Well I suppose it is slightly better than the usual characterizations that we see in the New York Times, but David Brooks recent column on the "improvisation, knowledge and artistry" involved in psychiatry is little more than damning with faint praise. His flaws include using the term "technical expertise" and comparing psychiatry to "physics and biology". Psychiatry is certainly comparable to biology but not to physics. And what is it about psychiatry that is unscientific? The idea that psychiatry seeks to legitimize itself by appearing to be scientific is a popular antipsychiatry theme. It is probably why many authors seek to equate psychiatry with the DSM. The science of psychiatry is out there in many technical journals that are scarcely ever mentioned in the public commentary about psychiatry. The idea that the science of psychiatry is collapsed into a modest (at best) diagnostic manual is a convenient way to deny that fact and portray psychiatrists as unscientific and perhaps not very much like physicians either.
Brooks characterization of the DSM shows a continued lack of understanding of this manual by every journalist who writes about it. There is practically no psychiatrist I know of who considers it to be authoritative. Very few psychiatrists actually go about their diagnostic business by reading through DSM criteria. That activity would be limited to novices and medical students. It is well known that only a fraction of the diagnoses listed are ever used in clinical practice. After familiarizing themselves with the major changes, few psychiatrists will every open it again. Like most physicians, psychiatrists are looking for patterns of illness that are based more on their clinical experience than criteria listed in a manual. The idea that this text has "an impressive aura of scientific authority" is certainly consistent with Brook's thesis, but that is not what a psychiatrist experiences when looking at it. Despite all of the concern about the public impact - psychiatrists are the target audience here. Psychiatrists are much more aware of the limitations of the approach than the media critics who write about it. I guess a lay person might be impressed, but I never met a psychiatrist who was.
Brooks is also confused about the nature of the DSM when he states that it contains "a vast body of technical knowledge that will allow her (your psychiatrist) to solve your problems". That vast body of technical knowledge is firmly outside of the DSM and it is in the form of training and ongoing education of a psychiatrist. That technical knowledge is contained in a vast literature, much of it written by psychiatrists. It is the reason that ongoing training and education of physicians is a career long commitment. In the general scope of things, the DSM would contribute a percentage point or two at most to that body of knowledge.
There is the associated question about whether physicians are scientists or not. I have seen Kandel himself interviewed about this issue and he states quite definitely that they are not. That is quite different from suggesting that physicians are unscientific. There are certainly not many physicians who are performing scientific experiments and publishing papers. I suppose that you have to do that to be a professional scientist. On the other hand, physicians are certainly accountable for learning immense amounts of of scientific principles and data that can be applied in clinical situations and used in critical thinking about patients and teaching it to successive generations of physicians.. I teach Dr. Kandel's plasticity concept and how it applies to addictions in about 30 lectures a year. Reducing scientific knowledge to "artistry" is really inconsistent with "technical expertise". There really is no art in medicine. The most technically competent doctors know the science, have seen more patterns of illness and can recognize those patterns. They can apply that knowledge to patient care. In complex medical (and psychiatric) care, a special plan can be designed for each individual patient and most aspects of that plan are rooted in science.
This essay strains under the weight of needing to place psychiatry outside of the scope of science and mainstream medicine. My study of psychiatry finds it in neither of those locations. There is a reason that psychiatrists need to go to medical school. The cross section of basic science and clinical science that all physicians are exposed to is necessary to be a psychiatrist. Using Brooks reasoning, I suppose he could say that this is just an effort to "legitimize" psychiatry by making it seem like it is on scientific par with the other fields of medicine. When I am face to face with a severely ill patient who has liver disease, heart disease, diabetes, alcoholism and a refractory psychiatric disorder - the science involved is much more than a political exercise.
Like every other branch of medicine, psychiatry is an amalgam of the clinical and basic sciences. Biology especially neuroscience but also the anatomy and physiology of the human body is the central focus. I will give Brooks partial credit when he writes about the DSM. Unlike many of his colleagues at the NY Times - he does not refer to it as a "Bible". When it comes to the issue of whether I am a scientist or not, I certainly realize that I am no Eric Kandel. But I also know that I am not rolling the dice or taking a leap of faith. I am doctor seeing people, trying to understand their unique set of problems, and applying medical science to help them get better.
George Dawson, MD. DFAPA
David Brooks. Heroes of Uncertainty. NYTimes May 27, 2013.
Thursday, May 30, 2013
Monday, May 27, 2013
Suggested Changes to Psychiatric Residency Programs
I received an e-mail two weeks ago that asked for my suggestions on immediately reforming residency programs for psychiatry. I had the experience of completing my residency in two different university based programs. My residency occurred at the height of the controversy between the self described biological psychiatrists and the psychotherapists and psychoanalysts. Although I have never seen it written about there was open animosity between the groups at times. A biological psychiatrist back in the day might make a statement like: "I don't do talk therapy". A psychotherapy oriented psychiatrist might refer to the biological types as "Dial twisters" referring to an approach that suggested excessive biological reductionism. Apparently neither group had read Kandel's seminal article in the New England Journal of Medicine four years earlier and how plasticity can be affected by talking, medications, and of course other experiences.
Several years ago, I attended an anniversary of the University of Wisconsin Department of Psychiatry, the program I eventually completed my residency at. Thomas Insel, MD was one of the invited speakers. He outlined a revolutionary approach to educating psychiatry residents that involved a joint 2 year neuroscience internship with residents from neurology and neurosurgery. He did not provide any details. When I sent him a follow up e-mail two years later, he said it would probably not happen on his watch. I can easily build on that theme. I think that a two year program focused on basic and clinical neuroscience remains a good approach. The current approach to getting the relevant information is haphazard at best. It depends on lectures in neuroscience being interspersed with clinical rotations of varying quality and to a large extent it depends on the faculty. How many faculty are there and how many of them are expected to produce managed care style billings or "productivity" rather than high quality teaching.
A comprehensive and integrated approach that will teach state of the art neuroscience and provide the relevant training in neurology and medicine is possible. There are many obvious areas for improvement. Residents often spend their time on clinical rotations of minimal relevance for psychiatrists. I can recall learning ICU medicine and needing to familiarize myself with various tasks (Swan-Ganz catheters, central lines, ventilator settings, dopamine drips, balloon pumps) that I would never use again. I needed to be seeing hundreds of people with heart disease, arrhythmias, hypertension, diabetes, other endocrine disorders and neurological disorders. I saw many of those people when they were hospitalized, but seeing these folks in ambulatory care settings designed to enhance the learning experience for a psychiatrist would provide a better experience. The process should probably start earlier in the fourth year of medical school. Prospective psychiatrists should be focused on electives in neurology, medicine, and neurosurgery rather than psychiatry.
The teaching of psychiatry needs to address the practical concerns about diagnosis and treatment but also philosophical concerns. Residents need to be familiar with the antipsychiatry philosophy and the existing literature that refutes it. Residents need to know about the issue of the validity and reliability of psychiatric diagnoses and how that is established. There is actually a rich history of how that came about but it could easily be summarized in one seminar. One of the features that I was interested in when I was interviewing for residency positions was whether or not the program supplied a reading list. There were surprisingly few that did. This subject area would be a good example of required reading that is necessary to bring any prospective resident up to speed.
A good model to illustrate the difference between a neuroscience based approach as opposed to a symptoms based approach is American Society of Addiction Medicine (ASAM) definition of addiction on their web site. Unlike the DSM collection of symptoms designed to pick a group of statistical outliers, the ASAM definition correlates known addictive behaviors with brain substrates or systems. Both of the standard texts in the field by Lowinson and Ruiz and the ASAM text by Ries, Feillin, Miller, and Saitz are chock full of neuroscience as it applies to addiction. When I teach those lectures, I generally am talking about how medications work in addiction at that level but also how psychological and social factors work at the level of neurobiology. I have not seen the DSM5 at this time, but I do think that it is time to move past defining every possible substance of abuse and associated syndrome and incorporating neuroscience. Especially when the neuroscience in this case has been around for 50 years. Residency programs need to teach that level of detail.
Several years ago, I attended an anniversary of the University of Wisconsin Department of Psychiatry, the program I eventually completed my residency at. Thomas Insel, MD was one of the invited speakers. He outlined a revolutionary approach to educating psychiatry residents that involved a joint 2 year neuroscience internship with residents from neurology and neurosurgery. He did not provide any details. When I sent him a follow up e-mail two years later, he said it would probably not happen on his watch. I can easily build on that theme. I think that a two year program focused on basic and clinical neuroscience remains a good approach. The current approach to getting the relevant information is haphazard at best. It depends on lectures in neuroscience being interspersed with clinical rotations of varying quality and to a large extent it depends on the faculty. How many faculty are there and how many of them are expected to produce managed care style billings or "productivity" rather than high quality teaching.
A comprehensive and integrated approach that will teach state of the art neuroscience and provide the relevant training in neurology and medicine is possible. There are many obvious areas for improvement. Residents often spend their time on clinical rotations of minimal relevance for psychiatrists. I can recall learning ICU medicine and needing to familiarize myself with various tasks (Swan-Ganz catheters, central lines, ventilator settings, dopamine drips, balloon pumps) that I would never use again. I needed to be seeing hundreds of people with heart disease, arrhythmias, hypertension, diabetes, other endocrine disorders and neurological disorders. I saw many of those people when they were hospitalized, but seeing these folks in ambulatory care settings designed to enhance the learning experience for a psychiatrist would provide a better experience. The process should probably start earlier in the fourth year of medical school. Prospective psychiatrists should be focused on electives in neurology, medicine, and neurosurgery rather than psychiatry.
The teaching of psychiatry needs to address the practical concerns about diagnosis and treatment but also philosophical concerns. Residents need to be familiar with the antipsychiatry philosophy and the existing literature that refutes it. Residents need to know about the issue of the validity and reliability of psychiatric diagnoses and how that is established. There is actually a rich history of how that came about but it could easily be summarized in one seminar. One of the features that I was interested in when I was interviewing for residency positions was whether or not the program supplied a reading list. There were surprisingly few that did. This subject area would be a good example of required reading that is necessary to bring any prospective resident up to speed.
