalajda JV, Beezhold DH. Detection of infectious influenza virus in
cough aerosols generated in a simulated patient examination room. Clin Infect
Dis. 2012 Jun;54(11):1569-77. doi: 10.1093/cid/cis237. Epub 2012 Mar 29. PubMed
PMID: 22460981.
5. ASHRAE (American Society of Heating, Refrigerating, and Air-Conditioning Engineers) ASHRAE Position Document on Airborne Infectious Diseases Approved by ASHRAE Board of Directors January 19, 2014 Expires January 19, 2017. - This is an interesting approach that looks at how to look at engineering approaches to airborne infectious particles and come up with a better approach.
Supplementary 1: Various inhalers used over the past year following a probable rhinovirus exacerbation of asthma in January of 2013. This is a rapid way to meet your annual deductible.

Supplementary 2: Graphic of pathogens detected per week is from the Minnesota Department of Health web site.

Supplementary 2: Graphic of pathogens detected per week is from the Minnesota Department of Health web site.
Thursday, January 1, 2015
2015 and......

I was going to try to post about alcohol consumption prior to New years Eve, but am still working on that post. Instead, I found myself reacting to a post on LinkedIn entitled "10 Warning Signs That Your Psychiatrist Is Not A Good Fit" by Amanda Itzkoff, MD. Look for it on LinkedIN if you are a member and see what you think. I found it fairly stark and negative. I found myself immediately typing up my own top ten list on how you know you have found a competent psychiatrist. That may not fit the usual blogger message that critical statements that apply to only a few is the only reason for commentary. One of my reasons for writing this blog is that the tremendous number of colleagues who I personally know are all very competent and the list is a composite of what anyone would find walking in to talk with any one of them. That list follows.
I had thought about posting a list of what I plan to continue to do here in the coming year but decided that was unnecessary. You can certainly go to any number of blogs to find out what is wrong with psychiatry or psychiatrists. Much of it is hyperbole. I hope that you will find what I write here is a realistic antidote to those other sites.
Top Ten Signs Your
Psychiatrist Is Competent
1. You are understood.
Your psychiatrist makes it very clear to you that he/she understands the problem and all of the
mitigating factors by formulating the problem and treatment plan, restating it
to you, and giving you useful advice.
That also includes discussing the relationship that you have with the
psychiatrist and any concerns that you have about it. That is one aspect of seeing a psychiatrist
that differs from seeing other physicians.
You should be comfortable bringing up any concerns and clarifying any
potential misunderstandings. Your
psychiatrist should also be able to answer the basic question about whether you
have any diagnosis or problem that requires treatment. Your psychiatrist should be focused on a
discussion of your problems and your best interest should be the focus of
treatment.
2. Your psychiatrist is an expert.
Your psychiatrist has
technical expertise in the field and is comfortable discussing new treatments
and innovation in the field ranging from psychotherapy to brain science. That includes an awareness of the current
limitations of treatment.
3. Your psychiatrist knows medicine.
During the initial
assessment and beyond, your psychiatrist pays close attention to any other
medical problems that you have and how the treatment he/she prescribes might
affect those conditions. That includes
being able to diagnose new medical conditions that can lead to psychiatric
presentations and ordering the appropriate tests to follow potential
complications of any new treatments or how new treatments might impact existing
conditions. That includes a willingness
and an ability to talk with the other generalists and specialists providing
your medical care.
4. Your psychiatrist takes enough time.
The assessment and
treatment of complicated problems takes time.
Many psychiatrists are in clinics where there are allowed only brief
periods of time (10 to 20 minutes) for assessment and treatment. Many people are satisfied with that amount of
time, but if you are not - a different treatment setting may offer more time. That can be discussed with the current
psychiatrist and a referral to psychiatrists practicing in different settings
can be obtained.
5. If medications are involved your psychiatrist thoroughly explains the risks, benefits, and limitations of treatment.
Like most areas of
medicine, medical treatments have their limitations. That includes medications that are not
completely effective in alleviating symptoms, side effects, and occasional very
serious side effects. Your psychiatrist
should be able to help you negotiate that area and provide you with more
detailed information for further study on request. You should believe that your psychiatrist is
taking any concern you have about side effects very seriously. The discussion of side effects is as
important as a discussion of potential therapeutic effects. Any informed discussion of medical treatment
should also include a discussion of non-medical approaches. Many people are surprised to learn than
non-medical approaches are more effective than medications in the treatment of
several severe mental health problems.
6. Your psychiatrist knows about addiction.
A significant number of
people being treated by psychiatrists have problems with addiction. Addiction can cause psychiatric problems and
complicate the care of psychiatric problems.
Even if your psychiatrist is not an addiction specialist, he/she should
be able to advise you in how to get well and not increase the risk for relapse
if you are sober. Your psychiatrist
should also be able to advise you in approaches to your problems if you are not
sober. Chronic pain is also an
associated problem and your psychiatrist should be able to make an assessment
of your chronic pain problem and how it affects associated mental health and
addiction problems.
7. Your psychiatrist is able to tell you about
things that you do not want to hear.
That can cover a broad
range of topics from your expectations about medication and psychotherapy, to
unrealistic expectations, to boundary problems involving what appear to be
straightforward problems like filling out a disability form. One example would be concerns about a
diagnosis of Attention Deficit-Hyperactivity Disorder (ADHD). A lot of adults seek treatment for this
problem and in many cases they are also expecting an approach that leads to
enhanced cognition. A consulting
psychiatrist should be able to say that they do not have ADHD and that
stimulant medications are not currently indicated for cognitive enhancement.
8. Your psychiatrist is concerned about your
safety.
One of the
characteristics of some mental health problems is that the safety of the person
involved is compromised. Psychiatrists
are trained to make these assessments and determine a plan to address the
problem. Many psychiatric disorders
result in impaired insight and judgment that is restored once the primary
problem is treated. It is often useful
to have a discussion about that in advance.
Some states have a psychiatric advanced directive that is useful to
direct your care in the event of an acute episode of illness that affects your
judgment. We live in a litigious society
and physicians are often accused of “covering” themselves by making very conservative
decisions. These decisions are most
likely driven more by safety concerns than malpractice concerns.
9. Your psychiatrist is willing to talk with
your family.
You should be certain
that your confidentiality is protected at all times per an explicit agreement
with your psychiatrist. That agreement
should include emergency contingencies and advise you about the statutes in
your state that affect confidentiality.
You should also expect that when you want your psychiatrist to talk with
your family that he/she will do that.
For certain aspects of treatment planning such as discharge planning
from hospitals and gathering diagnostic information, discussions with family
are critical.
10. Your psychiatrist is mindful of your
financial concerns.
Mental health services
are the most rationed services in medical care in the US. That typically results in more out-of-pocket
costs for people receiving psychiatric care than other types of medical or
surgical care. Your psychiatrist should
be able to discuss the cost aspects of all forms of care. That includes medication costs and also the
cost of ongoing psychotherapy. Cost effective alternatives for both
psychotherapy and medical assessment and treatment should be as easily
discussed as any other aspect of treatment.
Your psychiatrist is often placed in an impossible situation by the
insurance industry. The insurance
industry often makes it seem like your psychiatrist is responsible for decisions
that are really the result of insurance industry rationing. Any concerns you have about the financial basis
for decisions should be clarified with your psychiatrist.
Happy New Year!
George Dawson, MD, DFAPA
Subscribe to:
Posts (Atom)