A good model to illustrate the difference between a neuroscience based approach as opposed to a symptoms based approach is American Society of Addiction Medicine (ASAM) definition of addiction on their web site. Unlike the DSM collection of symptoms designed to pick a group of statistical outliers, the ASAM definition correlates known addictive behaviors with brain substrates or systems. Both of the standard texts in the field by Lowinson and Ruiz and the ASAM text by Ries, Feillin, Miller, and Saitz are chock full of neuroscience as it applies to addiction. When I teach those lectures, I generally am talking about how medications work in addiction at that level but also how psychological and social factors work at the level of neurobiology. I have not seen the DSM5 at this time, but I do think that it is time to move past defining every possible substance of abuse and associated syndrome and incorporating neuroscience. Especially when the neuroscience in this case has been around for 50 years. Residency programs need to teach that level of detail.
Psychiatrists need to maintain superior communication
skills relative to other physicians and that means getting a good
basic experience in interviewing and psychotherapy techniques. At the
same time - the psychiatrist of the future needs to be able to order and interpret
tests including ECGs and MRI scans. That wide skill base taxes every faculty except the very largest academic departments. In the Internet age, there is really no reason that every residency program should not have access to the same standardized PowerPoints, lectures, and didactic material. The ASCP Model Psychopharmacology Program is an excellent example of what is possible. I would go a step beyond that and say that there should be a culture within organized psychiatry so that every psychiatrist should have access to the same material. Establishing a culture where everyone (trainees and practicing psychiatrists alike) is up to speed and competent across the broad array of topics that psychiatrists need to be familiar with is a proven approach that is rarely used in medical education.
Psychiatry also needs to be focused on old school quality. Not the kind of quality that depends on a customer satisfaction survey. The issues of diagnostic assessment and appropriate prescribing at at the top of the list. How do we make sure that every person consulting with a psychiatrist gets a high quality evaluation and treatment plan and not a plan dictated by a managed care company? The University of Wisconsin has a paradigm for networking with all physicians in their collaborative Memory Clinics program. I see no reason why that could not be extended to different diagnostic groups across the state. The focus would be on quality assessment and to prevent outliers in terms of treatment. It could be open to any psychiatrist who wanted to join and it could have additional benefits of providing university resources like online access to the medical library to clinicians in the field.
An interested, excited, and technically competent psychiatrist is the ultimate goal of residency and it should continue throughout the career of a psychiatrist. That can only happen with a focus on professionalism at all levels. My definition of professionalism does not include managing costs so that a managed care organization can make more money. Psychiatrists need to forget about being cost effective and get back to defining and providing the best possible care.
George Dawson, MD. DFAPA
Saturday, May 25, 2013
The Real Role of Biological Tests in Psychiatry
The idea of a "biological test" in psychiatry has appeared on the internet recently, primarily as a way to deny that psychiatric disorders exist. The contention is that because there is no medical test for a psychiatric disorder - it must not exist. Time to add a balanced view.
As a backdrop, most people do not understand the concept of "tests" in medicine until they have a problem and realize that the problem is not reflected in the tests ordered by their doctor. That is a very common experience. Some studies show that up to 30% of patients presenting to a clinic for investigation of a symptom never find out what the cause of that symptom was. That is true even after they were given the usual panel of blood tests, imaging studies, and electrophysiological studies. The assumption that symptoms and disorders in medicine are all diagnosable by a "test" is incorrect.
The second problem occurs at the level of test interpretation. When a doctor orders a test they have to interpret it correctly and in many cases the idea of an "abnormal" test is blurred by biological variation. The evaluation of back pain using imaging studies like MRI scans is a good case in point. As people age there is a greater likelihood that an abnormal MRI scan of the spine is not necessarily the cause of their back pain. That has very important implications for treatment and the physician interpreting the test may will definitely be influenced by their specialty training, their own personal experience, their knowledge and examination of the patient, and possibly treatment guidelines that they may be mandated to follow. There is also the question of false positive and false negative testing. The recent controversy about the utility of prostate specific antigen (PSA) testing for prostate cancer is another good example. The current guideline says that this test has too many false positive results to use for treatment planning and further invasive procedures. Even in the case where the diagnosis is made by a specific number there is always the question of whether the test number is accurate or not. I have frequently repeated thyroid function tests that seemed to show hyperthyroidism only to see them in the normal range on repeat testing. It is obvious to physicians that the so-called biological tests in medicine have their limitations and always need to be interpreted in the context of a comprehensive evaluation of the patient.
How are biological tests currently used in psychiatry? It turns out that there are a lot of applications similar to the rest of medicine.
1. To detect a medical cause of a psychiatric disorder. The DSM classification has an entire set of disorders that are caused by underlying neurological illnesses, endocrine disorders, and infectious diseases that need to be recognized and treated. They often present as psychiatric disorders. In my experience of treating people with severe problems, up to 15% of the psychiatric presentations had an underlying medical illness that either was a direct cause of the "psychiatric" symptoms or it made a psychiatric disorder worse. In that case the psychiatrist has to be trained to order the appropriate tests, make the diagnosis and refer the patient for treatment of the underlying disorder.
2. To screen for medical illnesses that complicate the psychiatric disorder or its treatment. A good example here is screening blood tests and electrocardiograms based on the clinical assessment of the patient and the likelihood that a disease is present. At times patients present with significant problems that require urgent treatment that they are unaware of. A good example would be detecting complete heart block on an ECG because of a patient's responses to the cardiovascular review of systems and the fact that an antidepressant was going to be prescribed.
3. To monitor the safety of biological treatments. There is probably no better example than the FDA focus on cardiac conduction and how that can be affected by medications. The most recent warning occurred with citalopram. This antidepressant has been used for over a decade by psychiatrists and was widely considered to be a very safe medication. Both the FDA and the Mayo Clinic have guidelines about how this problem needs to be assessed and that is a combination of clinical assessment and electrocardiograms. In some cases electrocardiograms and referrals to electrophysiologists are required. In light of this information psychiatrists need to have access to these ECGs and a plan to address any abnormalities. As specialists, it is common to see patients who are referred taking doses of citalopram that exceed current FDA guidelines and that may involve testing and a plan to modify the dose of antidepressant.
4. To identify medical emergencies in patients who are being followed for a psychiatric disorder. Many patients who see psychiatrists either do not have primary care physicians or are very reluctant to see them. A psychiatrist in this position needs to make every effort possible to encourage the patient to establish primary care, but even then medical emergencies need to be recognized and appropriately triaged. That can happen more quickly if testing is available to facilitate the referral. If a patient presents with jaundice, medical consultants are more likely to see him quickly if some basic testing is done that can be discussed with the consultant.
5. To identify neurobiological correlates of psychiatric disorders. A common example is an abnormal brain imaging or electrophysiological study that was ordered because of an acute or progressive behavioral change.
6. For heuristic purposes. The classic example of a test done for heuristic purposes was the dexamethasone suppression test. At various times it was suggested as a test for various forms of severe depression and suicide risk. The test is rarely done today because of the false positive errors but it helped generate a couple of decades of research on the neuroendocrinology associated with psychiatric disorders.
Some of the articles currently out there on the internet deny the existence of psychiatric disorders because there is no biological test for these disorders like depression or schizophrenia. That really does not differentiate psychiatric disorders from neurological or rheumatic disorders that may have some supporting markers but that in general depend more on pattern recognition and less on a gold standard or pathognomonic test. From a paper that addresses that subject (1):
"Although the results are often useful, they can be misleading. Few tests yield results that are pathognomonic for particular diseases. For these reasons, test results for autoantibodies alone are insufficient to establish the diagnosis of a systemic rheumatic disease; they must always be interpreted in the clinical context. Positive results for tests such as the ANA test are seen quite commonly in patients with nonrheumatic diseases and even among normal, healthy persons..."
The key sentence here is: "Few tests yield results that are pathognomonic for particular diseases." That would mean that in fact there are few so-called gold standard medical tests that confirm or deny the existence of a diagnosis. Up to 30% of people presenting to a medical clinic for an evaluation of symptoms will never have a diagnosis to explain their symptoms no matter how many tests they have. People with real illnesses often are frustrated by the fact that the test results they get are often equivocal. Obvious conditions that have no biomarkers range from migraine headaches to Alzheimer's Disease. I don't think that any rational person would suggest that neither of these conditions exist. People who have first hand experience with severe mental disorders know that the profound emotional and cognitive changes that they see in their friend of family member is real - whether there is a biomarker or not.
George Dawson, MD, DFAPA
As a backdrop, most people do not understand the concept of "tests" in medicine until they have a problem and realize that the problem is not reflected in the tests ordered by their doctor. That is a very common experience. Some studies show that up to 30% of patients presenting to a clinic for investigation of a symptom never find out what the cause of that symptom was. That is true even after they were given the usual panel of blood tests, imaging studies, and electrophysiological studies. The assumption that symptoms and disorders in medicine are all diagnosable by a "test" is incorrect.
The second problem occurs at the level of test interpretation. When a doctor orders a test they have to interpret it correctly and in many cases the idea of an "abnormal" test is blurred by biological variation. The evaluation of back pain using imaging studies like MRI scans is a good case in point. As people age there is a greater likelihood that an abnormal MRI scan of the spine is not necessarily the cause of their back pain. That has very important implications for treatment and the physician interpreting the test may will definitely be influenced by their specialty training, their own personal experience, their knowledge and examination of the patient, and possibly treatment guidelines that they may be mandated to follow. There is also the question of false positive and false negative testing. The recent controversy about the utility of prostate specific antigen (PSA) testing for prostate cancer is another good example. The current guideline says that this test has too many false positive results to use for treatment planning and further invasive procedures. Even in the case where the diagnosis is made by a specific number there is always the question of whether the test number is accurate or not. I have frequently repeated thyroid function tests that seemed to show hyperthyroidism only to see them in the normal range on repeat testing. It is obvious to physicians that the so-called biological tests in medicine have their limitations and always need to be interpreted in the context of a comprehensive evaluation of the patient.
How are biological tests currently used in psychiatry? It turns out that there are a lot of applications similar to the rest of medicine.
1. To detect a medical cause of a psychiatric disorder. The DSM classification has an entire set of disorders that are caused by underlying neurological illnesses, endocrine disorders, and infectious diseases that need to be recognized and treated. They often present as psychiatric disorders. In my experience of treating people with severe problems, up to 15% of the psychiatric presentations had an underlying medical illness that either was a direct cause of the "psychiatric" symptoms or it made a psychiatric disorder worse. In that case the psychiatrist has to be trained to order the appropriate tests, make the diagnosis and refer the patient for treatment of the underlying disorder.
2. To screen for medical illnesses that complicate the psychiatric disorder or its treatment. A good example here is screening blood tests and electrocardiograms based on the clinical assessment of the patient and the likelihood that a disease is present. At times patients present with significant problems that require urgent treatment that they are unaware of. A good example would be detecting complete heart block on an ECG because of a patient's responses to the cardiovascular review of systems and the fact that an antidepressant was going to be prescribed.
3. To monitor the safety of biological treatments. There is probably no better example than the FDA focus on cardiac conduction and how that can be affected by medications. The most recent warning occurred with citalopram. This antidepressant has been used for over a decade by psychiatrists and was widely considered to be a very safe medication. Both the FDA and the Mayo Clinic have guidelines about how this problem needs to be assessed and that is a combination of clinical assessment and electrocardiograms. In some cases electrocardiograms and referrals to electrophysiologists are required. In light of this information psychiatrists need to have access to these ECGs and a plan to address any abnormalities. As specialists, it is common to see patients who are referred taking doses of citalopram that exceed current FDA guidelines and that may involve testing and a plan to modify the dose of antidepressant.
4. To identify medical emergencies in patients who are being followed for a psychiatric disorder. Many patients who see psychiatrists either do not have primary care physicians or are very reluctant to see them. A psychiatrist in this position needs to make every effort possible to encourage the patient to establish primary care, but even then medical emergencies need to be recognized and appropriately triaged. That can happen more quickly if testing is available to facilitate the referral. If a patient presents with jaundice, medical consultants are more likely to see him quickly if some basic testing is done that can be discussed with the consultant.
5. To identify neurobiological correlates of psychiatric disorders. A common example is an abnormal brain imaging or electrophysiological study that was ordered because of an acute or progressive behavioral change.
6. For heuristic purposes. The classic example of a test done for heuristic purposes was the dexamethasone suppression test. At various times it was suggested as a test for various forms of severe depression and suicide risk. The test is rarely done today because of the false positive errors but it helped generate a couple of decades of research on the neuroendocrinology associated with psychiatric disorders.
Some of the articles currently out there on the internet deny the existence of psychiatric disorders because there is no biological test for these disorders like depression or schizophrenia. That really does not differentiate psychiatric disorders from neurological or rheumatic disorders that may have some supporting markers but that in general depend more on pattern recognition and less on a gold standard or pathognomonic test. From a paper that addresses that subject (1):
"Although the results are often useful, they can be misleading. Few tests yield results that are pathognomonic for particular diseases. For these reasons, test results for autoantibodies alone are insufficient to establish the diagnosis of a systemic rheumatic disease; they must always be interpreted in the clinical context. Positive results for tests such as the ANA test are seen quite commonly in patients with nonrheumatic diseases and even among normal, healthy persons..."
The key sentence here is: "Few tests yield results that are pathognomonic for particular diseases." That would mean that in fact there are few so-called gold standard medical tests that confirm or deny the existence of a diagnosis. Up to 30% of people presenting to a medical clinic for an evaluation of symptoms will never have a diagnosis to explain their symptoms no matter how many tests they have. People with real illnesses often are frustrated by the fact that the test results they get are often equivocal. Obvious conditions that have no biomarkers range from migraine headaches to Alzheimer's Disease. I don't think that any rational person would suggest that neither of these conditions exist. People who have first hand experience with severe mental disorders know that the profound emotional and cognitive changes that they see in their friend of family member is real - whether there is a biomarker or not.
George Dawson, MD, DFAPA
Reference:
1: Arthur Kavanaugh, Russell Tomar, John Reveille, Daniel H. Solomon, Henry A. Homburger; Guidelines for Clinical Use of the Antinuclear Antibody Test and Tests for Specific Autoantibodies to Nuclear Antigens. Arch Pathol Lab Med 1 January 2000; 124 (1): 71–81. doi: https://doi.org/10.5858/2000-124-0071-GFCUOT
Wednesday, May 22, 2013
The Myth of the Psychiatrist as Bogeyman
Probably the most annoying aspect of being a real psychiatrist is the constant attacks on the profession. Psychiatry is unique among medical specialties in that there are a number of philosophies, special interests, critics for profit, and some might say cults out there who generate a constant barrage of criticism of widely varying quality. There are even attacks from within the field. Most medical specialists are concerned primarily with patient care, but that is not true for the self appointed critics of psychiatry who like to attack psychiatry at any possible point in time. In this negative atmosphere - real psychiatrists like me are dedicated to patient care and continue to provide a valued service that has recently been demonstrated to deliver treatment results on par with other medical specialists. Our reason for existence in the negative environment is the sole fact that we will treat severe problems successfully that nobody else will approach. Unique psychiatric training allows us to do that. So how do we explain the incongruence between what real psychiatrists do every day and how they are treated in the media? It is basically a two step process.
The first step is looking at what is said in the media and what it really means. When Senator Grassley began investigating psychiatrists and their relationships to the pharmaceutical industry on a selective basis ignoring other medical specialties despite widespread relationships between other specialists and the pharmaceutical and medical device industry what was the real message there? When the DSM5 is critiqued for being an inaccurate device designed to make as much money for the pharmaceutical industry and organized psychiatry as possible - what is the real message there? When psychiatric diagnosis is described as being totally arbitrary and lacking validity by people who think that validity has something to do with a laboratory test, what is the real message there? Let me translate it for you. It means that psychiatrists are at best totally incompetent and at their worst greedy, dishonest, manipulative, unethical, and interested basically taking money for a worthless diagnostic and treatment exercise that frequently harms people. In other words perpetrating fraud. There is really no way to sugar coat it. If all of the critiques of psychiatry in the media are accurate - that is the only logical conclusion. If you accept that position psychiatry has been devalued as an essentially worthless medical specialty.
The second critical step is to ignore all of the flaws associated with the rest of medicine. Let's forget the fact that 30% of patients entering a medical clinic will not get an adequate explanation for their symptoms even after extensive investigation with those gold standard tests. You know - the tests that mean the diagnosis is "valid". Let's forget that reliability estimates for medical diagnoses - even using those gold standard tests are no better than the so-called poor reliability estimates of psychiatric diagnoses. Let's forget the fact that diagnostic and treatment errors in medicine are common. Let's forget that treatments for medical disorders generally carry a much higher risk of death and complications. Let's forget the fact that patients with factitious disorders get admitted to general hospitals for extended periods of time and pretend that only psychiatrists can't detect a pseudopatient. Let's forget the fact that significant numbers of medical diagnoses are routinely made in the same way that psychiatric diagnoses are made. Let's forget the fact that consensus medical diagnoses by experts are common within all medical specialties. Let's forget the fact that other specialists work for pharmaceutical and medical device companies. Let's forget the fact that many specialty organizations have revenues from industries that easily exceed the revenue stream of the American Psychiatric Association (APA). Let's forget an entire list of imperfections in the practice of medicine and pretend that general medicine is perfect for the sake of comparison with with an imperfect psychiatry. We have succeeded in overidealizing medicine.
That two step dynamic of devaluing psychiatry on a purely arbitrary basis and idealizing the rest of medicine and choosing not to apply the same criticisms that are used in the case of psychiatry is the recipe for the psychiatric bogeyman that you keep reading about in the papers.
If you really believe that there is a psychiatric bogeyman - I have a bridge in Brooklyn that I can sell you.
George Dawson, MD, DFAPA
The first step is looking at what is said in the media and what it really means. When Senator Grassley began investigating psychiatrists and their relationships to the pharmaceutical industry on a selective basis ignoring other medical specialties despite widespread relationships between other specialists and the pharmaceutical and medical device industry what was the real message there? When the DSM5 is critiqued for being an inaccurate device designed to make as much money for the pharmaceutical industry and organized psychiatry as possible - what is the real message there? When psychiatric diagnosis is described as being totally arbitrary and lacking validity by people who think that validity has something to do with a laboratory test, what is the real message there? Let me translate it for you. It means that psychiatrists are at best totally incompetent and at their worst greedy, dishonest, manipulative, unethical, and interested basically taking money for a worthless diagnostic and treatment exercise that frequently harms people. In other words perpetrating fraud. There is really no way to sugar coat it. If all of the critiques of psychiatry in the media are accurate - that is the only logical conclusion. If you accept that position psychiatry has been devalued as an essentially worthless medical specialty.
The second critical step is to ignore all of the flaws associated with the rest of medicine. Let's forget the fact that 30% of patients entering a medical clinic will not get an adequate explanation for their symptoms even after extensive investigation with those gold standard tests. You know - the tests that mean the diagnosis is "valid". Let's forget that reliability estimates for medical diagnoses - even using those gold standard tests are no better than the so-called poor reliability estimates of psychiatric diagnoses. Let's forget the fact that diagnostic and treatment errors in medicine are common. Let's forget that treatments for medical disorders generally carry a much higher risk of death and complications. Let's forget the fact that patients with factitious disorders get admitted to general hospitals for extended periods of time and pretend that only psychiatrists can't detect a pseudopatient. Let's forget the fact that significant numbers of medical diagnoses are routinely made in the same way that psychiatric diagnoses are made. Let's forget the fact that consensus medical diagnoses by experts are common within all medical specialties. Let's forget the fact that other specialists work for pharmaceutical and medical device companies. Let's forget the fact that many specialty organizations have revenues from industries that easily exceed the revenue stream of the American Psychiatric Association (APA). Let's forget an entire list of imperfections in the practice of medicine and pretend that general medicine is perfect for the sake of comparison with with an imperfect psychiatry. We have succeeded in overidealizing medicine.
That two step dynamic of devaluing psychiatry on a purely arbitrary basis and idealizing the rest of medicine and choosing not to apply the same criticisms that are used in the case of psychiatry is the recipe for the psychiatric bogeyman that you keep reading about in the papers.
If you really believe that there is a psychiatric bogeyman - I have a bridge in Brooklyn that I can sell you.
George Dawson, MD, DFAPA
Monday, May 20, 2013
The Latest Proclamation by Allen Frances
Just when you think that Allen Frances has run out of
editorial venues for his anti DSM5 critiques another one pops up. This time it is in the Annals of Internal Medicine.
This is a note about that process before I get into addressing his
repetitive critiques. The Annals is a respected medical
journal. For a number of years I was an
ACP member and subscribed to it myself.
Why would the Annals go along
with publishing an editorial piece that is basically a rehash of what has been
published in the New York Times and
the Huffington blog and who knows
where else? There is really precious
little science involved. I think the
only logical explanation is that the staff of the Annals has jumped on the popular bias against psychiatry that has
been widely noted in the press by Claire Bithell and her group that studies these
issues. I am not a current subscriber
to the Annals but the question is whether
there was equal time for rebuttal. If not is this professional bias against psychiatry?
Probably the best way to address this rehash of old
criticisms is to link up to previous blog posts here where that occurs. Beginning in paragraph one Dr. Frances cites
a famous study about pseudopatients
as though it has some applicability to the issue of “unreliable and inaccurate”
psychiatric diagnosis. He cites this
study as if it is somehow relevant to the problem. All of the considerable scholarship refuting
this study as meaningful by various authors including Spitzer and Kety is
ignored. Using this as a premise for a scholarly
article on the validity of psychiatric diagnosis should raise an eyebrow or
two, but on the other hand I doubt that there is anyone on the editorial board
at this Internal Medicine journal who is familiar with this literature.
The issue of diagnostic inflation is a frequent critique
used by Frances and others to suggest that this invalidates the DSM5. Most people are very surprised to learn that compared
to previous editions and the ICD-10 this is really
not an issue. The previous blog post
illustrates that compared to the ICD-10, the possible increase in diagnostic
categories in the DSM is trivial. The increase in the number of codes for a
knee fracture alone approximates the total codes in the DSM! Contrary to his description of “holding the
line” with DSM-IV diagnoses – the data presented in that post shows that the
DSM-IV added twice as many diagnoses as the DSM5 will.
Dr. Frances uses the “no bright line” approach to say that
there is no way to separate the worried well from people with disorders. There certainly is no written “bright line” in
the DSM. Every DSM has a section with
qualifying statements about its use and that fact that diagnostic criteria
alone are not sufficient. A psychiatric
diagnosis, especially a diagnosis made by psychiatrists in the same group with
the same focus is very consistent and it is a reliable marker of illness
severity. Professional judgment is required. The “no bright line” issue is
not a problem that is unique to psychiatry.
It is omnipresent in general medicine with regard to chronic pain
diagnoses, chronic pain treatment, and in the overprescription of pain
medications and antibiotics. The overprescription of antibiotics has been
identified as a problem by the Centers for Disease Control (CDC) for 20 years
and recent authors suggest that minimal progress has been made. It seems that other specialties are subject to
the “fallible subjective judgments” suggested in this article.
Another implicit myth used by Dr. Frances and other critics
of psychiatry is that there is some magical diagnostic process that occurs in
medicine and surgery that makes them better than psychiatric
diagnoses. What happens when we test
that theory by looking at the reliability of general medical diagnoses? Looking at that data, it is clear that the
published reliability data from medicine and surgery is no better than the frequently criticized data from psychiatry even when objective medical tests are used. Practically everyone I know has a favorite
story about a misdiagnosis and/or ineffective treatment of a medical or
surgical problem. That evidence does not
support the contention that psychiatry is somehow less accurate or effective
than the rest of medicine. Some medical
specialties used similar descriptive techniques even when they have numerous
biological markers of the illness. The
other elephant in the room on this diagnosis issue is medically unexplained
symptoms. The studies of all patients
coming in to a clinic setting suggest that 30% do not get a diagnosis to explain their
symptoms. These patients often get multiple
tests looking for a cause for their problem.
This is by far the most significant problem that I hear from relatives, acquaintances,
and the public in general. If nonpsychiatric
medical diagnoses are supposed to be highly accurate based on biological tests –
a substantial number of people never actually experience that.
On the fuzzy diagnosis in psychiatry critique, a common
theme here is to go after the bereavement exclusion and suggest that normal
bereavement will be treated like depression.
I have an extensive
response to this when it was posted in a newspaper article and invite any
interested reader to look at the previous blog post and the fact that this
approach to grieving patients who come to the attention of psychiatrists has
been written about for over 30 years (see last 5 paragraphs at link). Practically every point in this section of
the editorial can be disputed but the point of the article is not a scientific
review, it is basically a selection of comments to support a specific
viewpoint.
To Dr. Frances credit he references an excellent
meta-analysis by Leucht,
et al on how the results of psychiatric treatment are as good or better
than the results of other medical specialties.
He is silent on how that occurs if psychiatric diagnosis is so unreliable
and inaccurate. How is it possible to
get results that good compared with
other specialties? Maybe it is because
as I have just suggested, the “special problems” in psychiatric diagnosis are
really general problems that are shared by all medical specialists?
The criticism is less focused in the final paragraphs with
some commentary on style points about the DSM political process, the issue of conflict
of interest focused on publishing profits, and the idea that the APA should
submit the DSM to oversight by a broad coalition of “50 mental health
associations”. Let me take the last
point first. There are a number of other
diagnostic approaches and manuals that have
been completed by coalitions of several other mental health organizations. With the number of different approaches, I
would encourage any organization to publish their own approach to the diagnosis
of mental disorders. Contrary to the
rhetoric suggesting that there is a DSM monopoly, nothing could be further from
the truth. The entire text of the World
Health Organization’s (WHO) ICD-10 is available free online. The Mental and Behavioral Disorders section
of the ICD-10 gives detailed descriptions of each disorder. The detailed
research criteria for ICD-10 can be purchased for about ¼ the cost of a DSM5. It seems to me that there is a marketplace of
ideas and plenty of competition. If I
was not a psychiatrist with an interest in reading about developments in my
field, I would not be compelled to purchase a DSM5. I would probably take a few courses in the
changes to DSM-IV and stick with that for a while.
On the issue of submitting the DSM5 to outside groups there
are several compelling reasons why that would not be a good idea for most
psychiatrists. Some critiques
have suggested that psychiatry should be open to forced collaboration by others
based on previous relationships. Over the span of
my career, I have noted that there is often an adversarial
approach by other organizations rather than an affiliative one. And why wouldn’t there be? This is the United States and everyone here
is familiar with the competitive and politicized atmosphere. It seems like that has been left out of the equation
when charges of “conflict of interest” are leveled at the APA in the area of
publishing a DSM. A recent critique of
the DSM5 also suggested broader collaboration with social scientists and I
critique that article here. The political slant of all of these articles
is that the APA needs the input of others to improve descriptive psychiatry. Including that in an article that has a basic
thesis that: “We will be stuck with descriptive psychiatry for the forseeable
future.” (line 27-28) being a negative is inconsistent.
If anything Dr. Frances seems to be suggesting that we should be moving
more to the biomedical side and distancing ourselves from the social scientists. The bottom
line here is that the DSM5 is a diagnostic guideline for psychiatrists to use
in clinical practice. It is not
synonymous with a psychiatric diagnosis and it is used at some level by
psychiatrists to understand mental disorders.
It is not designed for anyone to read and act like a psychiatrist and it
has nothing to do with people who do not have psychiatric problems. It is not a “Bible” like the New York Times
suggests. It is a tool for psychiatrists
and if you are not a psychiatrist there may be no reason for you to buy it or even
think that it is relevant to you.
On the issue of Dr. Frances serial DSM5 critiques - this
seems like a war of attrition to me. Dr. Frances has an infinite number of venues that are quite willing
to publish his very finite and repetitive criticisms of the DSM5 and the
associated process. Outside of myself –
there appears to be nobody else including the American Psychiatric Association who is willing to offer the
obvious counterpoints. He has more time
on his hands and many more connections than I do. So in terms of sheer volume I guess this is a
Pyrrhic victory of sorts. I will have to
be content with expressing the opinion of a psychiatrist who practices real
psychiatry, making diagnoses and helping people every day and knowing that my
results are on par with anybody else in medicine and that there is nothing random about
it.
George Dawson, MD, DFAPA
Saturday, May 18, 2013
Financial Blogger Gets It - Sort Of
I was buoyed to see this line as the title of a financial blog today: "Coming Corporate Control of Medicine Will Throw Patients Under the Bus". You don't usually see that level of insight into what is going on in medicine from financial people who have usually bought the "cost effectiveness" dogma, even at a time where middlemen are siphoning off hundreds of billions of dollars from the direct provision of health care and producing an inferior product. I will say it for the thousandth time - what other industry can make money by selling you a rationed product and denying your access to that product? Can you imagine what the automobile or cell phone market would look like with that guiding principle?
The article is focused on two critical issues-physician management by people with no medical experience and the message from the top. The first part of the article discusses the situation of a pediatrician who had successfully managed a clinic but found herself being managed by a non-physician who told her that she either had to see very complex patients in a shorter period of time or not see them at all. The second part of the article focuses on a blog post where a CEO/physician for a managed care company flat out encourages physicians to get rid of difficult patients to improve their managed care style performance measures.
The blogger in this case is Yves Smith. I have been reading her blog for years. She wrote the book Econned and takes a generally skeptical view of that way that financial markets are regulated and run. I have seen her do commentary on some financial television but infrequently. I would tend to see her commentary as legitimate criticism and welcome in the area of physician and health care management. As a blogger she is highly successful. This post alone has about 40 pages of commentary.
In this article she has some additional comments about what physicians face in the assembly line of today's managed care environment:
"As an aside, it's hard to stress enough that this sort of demoralizing micromanagement an unwillingness to listen and learn from workers is a weird shortcoming of management American style. And it has been weirdly airbrushed out of the media."
I can't agree more with the second comment in particular. The American public gets a glimpse of how their health care management occurs only when Michael Moore makes a movie about it or they are confronted face to face with an impossible situation. That happens all of the time in psychiatry with restrictions on treatment to the point that it seems like treatment has never occurred. To get that accomplished takes both micromanagement of physicians and a general management style that greatly emphasizes profit margin over patients. At the public relations level, physician opinion especially physician dissent is not tolerated. The personal experience of the physicians in these systems is considered the property of the organization. Any public disclosure of the severe shortcomings can be ruthlessly suppressed either by firing or a series of political maneuvers designed to force resignation at some point.
There is a divergence of medical and corporate culture at the level of disclosure of errors or wrongdoing. For most of my professional life I have been in monthly conferences - some type of mortality-morbidity conferences where real or potential errors were discussed on a department wide basis. I don't think that happens in the corporate world. I think that errors in the corporate world are acknowledged if they are widely known and there is an emphasis on public relations and maintaining an almost unrealistic positive light on the company. That has been most evident in the past decade with an abundance of managed care public relations. Wherever I turn it seems like I come across a hospital or clinic that is proclaiming themselves as the "best" - usually in the country. That kind of advertising by physicians was widely viewed as unethical by state medical boards. These ratings are usually based on a few process parameters that can be actively "managed". Contrary to what health care management tells you the quality of any hospital or clinic depends on the quality of the physicians working there and the level of autonomy they have in their medical decision making.
You can have the best surgeons, internists, or psychiatrists in the world and if they are managed to see as many patients as possible and provide the care that will provide the best profit margin for the company - their medical and surgical care will not be appreciably different from a mediocre staff.
I wrote a piece several years ago about an informed approach to managing knowledge workers that originated with management guru Peter Drucker. The details can be found in the original piece in this newsletter (page 3) and a earlier posts on this blog. Everywhere I look in health care we are at the opposite pole from Drucker. Managers are generally far too authoritarian in dealing with physicians especially in cases where (like the Yves Smith blog post) - the mangers know far less than the physicians. This managerial style is also disruptive. Many health care managers think that they can implement any idea they wake up with that morning if they accompany it with enough "Change is good" or "Cost effective" rhetoric. All of this micromanagement and mismanagement illustrates that Dilbert has changed professions. He is currently wearing a white lab coat.
The other bad news of course is that corporate control of medicine is not coming - it has been here for years. In the case of psychiatry it has been here for 30 years. Anyone who wants to see how corporate control of medicine changes things only has to look at the state of current psychiatric services or their "shortage" for a lesson.
George Dawson, MD, DFAPA
The article is focused on two critical issues-physician management by people with no medical experience and the message from the top. The first part of the article discusses the situation of a pediatrician who had successfully managed a clinic but found herself being managed by a non-physician who told her that she either had to see very complex patients in a shorter period of time or not see them at all. The second part of the article focuses on a blog post where a CEO/physician for a managed care company flat out encourages physicians to get rid of difficult patients to improve their managed care style performance measures.
The blogger in this case is Yves Smith. I have been reading her blog for years. She wrote the book Econned and takes a generally skeptical view of that way that financial markets are regulated and run. I have seen her do commentary on some financial television but infrequently. I would tend to see her commentary as legitimate criticism and welcome in the area of physician and health care management. As a blogger she is highly successful. This post alone has about 40 pages of commentary.
In this article she has some additional comments about what physicians face in the assembly line of today's managed care environment:
"As an aside, it's hard to stress enough that this sort of demoralizing micromanagement an unwillingness to listen and learn from workers is a weird shortcoming of management American style. And it has been weirdly airbrushed out of the media."
I can't agree more with the second comment in particular. The American public gets a glimpse of how their health care management occurs only when Michael Moore makes a movie about it or they are confronted face to face with an impossible situation. That happens all of the time in psychiatry with restrictions on treatment to the point that it seems like treatment has never occurred. To get that accomplished takes both micromanagement of physicians and a general management style that greatly emphasizes profit margin over patients. At the public relations level, physician opinion especially physician dissent is not tolerated. The personal experience of the physicians in these systems is considered the property of the organization. Any public disclosure of the severe shortcomings can be ruthlessly suppressed either by firing or a series of political maneuvers designed to force resignation at some point.
There is a divergence of medical and corporate culture at the level of disclosure of errors or wrongdoing. For most of my professional life I have been in monthly conferences - some type of mortality-morbidity conferences where real or potential errors were discussed on a department wide basis. I don't think that happens in the corporate world. I think that errors in the corporate world are acknowledged if they are widely known and there is an emphasis on public relations and maintaining an almost unrealistic positive light on the company. That has been most evident in the past decade with an abundance of managed care public relations. Wherever I turn it seems like I come across a hospital or clinic that is proclaiming themselves as the "best" - usually in the country. That kind of advertising by physicians was widely viewed as unethical by state medical boards. These ratings are usually based on a few process parameters that can be actively "managed". Contrary to what health care management tells you the quality of any hospital or clinic depends on the quality of the physicians working there and the level of autonomy they have in their medical decision making.
You can have the best surgeons, internists, or psychiatrists in the world and if they are managed to see as many patients as possible and provide the care that will provide the best profit margin for the company - their medical and surgical care will not be appreciably different from a mediocre staff.
I wrote a piece several years ago about an informed approach to managing knowledge workers that originated with management guru Peter Drucker. The details can be found in the original piece in this newsletter (page 3) and a earlier posts on this blog. Everywhere I look in health care we are at the opposite pole from Drucker. Managers are generally far too authoritarian in dealing with physicians especially in cases where (like the Yves Smith blog post) - the mangers know far less than the physicians. This managerial style is also disruptive. Many health care managers think that they can implement any idea they wake up with that morning if they accompany it with enough "Change is good" or "Cost effective" rhetoric. All of this micromanagement and mismanagement illustrates that Dilbert has changed professions. He is currently wearing a white lab coat.
The other bad news of course is that corporate control of medicine is not coming - it has been here for years. In the case of psychiatry it has been here for 30 years. Anyone who wants to see how corporate control of medicine changes things only has to look at the state of current psychiatric services or their "shortage" for a lesson.
George Dawson, MD, DFAPA
Saturday, May 11, 2013
The Model of Psychiatric Care for the Future
The Psychiatric News came out with an article yesterday that is critically important for all psychiatrists to read. It reveals the American Psychiatric Association (APA) thinking about the future role of psychiatrists and the model of care that they are promoting. The diagram in this article titled "Integrated Care Relies on Team Approach, Consultant Role for Psychiatrists" is a critical read because it shows what is basically a managed care paradigm for marginalizing psychiatrists. There is is a "BHP/Care Manager" between the psychiatrist and the patient. This is a popular managed care approach to having "care/case managers" making discharge decisions for psychiatrists providing inpatient care. For anyone with professional expertise and direct responsibility to patients it is unacceptable.
The main reason that psychiatry has been marginalized is that all of the knowledge in the membership about what we do and the value we add is ignored in the face of special interest research. The research that forms the "evidence base" for our marginalization in the Psych News article is a good example. There is a long history of similar studies have been published to sell the managed care industry. I can come up with a pharmacoepidemiology study from 20 years ago that show that putting everyone in a primary care clinic on fluoxetine saves money on as many parameters as this article claims for integrated care. Instead of confronting that and saying: "You know psychiatrists do a lot more than that" - the APA seems to accept it and think that integrated care is some big deal. From the diagram it is clear to me that integrated care is just the latest head of the managed care hydra.
The other aspect of the article is the omnipresent "cost savings" rhetoric. Professional organizations have bought this hook line and sinker and seem obliged to include that nonsense in policy about the future of their speciality. The difference of course is that in the last two decades, Cardiology has built out a trillion dollar infrastructure being "cost effective" and we are now treating people in jails who should be in psychiatric hospitals, we have few functional detox facilities and have minimal resources to help disabled patients in the community.
What we need here is a reality based characterization of what psychiatrists do and on average it is a lot more than sitting in a primary care clinic and advising primary care docs about what to do if they can't get their depression ratings (PHQ-9 scores) headed in the right direction. Its is just a matter of time before everybody who thinks they can make a psychiatric diagnosis by reading the DSM will think they can treat depression by reading an algorithm and psychiatry slips off the next managed care diagram. Nobody will realize they just eliminated not just a psychiatrist but the person in the clinic who knew the most Neurology as well.
If we are going to promote any image of ourselves and an image that current trainees can be excited about, it should be a larger than life psychiatric multispeciality clinic and a group of psychiatrists who can cover the gamut of care. That is consistent with the psychiatrist of the future that Thomas Insel, MD has talked about, and it takes a page from some of our specialist colleagues like Radiologists and Anesthesiologists.
They realized a long time ago that you are not going to get a fair deal bartering away your expertise for the sake of doing business.
George Dawson, MD. DFAPA
Mark Moran. Report on Health Care Reform Focuses on Psychiatrists' Role. Psychiatric News May 3, 2013.
Sunday, May 5, 2013
Using A Civil War Law to Intimidate Physicians
I thought I would post this latest iteration of how managed care organizations (MCOs) and their proxies in the pharmacy benefit manager (PBM) industry are intimidating physicians into not prescribing a specific medication for you. At some point these companies started to attach a reference to the False Claims Act, along with the usual forms they expect doctors to fill out so that you can get your prescription filled. Intimidating physicians has always been a tactic to try to slow doctors down or stop them in their tracks. Delaying and stopping doctors from writing prescriptions is money in the pocket of any PBM or MCO. Intimidating physicians is also useful because it has a demonstrated effect on their behavior. It causes them to undercode or bill for less service than they actually provided and it dates back to the 1990s when the FBI was used change the billing behavior of an entire generation of teaching physicians under the threat of large scale paybacks for "fraud" or RICO actions and the threat of imprisonment. I have never seen an estimate of the total amount of money "saved" (as in removed from physicians) and time wasted based on these political ideas, but it would not surprise me if it was hundreds of billions of dollars. I know it forced me not to teach residents for over a decade. I could see no point in needing to generate a daily note that was identical to my residents' notes and they logically found it offensive.
So we have the issue of "prior authorization". You used to get a prescription from your doctor, take it to the pharmacy, and get it filled. In the 1990s HMOs and MCOs decided they knew more than doctors and they would adopt some sweeping measures to "reform" prescribing practices. In some of the areas it made sense at the level of clinic or hospital based Pharmacy and Therapeutics (P&T) Committees. Certain drugs are so specialized (eg. chemotherapy agents) that only certain physicians should prescribe them. There has been a two decades long problem with antibiotic over prescribing and there are typically ongoing initiatives to deal with that problem. I have not been on a P&T Committee for over three years, but I can't imagine there is nothing currently being done to curb opioid painkiller overprescribing. There are definite reasons for intervening with prescribers on a scientific basis. But at some point prior authorization became much more than that and some of the assumptions (like all SSRIs are alike) are not valid. To make matters worse, the pharmacy arm of managed care companies (the PBMs) were now asking for prior authorizations on generic drugs. Or they were asking for repeat authorizations if the prescriber changed or the patient was hospitalized and the prescription stayed the same. These same PBMS found that the same rules did not apply to themselves. They could frequently make deals with hospital that would involve the bundling of one medication with the same medication form the same company and they could make money off that. PBMs had become a multibillion dollar business.
The hassle of filling out forms and making many phone calls in order to assure that a prescription is completed is more than an annoyance. It removes billions of dollars of resources from the provision of medical care. One study estimated that the cost for American physicians to deal with insurance companies was $82,975 per physician or about four times higher than their Canadian counterparts. That amounts to $27.6 billion nationwide. That is a lot of medical care and the time jumping through hoops is never reimbursed by MCOs or PBMs. An estimate of the losses to the treatment side for billing practices alone is about $7 billion.
The political aspects of this intrusion of business into medical practice is instructive. Physicians are notoriously inept when it comes to politics and there is no clearer example than drug prior authorization. What other business in the United States has to provide that level of free work in addition to the primary work in order to be reimbursed. Do other professionals like lawyers need to waste this amount of time? I sat through a meeting at one point where the debate was whether we could influence the length of a drug prior authorization form and get it down to two pages instead of five. The consensus at the time was that there were probably federal rules that would not allow the form to be "streamlined" to two pages!
So now we have the streamlined form with a 14 page federal statute affixed to it. Reading through the statute and figuring out what it means takes an attorney. But every doctor who sees this knows what it means. Don't rock the boat. Don't question this government backed, big business policy that is guaranteed to waste your time and put more money into the pocket of the insurance industry. And by the way, there is no guarantee that your patient will get the medication that you think they need, even if you jump through all of these hoops.
That is the state of health care in America today and it may be why you are standing in a pharmacy waiting to get your prescription filled. It also may be why your doctor looks exhausted.
George Dawson, MD, DFAPA
Morra D, Nicholson S, Levinson W, Gans DN, Hammons T, Casalino LP. US physician practices versus Canadians: spending nearly four times as much money interacting with payers. Health Aff (Millwood). 2011 Aug;30(8):1443-50. doi: 10.1377/hlthaff.2010.0893. Epub 2011 Aug 3. PubMed PMID: 21813866.
So we have the issue of "prior authorization". You used to get a prescription from your doctor, take it to the pharmacy, and get it filled. In the 1990s HMOs and MCOs decided they knew more than doctors and they would adopt some sweeping measures to "reform" prescribing practices. In some of the areas it made sense at the level of clinic or hospital based Pharmacy and Therapeutics (P&T) Committees. Certain drugs are so specialized (eg. chemotherapy agents) that only certain physicians should prescribe them. There has been a two decades long problem with antibiotic over prescribing and there are typically ongoing initiatives to deal with that problem. I have not been on a P&T Committee for over three years, but I can't imagine there is nothing currently being done to curb opioid painkiller overprescribing. There are definite reasons for intervening with prescribers on a scientific basis. But at some point prior authorization became much more than that and some of the assumptions (like all SSRIs are alike) are not valid. To make matters worse, the pharmacy arm of managed care companies (the PBMs) were now asking for prior authorizations on generic drugs. Or they were asking for repeat authorizations if the prescriber changed or the patient was hospitalized and the prescription stayed the same. These same PBMS found that the same rules did not apply to themselves. They could frequently make deals with hospital that would involve the bundling of one medication with the same medication form the same company and they could make money off that. PBMs had become a multibillion dollar business.
The hassle of filling out forms and making many phone calls in order to assure that a prescription is completed is more than an annoyance. It removes billions of dollars of resources from the provision of medical care. One study estimated that the cost for American physicians to deal with insurance companies was $82,975 per physician or about four times higher than their Canadian counterparts. That amounts to $27.6 billion nationwide. That is a lot of medical care and the time jumping through hoops is never reimbursed by MCOs or PBMs. An estimate of the losses to the treatment side for billing practices alone is about $7 billion.
The political aspects of this intrusion of business into medical practice is instructive. Physicians are notoriously inept when it comes to politics and there is no clearer example than drug prior authorization. What other business in the United States has to provide that level of free work in addition to the primary work in order to be reimbursed. Do other professionals like lawyers need to waste this amount of time? I sat through a meeting at one point where the debate was whether we could influence the length of a drug prior authorization form and get it down to two pages instead of five. The consensus at the time was that there were probably federal rules that would not allow the form to be "streamlined" to two pages!
So now we have the streamlined form with a 14 page federal statute affixed to it. Reading through the statute and figuring out what it means takes an attorney. But every doctor who sees this knows what it means. Don't rock the boat. Don't question this government backed, big business policy that is guaranteed to waste your time and put more money into the pocket of the insurance industry. And by the way, there is no guarantee that your patient will get the medication that you think they need, even if you jump through all of these hoops.
That is the state of health care in America today and it may be why you are standing in a pharmacy waiting to get your prescription filled. It also may be why your doctor looks exhausted.
George Dawson, MD, DFAPA
Morra D, Nicholson S, Levinson W, Gans DN, Hammons T, Casalino LP. US physician practices versus Canadians: spending nearly four times as much money interacting with payers. Health Aff (Millwood). 2011 Aug;30(8):1443-50. doi: 10.1377/hlthaff.2010.0893. Epub 2011 Aug 3. PubMed PMID: 21813866.
Even more DSM bashing - is it a fever pitch yet?
Just when you think you have seen it all, you run into an article like this one in The Atlantic. A psychotherapist with a long antipsychiatry monologue. It is written in interview format with psychotherapist Gary Greenberg as the discussant. I thought it was interesting because the title describes this diatribe as the "real problems" with psychiatry. Of course what he writes about has nothing to do with the real problems that specifically are the rationing and decimation of psychiatric services by managed care companies and the government. The entire article can be discredited on a point by point basis but I will focus on a few broad brush strokes.
The author here spins a tale that the entire impetus for a diagnostic manual and a biomedical orientation for psychiatry is strictly political in nature and it has to do with wanting to establish credibility with the rest of medicine. That is quite a revision of history. Psychiatry pretty much exists now because psychiatrists would take care of the problems that nobody else wanted to. I have immediate credibility when another physician is seeing a person with a mental illness, they don't know what to do about it, and I do. It is less clear today, but psychiatry professional organizations were asylum focused and the goal was to treat people in asylums initially and then figure out a way to get them back home. Part of the psychiatric nosology was based on the people who would get out of asylums at some point and those who did not. The credibility of psychiatry has nothing to do with a diagnostic manual. It has to do with the fact that psychiatrists have a history of treating people with serious problems and helping them get well. There is no discussion of how the numbers of people institutionalized in the 1950s and 1960s fell to the levels of current European levels as a result of psychiatric intervention that included the use of new medications but also a community psychiatry movement that was socially based. (see Harcourt Figure II.2)
The author uses the idea of "chemical imbalance" rhetorically here as further proof that psychiatrists are using a false premise for political purposes. He presumes to tell his readers that during the time he is giving the interview there is some psychiatrist out there using the term chemical imbalance to convince a patient to take antidepressants. Since I have never used that term and generally discourage it when patients bring it up, I wonder if he is right. Any psychiatrist trained in the past three decades knows the situation is much more complex than that. Eric Kandel describes the situation very well in his 1979 classic article on "Psychotherapy and the Single Synapse". Any antipsychiatrist using "chemical imbalance" against psychiatry in a rhetorical manner suggests that there is no biomedical basis for mental disorders. There should be nobody out here who believes that is true and in fact this article acknowledges that.
The basic position here is to deny that anything psychiatric exists. Psychiatrists don't know what they are doing. Psychiatrists are driven by the conflict of interest that nets them "hundreds of millions of dollars". He doesn't mention how much money he makes as an outspoken critic of psychiatry. He tries to outflank his rhetoric by suggesting any psychiatrists who disagrees with him and suggests that it is typical antipsychiatry jargon is "diagnosing him". He doesn't mention the fact that antipsychiatry movements are studied and classified by philosophers.
I think the most revealing part of this "interview" is that it appears to be orchestrated to enhance the author's rhetoric. The evidence for that is the question about "drapetomania" and implying that has something to do with coming up with DSM diagnoses and the decision to drop homosexuality as a diagnostic category. That is more than a stretch that is a clear distortion and of course the question is where the interviewer comes up with a question about "drapetomania". I wonder how that happened?
This column is an excellent ad for the author's antipsychiatry work. Apart from that it contains contains the standard "chemical imbalance" and psychiatric disorders are not "real illnesses". To that he adds the conflicting positions of saying there appear to be biological correlates of mental disorders but they would never correlate with an existing diagnosis and the idea of a chemical imbalance metaphor is nonsense. He uses colorful language to boost his rhetoric: "They'll (those wacky psychiatrists - my clarification) bob and weave, talk about the "living document," and unleash their line of bullshit."
His conclusory paragraph and the idea to "take the thing (DSM) away from them" has been a common refrain from the DSM critics. In fact as I have repeatedly pointed out, there is nothing to stop any other organization from coming up with a competing document. In fact, sitting on my shelf right now (next to DSM-IV) is a reference called the Psychodynamic Diagnostic Manual. It is listed as a collaborative effort of six different organizations of mental health professionals. It was published 12 years after the last edition of the DSM - it is newer. I have texts written by several of the collaborators of this volume. When I talk with psychiatrists from the east coast, they frequently ask me about whether or not I am familiar with the volume. My point here is that if the author's contentions about the reality basis of DSM diagnoses are correct, it should be very easy to come up with a different system. I encourage anyone or group of people to develop their own diagnostic system and compete with the DSM.
So the last minute attacks on psychiatry with the release of the DSM seem to be at a fever pitch. The myth of the psychiatric bogeyman is alive and well. Add The Atlantic to the list of uncritical critics of psychiatry.
George Dawson, MD, DFAPA
1. Hope Reese. The Real Problems with Psychiatry. The Atlantic. May 2, 2013.
2. Bernard E. Harcourt. From the asylum to the prison: rethinking the incarceration revolution. The Law School, University of Chicago, 2007.
3. Psychodynamic Diagnostic Manual (PDM). A collaborative effort of the American Psychoanalytic Association, International Psychoanalytic Association, Division of Psychoanalysis (38) of the American Psychological Association, American Academy of Psychoanalysis and Dynamic Psychiatry, National Membership Committee on Psychoanalysis in Clinical Social Work. Published by the Alliance of Psychoanalytic Organizations. Silver Spring, MD (2006).
4. Kandel ER. Psychotherapy and the single synapse. The impact of psychiatric thought on neurobiologic research. N Engl J Med. 1979 Nov 8;301(19):1028-37. PubMed PMID: 40128.
The author here spins a tale that the entire impetus for a diagnostic manual and a biomedical orientation for psychiatry is strictly political in nature and it has to do with wanting to establish credibility with the rest of medicine. That is quite a revision of history. Psychiatry pretty much exists now because psychiatrists would take care of the problems that nobody else wanted to. I have immediate credibility when another physician is seeing a person with a mental illness, they don't know what to do about it, and I do. It is less clear today, but psychiatry professional organizations were asylum focused and the goal was to treat people in asylums initially and then figure out a way to get them back home. Part of the psychiatric nosology was based on the people who would get out of asylums at some point and those who did not. The credibility of psychiatry has nothing to do with a diagnostic manual. It has to do with the fact that psychiatrists have a history of treating people with serious problems and helping them get well. There is no discussion of how the numbers of people institutionalized in the 1950s and 1960s fell to the levels of current European levels as a result of psychiatric intervention that included the use of new medications but also a community psychiatry movement that was socially based. (see Harcourt Figure II.2)
The author uses the idea of "chemical imbalance" rhetorically here as further proof that psychiatrists are using a false premise for political purposes. He presumes to tell his readers that during the time he is giving the interview there is some psychiatrist out there using the term chemical imbalance to convince a patient to take antidepressants. Since I have never used that term and generally discourage it when patients bring it up, I wonder if he is right. Any psychiatrist trained in the past three decades knows the situation is much more complex than that. Eric Kandel describes the situation very well in his 1979 classic article on "Psychotherapy and the Single Synapse". Any antipsychiatrist using "chemical imbalance" against psychiatry in a rhetorical manner suggests that there is no biomedical basis for mental disorders. There should be nobody out here who believes that is true and in fact this article acknowledges that.
The basic position here is to deny that anything psychiatric exists. Psychiatrists don't know what they are doing. Psychiatrists are driven by the conflict of interest that nets them "hundreds of millions of dollars". He doesn't mention how much money he makes as an outspoken critic of psychiatry. He tries to outflank his rhetoric by suggesting any psychiatrists who disagrees with him and suggests that it is typical antipsychiatry jargon is "diagnosing him". He doesn't mention the fact that antipsychiatry movements are studied and classified by philosophers.
I think the most revealing part of this "interview" is that it appears to be orchestrated to enhance the author's rhetoric. The evidence for that is the question about "drapetomania" and implying that has something to do with coming up with DSM diagnoses and the decision to drop homosexuality as a diagnostic category. That is more than a stretch that is a clear distortion and of course the question is where the interviewer comes up with a question about "drapetomania". I wonder how that happened?
This column is an excellent ad for the author's antipsychiatry work. Apart from that it contains contains the standard "chemical imbalance" and psychiatric disorders are not "real illnesses". To that he adds the conflicting positions of saying there appear to be biological correlates of mental disorders but they would never correlate with an existing diagnosis and the idea of a chemical imbalance metaphor is nonsense. He uses colorful language to boost his rhetoric: "They'll (those wacky psychiatrists - my clarification) bob and weave, talk about the "living document," and unleash their line of bullshit."
His conclusory paragraph and the idea to "take the thing (DSM) away from them" has been a common refrain from the DSM critics. In fact as I have repeatedly pointed out, there is nothing to stop any other organization from coming up with a competing document. In fact, sitting on my shelf right now (next to DSM-IV) is a reference called the Psychodynamic Diagnostic Manual. It is listed as a collaborative effort of six different organizations of mental health professionals. It was published 12 years after the last edition of the DSM - it is newer. I have texts written by several of the collaborators of this volume. When I talk with psychiatrists from the east coast, they frequently ask me about whether or not I am familiar with the volume. My point here is that if the author's contentions about the reality basis of DSM diagnoses are correct, it should be very easy to come up with a different system. I encourage anyone or group of people to develop their own diagnostic system and compete with the DSM.
So the last minute attacks on psychiatry with the release of the DSM seem to be at a fever pitch. The myth of the psychiatric bogeyman is alive and well. Add The Atlantic to the list of uncritical critics of psychiatry.
George Dawson, MD, DFAPA
1. Hope Reese. The Real Problems with Psychiatry. The Atlantic. May 2, 2013.
2. Bernard E. Harcourt. From the asylum to the prison: rethinking the incarceration revolution. The Law School, University of Chicago, 2007.
3. Psychodynamic Diagnostic Manual (PDM). A collaborative effort of the American Psychoanalytic Association, International Psychoanalytic Association, Division of Psychoanalysis (38) of the American Psychological Association, American Academy of Psychoanalysis and Dynamic Psychiatry, National Membership Committee on Psychoanalysis in Clinical Social Work. Published by the Alliance of Psychoanalytic Organizations. Silver Spring, MD (2006).
4. Kandel ER. Psychotherapy and the single synapse. The impact of psychiatric thought on neurobiologic research. N Engl J Med. 1979 Nov 8;301(19):1028-37. PubMed PMID: 40128.
Friday, May 3, 2013
Greyhound Therapy - suddenly wrong?
Without any disrespect to the famous long haul bus company, I wanted to comment on this story posted from the APA's Facebook feed. It is a story about a man, James Brown who was discharged unchanged from a psychiatric hospital in the state of Nevada and sent to California via bus with minimal resources. That was the discharge plan. Watch the actual clip to see what happened and watch the concerned discussion by the public official in this case. Diane Sawyer, et al were outraged. How could this possibly happen? How often does this happen? There was a happy ending to this story but how often does it go horribly wrong?
When I looked at this clip I was amazed for a couple of reasons. First off, it was on the APA's Facebook feed with a comment by the Medical Director. Without going into all of the details that I have posted so far on this blog, I will say that it is about time and leave it at that. The fact that nothing has been said to this point is also reflected in my second point and that is - this has been going on for over 20 years! Every place in this country with a major psychiatric hospital has been the recipient or point of origin for discharges by bus to another state. It is so common that I used to refer to it as Greyhound Therapy with my coworkers and everybody knew exactly what I was talking about.
At first blush putting somebody with a severe mental illness on a bus and sending them to another state - sometimes across a number of states seems inhumane. In some cases, the person himself may insist but if we are talking about the instance where the person is mentally ill and cannot care for themselves - I agree completely. It is inhumane and not really ethical from the standpoint of a physician. So how does it occur?
It basically occurs by taking a business approach to psychiatry. Rationing and cost center management coalesce into the perfect mechanism to get people out of psychiatric hospitals when they are at their most vulnerable. I have posted many times the concept of getting people out of the hospital before the hospital loses money on a DRG payment. That is generally within 3 - 5 days. That period of time is well below any acceptable time period necessary for the evaluation or treatment of severe psychiatric problems. Everyone agrees that hospital treatment like outpatient treatment means treating people with medications and in hospitals the medications are generally added faster and at much larger doses than in outpatient settings. Five days does not allow for any changes if there are side effects or inadequate treatment response or comorbid medical complications that may crop up. So doctors don't want to use this approach. Who does?
The main drivers are managed care companies and the government agencies that promote these tactics. So the psychiatrist doesn't want to discharge the patient in 5 days - get a managed care reviewer to say that the hospital stay is no longer "medically necessary" and will not be paid for. If the attending psychiatrist doesn't like that decision - he or she can appeal it to another reviewer within the same company. How do you think that will turn out? Of course you can always appeal to the state - right? The state has managed care rights embedded in their statutes. The appeal goes through a commission that is often staffed by insurance industry insiders and they are not there to advocate for patients or their physicians. In the case of psychiatrists who are unfortunate enough to work for managed care companies, they may find their discharge decisions commandeered by case managers and a medical director whose only jobs are to get people out of the hospital as soon as possible. Disagree with them and you might hear that the medical director will come down and take over discharging the patient. Or you might find yourself fighting a never ending series of political battles for not being a "team player." The discharge team may decide to do an end run around you entirely and that could involve putting somebody on a bus.
What about the psychiatrists working in these settings? Why don't they ever speak up? It should be obvious from the preceding paragraph that it could result in getting fired or forced out in one way or another. Every organization these days has policies that stifle disclosure from physicians working in those companies. All of the communication needs to go though an administrator who has the company's best interest at heart. The interest of the patient, the physician, and the physician-patient relationship is not a priority. Making money is the priority or in the case of health care, being "cost-effective".
We have a perfectly corrupted system of hospital care for people with severe mental illnesses. Businesses and governments can essentially do what they want. Many of these settings are so miserable that good psychiatrists avoid them. Patients churn in and out often with no changes or changes that are so abrupt that they are immediately rehospitalized.
There is a solution that can have immediate impact and potentially lead to reform. I applaud James Brown in this case for disclosing what happened to him and elegantly stating what he was deprived of. On the other hand, nobody should have to forfeit their confidentiality and talk about what continues to be a stigmatizing illness just because business friendly systems predictably fail to provide quality medical care and marginalize medical decisions. A whistleblower statute that protects any psychiatrist who reports that their patient was discharged against their recommendations and given a bus ticket is a quick solution. It should also apply when a managed care company is insisting that an unstable patient be discharged when they remain at high risk or have not been evaluated or treated. The ABC story here suggests that these discharged patients may be "dangerous to themselves or others". In fact, the majority of these cases are very vulnerable people who need help and protection. That help and protection is not coming from a government set up to protect the managed care industry and those forces that ration care for the mentally ill.
George Dawson, MD, DFAPA
ABC News. Man with Psychosis Recalls Nevada 'Patient Dumping'.
When I looked at this clip I was amazed for a couple of reasons. First off, it was on the APA's Facebook feed with a comment by the Medical Director. Without going into all of the details that I have posted so far on this blog, I will say that it is about time and leave it at that. The fact that nothing has been said to this point is also reflected in my second point and that is - this has been going on for over 20 years! Every place in this country with a major psychiatric hospital has been the recipient or point of origin for discharges by bus to another state. It is so common that I used to refer to it as Greyhound Therapy with my coworkers and everybody knew exactly what I was talking about.
At first blush putting somebody with a severe mental illness on a bus and sending them to another state - sometimes across a number of states seems inhumane. In some cases, the person himself may insist but if we are talking about the instance where the person is mentally ill and cannot care for themselves - I agree completely. It is inhumane and not really ethical from the standpoint of a physician. So how does it occur?
It basically occurs by taking a business approach to psychiatry. Rationing and cost center management coalesce into the perfect mechanism to get people out of psychiatric hospitals when they are at their most vulnerable. I have posted many times the concept of getting people out of the hospital before the hospital loses money on a DRG payment. That is generally within 3 - 5 days. That period of time is well below any acceptable time period necessary for the evaluation or treatment of severe psychiatric problems. Everyone agrees that hospital treatment like outpatient treatment means treating people with medications and in hospitals the medications are generally added faster and at much larger doses than in outpatient settings. Five days does not allow for any changes if there are side effects or inadequate treatment response or comorbid medical complications that may crop up. So doctors don't want to use this approach. Who does?
The main drivers are managed care companies and the government agencies that promote these tactics. So the psychiatrist doesn't want to discharge the patient in 5 days - get a managed care reviewer to say that the hospital stay is no longer "medically necessary" and will not be paid for. If the attending psychiatrist doesn't like that decision - he or she can appeal it to another reviewer within the same company. How do you think that will turn out? Of course you can always appeal to the state - right? The state has managed care rights embedded in their statutes. The appeal goes through a commission that is often staffed by insurance industry insiders and they are not there to advocate for patients or their physicians. In the case of psychiatrists who are unfortunate enough to work for managed care companies, they may find their discharge decisions commandeered by case managers and a medical director whose only jobs are to get people out of the hospital as soon as possible. Disagree with them and you might hear that the medical director will come down and take over discharging the patient. Or you might find yourself fighting a never ending series of political battles for not being a "team player." The discharge team may decide to do an end run around you entirely and that could involve putting somebody on a bus.
What about the psychiatrists working in these settings? Why don't they ever speak up? It should be obvious from the preceding paragraph that it could result in getting fired or forced out in one way or another. Every organization these days has policies that stifle disclosure from physicians working in those companies. All of the communication needs to go though an administrator who has the company's best interest at heart. The interest of the patient, the physician, and the physician-patient relationship is not a priority. Making money is the priority or in the case of health care, being "cost-effective".
We have a perfectly corrupted system of hospital care for people with severe mental illnesses. Businesses and governments can essentially do what they want. Many of these settings are so miserable that good psychiatrists avoid them. Patients churn in and out often with no changes or changes that are so abrupt that they are immediately rehospitalized.
There is a solution that can have immediate impact and potentially lead to reform. I applaud James Brown in this case for disclosing what happened to him and elegantly stating what he was deprived of. On the other hand, nobody should have to forfeit their confidentiality and talk about what continues to be a stigmatizing illness just because business friendly systems predictably fail to provide quality medical care and marginalize medical decisions. A whistleblower statute that protects any psychiatrist who reports that their patient was discharged against their recommendations and given a bus ticket is a quick solution. It should also apply when a managed care company is insisting that an unstable patient be discharged when they remain at high risk or have not been evaluated or treated. The ABC story here suggests that these discharged patients may be "dangerous to themselves or others". In fact, the majority of these cases are very vulnerable people who need help and protection. That help and protection is not coming from a government set up to protect the managed care industry and those forces that ration care for the mentally ill.
George Dawson, MD, DFAPA
ABC News. Man with Psychosis Recalls Nevada 'Patient Dumping'.
Wednesday, May 1, 2013
Nature Takes A Shot at DSM5 – Spectrums Only Get You So Far
"The Catholic Church changes its pope more often than the APA publishes a new DSM." (reference 1)
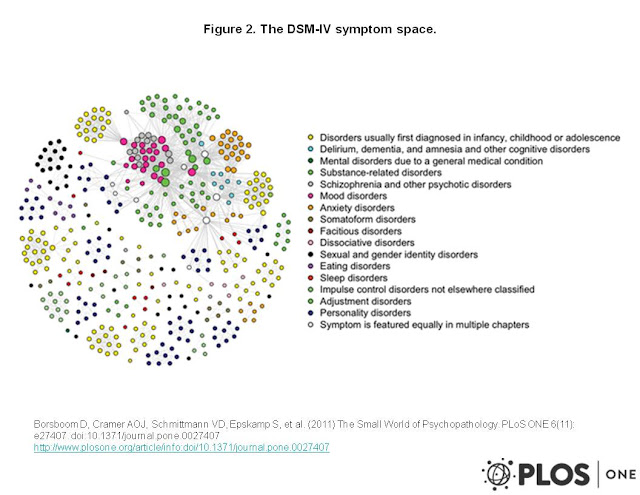
I was disappointed to see another shot at the DSM, this time
on my Nature Facebook feed. I suppose with the impending release it is a
chance to jump on the publicity bandwagon.
I will jump over numerous errors in the first paragraph (David Kupfer – modern
day heretic?!) and get to the main argument.
The author in this case makes it seem like seeing psychopathological
traits on a spectrum
is somehow earth shaking news and yet another reason to trash a modest
diagnostic manual designed by psychiatrists to be used as a part of psychiatric
diagnostic process.
In evaluating this article the first question is the whole
notion of continuums. The idea has
been there for a long time and this is nothing new. Just looking at some DSM-IV major category
criteria like major depression, dysthymia, and mania and just counting symptoms
using combinatorics you get the following possibilities:
Major depression - 20 C 5 = 15,504
Manic episode - 15 C 3 = 455
Dysthymia - 2 C 10 = 45
Mixed - 20 C 5 + 15 C 3 = 15,959
That means if you are following the DSM classification and
looking just at the suggested diagnostic combinations you will be seeing
something like 16,004 combinations of mood symptoms just based on a categorical
classification. Superimposed reality can
expand that number by several factors right up to the point that you have a
patient who cannot be categorically diagnosed. If you add all Axis II
conditions with mood sx - there is another large expansion in the number of
combinations. The sheer number of combinations possible should suggest at
some point that the discrete categories give way to a frequency
distribution. The only problem of course
(and this is lost or ignored by all managed care and political systems) the
clinician is treating an individual patient with certain problems and not
addressing the entire spectrum of possibilities. The other reality is that if you put a point anywhere on the spectrum including the Nature blog's mental retardation-autism-schizophrenia-schizoaffective disorder-bipolar and unipolar disorder spectrum - you essentially have a categorical diagnosis.
In a recent article, Borsboom,
et al use a graphing approach to show the relationship between the 522
criteria (simplified to 439 symptoms) of 201 distinct disorders in the
DSM-IV. The authors demonstrate that
these symptoms are highly clustered relative to a random graph and go on to
suggest that their network model currently account for the variance in genetics,
neuroscience, and etiology in the study of mental disorders. Their figure below is reproduced in accordance with the Creative Commons 3.0 license. (click to enlarge).

For the example given
by the author’s example – schizophrenia with obsessive traits, we still need to
make that characterization in order to proceed with treatment. The diagnostic categories “schizophrenia”
and “obsessive compulsive disorder” and “obsessive compulsive personality
disorder” are still operative. What does
saying that there is a “continuum” or “spectrum disorder” add? In initial evaluations psychiatrists are
still all looking for markers of all of the major diagnostic categories and
listing everything that they find. The
treatment plan needs to be a cooperative effort between the psychiatrist and
patient to treat the problems that are affecting function and leading to
impairment. The idea that there will be
a magical genetic and brain imaging test that will result in a “proper clinical
assessment” at this point is a pipe dream rather than a potential product of a
diagnostic manual. The limitations of the spectrum approach are also evident in this article that points out the failed field trials attempting to use a dimensional approach for personality disorders.
George Dawson, MD, DFAPA
1. Adam D. Mental health: On the spectrum. Nature. 2013 Apr
25;496(7446):416-8. doi: 10.1038/496416a. PubMed PMID: 23619674
2. Borsboom D, Cramer AO, Schmittmann VD, Epskamp S, Waldorp
LJ. The small world of psychopathology. PLoS One. 2011;6(11):e27407. doi: 10.1371/journal.pone.0027407.
Epub 2011 Nov 17. PubMed PMID: 22114671
Subscribe to:
Posts (Atom)